
Abstract
Progressive colorectal cancer frequently presents with various manifestations, including hepatic, pulmonary, and peritoneal metastases, as well as local and anastomotic site recurrences. However, pancreatic metastasis is extremely rare. Complete surgical resection is currently considered the most effective and only potentially curative treatment for colorectal cancer with distant metastases. We report the successful laparoscopic treatment of a patient with pancreatic metastasis after initial surgery for Stage IV sigmoid colon cancer with pulmonary metastasis. An 84-year-old man was initially diagnosed with sigmoid colon cancer and pulmonary metastasis. Laparoscopic sigmoidectomy and thoracoscopic partial resection of the right lung were performed in 2017. After 8 months, an approximately 20-mm tumor was detected in the pancreatic tail during imaging investigations. We performed laparoscopic distal pancreatectomy without lymph node dissection at 1 year after the initial operation. The histopathological findings suggested metachronous pancreatic metastasis from the sigmoid colon cancer. The patient has had an uneventful postoperative course with no signs of recurrent disease during 29 months of follow-up after the pancreatic surgery. After prior surgery for Stage IV sigmoid colon cancer with pulmonary metastasis, curative resection was performed for pancreatic metastasis. We believe that curative resection may be useful for pancreatic tumors that involve hematogenous metastasis.
Introduction
Curative resection is not indicated for distant hepatic metastases arising from multiple types of carcinomas. However, surgical resection has recently been considered effective for hepatic and pulmonary metastasis arising from colorectal cancer. Hepatectomy is recommended for curable hepatic metastases by the Japanese Society for Cancer of the Colon and Rectum 2019 guidelines for the treatment of colorectal cancer. However, few reports have addressed surgical resection of colorectal cancer metastasis to other organs beyond the liver and lungs. In particular, there is little evidence to support the usefulness of surgery for pancreatic metastasis from colorectal cancer, and further studies and case accumulation are needed to address this issue. We report a case of successful laparoscopic resection of pancreatic metastasis from colorectal cancer, with the patient remaining alive and free from recurrence at 29 months after the operation.
Case Presentation
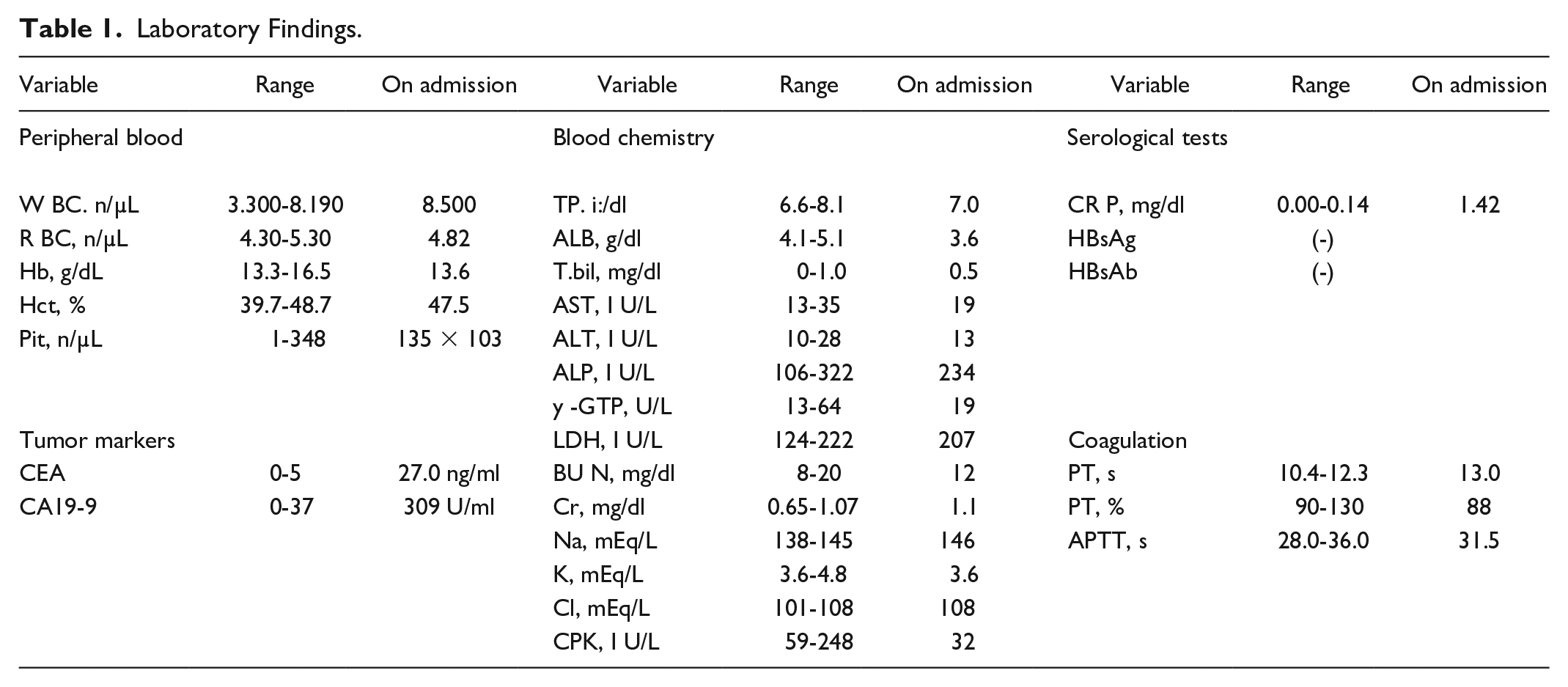
An 84-year-old man was referred to our hospital because of bloody stools. He had a history of diabetes mellitus for the last 50 years, for which he was taking medication. His family history was unremarkable. The laboratory findings were as follows: hematocrit: 47.5%, platelets: 135 × 103 /μL, serum aspartate aminotransferase: 19 IU/L (normal: <35 IU/L), serum alanine aminotransferase: 13 IU/L (normal: <28 IU/L), bilirubin: 0.5 mg/dL (normal: <1.0 mg/dL), albumin: 3.6 mg/dL, and prothrombin time: 88%. Screening for hepatitis B and C revealed negative findings. The serum carcinoembryonic antigen concentration was 27.0 ng/mL (normal: <5.0 ng/mL) and the serum carbohydrate antigen 19-9 concentration was 309 mAU/mL (normal: <40 mAU/mL) (Table 1). Total colonoscopy revealed three-quarters of a Type 2 tumor in the sigmoid colon that was approximately 30 cm from the anal verge. Tumor biopsy revealed well and moderately differentiated adenocarcinoma, which led to a diagnosis of sigmoid colon cancer. Laparoscopic sigmoidectomy was performed for sigmoid colon cancer in July 2017. Histological examination revealed that the tumor was a well and moderately differentiated adenocarcinoma with invasion into the subserosa (T3) and no regional lymph node metastases (N0). In October of the same year, a right pulmonary nodule was discovered and treated using thoracoscopic partial resection of the right lung (pM1a [PUL1] and pStage Ⅳa).
Laboratory Findings.
At 8 months after the initial operation, the carcinoembryonic antigen concentration increased to 27 ng/mL and positron emission tomography revealed fluorodeoxyglucose accumulation in the tail of the pancreas. Enhanced computed tomography also revealed an approximately 20-mm ischemic mass in the tail of the pancreas (Figure 1). Abdominal magnetic resonance imaging revealed an approximately 20-mm space-occupying lesion in the tail of the pancreas, with a low T1-weighted signal and slightly high T2-weighted signal (Figures 2a and 2a). Fluorodeoxyglucose-positron emission tomography confirmed fluorodeoxyglucose accumulation (maximum standardized uptake value: 5.58 early, 6.91 late), which was consistent with the mass in the pancreatic tail (Figure 3). Endoscopic ultrasound-guided fine needle aspiration biopsy revealed numerous atypical cells with only nucleoli, which were indicative of adenocarcinoma cells (Figure 4). Based on those findings, the lesion was diagnosed as a solitary metastatic pancreatic tumor and we decided to perform surgery while keeping in mind the possibility of primary pancreatic cancer.

Enhanced computed tomography revealed an approximately 20-mm ischemic mass in the tail of the pancreas (arrow).

Abdominal magnetic resonance imaging revealed (a) an approximately 20-mm space-occupying lesion in the tail of the pancreas with a low T1-weighted signal (arrow) and (b) a slightly higher T2-weighted signal.

Positron emission tomography-computed tomography revealed fluorodeoxyglucose accumulation, which was consistent with the mass in the pancreatic tail.

Endoscopic ultrasound revealed a space-occupying lesion in the pancreatic tail (arrow), and fine needle aspiration revealed many atypical.
Laparoscopic pancreatectomy was performed at approximately 1 year after the initial operation. No splenic lymph node metastasis or distant metastases were observed macroscopically or based on the preoperative imaging, and the spleen was preserved. The specimen exhibited hyperplasia of high columnar atypical glandular epithelium, which is a hallmark of adenocarcinoma. Immunohistochemical staining revealed no expression of CK7, CK20 expression, and CDX-2 expression (Figure 5). Therefore, the final diagnosis was metachronous pancreatic metastasis from sigmoid colon cancer.

Histopathological findings from the resected specimen revealed (a) hyperplasia of high columnar atypical glandular epithelium (H&E staining), which is typical of adenocarcinoma. Immunohistochemical staining revealed no CK7 expression (b), CK20 expression (c), and CDX-2 expression (d).
The postoperative course was uneventful, and the patient was discharged on the 11th postoperative day. No adjuvant chemotherapy was administered, and the patient remains alive and free from recurrence after 29 months of follow-up.
Discussion
The Japanese Society for Cancer of the Colon and Rectum estimates that the incidences of the first recurrence after curative resection of rectal cancer are 7.1% for hepatic metastasis, 5.5% for pulmonary metastasis, 2.0% for peritoneal metastasis, 2.0% for local recurrence, 1.1% for the anastomotic site, and 4.8% for other sites. 1 The liver is a frequent site of distant metastasis and recurrence of colorectal cancer, while the incidence of pancreatic metastasis is extremely low (approximately 1.7%). Most carcinomas as distant metastases are observed in the terminal stages of malignant tumors with multiple organ metastases or peritoneal dissemination, and are not considered amenable to radical treatment. However, radical treatment can frequently be performed for colorectal cancer, even in cases that involve hepatic metastases, and this treatment strategy greatly affects the patient’s prognosis. Nevertheless, surgical resection of pancreatic metastasis after surgery for colorectal cancer is very rare.2-7 The metastatic routes to the pancreas include (1) continuous spread from nearby organs, (2) invasion into the pancreatic parenchyma via lymphatic metastasis to the peripancreatic lymph nodes, (3) cancerous peritonitis, and (4) hematogenous metastasis. In our case, the diagnosis was hematogenous metastasis because no lymph node metastasis was observed for the primary and metastatic lesions. Moreover, lymphatic invasion was ruled out during the pathological examination, and pulmonary metastasis was also observed.
Hepatic and lung metastases, which are representative of hematogenous metastases, have been reported to have 5-year survival rates of 35% to 58%3,4,8 and 30% to 68%9-11 after curative resection. Lymph node dissection is not necessary and resection of only the metastatic lesions is considered sufficiently curative. Similarly, in cases involving surgery for pancreatic metastasis, lymph node dissection is not considered necessary for hematogenous metastasis because metastases to peripancreatic lymph nodes are rare. In 4 cases reported in Japan, 12 where the prognosis after pancreatectomy was clear, only 2 patients with no metastases to the peripancreatic lymph nodes died and the median survival time was 21 months (range: 1–156 months).
Nevertheless, there have been reports of cases that involved lymph node metastasis. If lymphatic metastasis is suspected because of positive lymphatic invasion or lymph node metastasis at the site of the primary lesion, or if suspected metastatic lymph nodes are observed before or during surgery, local resection combined with lymph node dissection should be performed. The median survival time for patients with positive pancreatic lymph node metastasis is as short as 16 months (range: 2-57 months), which reflects a poor prognosis.
Numerous clinical trials have examined adjuvant treatments for colorectal cancer. Randomized trials in Europe and the US have shown that the combination of 5-fluorouracil plus leucovorin and oxaliplatin (FOLFOX and CapeOX) suppresses recurrence and increases survival time, which indicates that postoperative adjuvant therapy is useful for Stage III colorectal cancer. 13 However, the use of adjuvant chemotherapy for Stage IV colorectal cancer remains controversial, as it is clearly more advanced and has a higher risk of recurrence. Therefore, several clinical trials have examined the effectiveness of perioperative chemotherapy for suppressing recurrence in Stage IV patients. One study 13 compared postoperative 5-fluorouracil/leucovorin therapy after hepatectomy to hepatectomy alone for Stage IV colorectal cancer with hepatic metastasis, and another integrated analysis 14 combined data from the European Organization for Research and Treatment of Cancer/National Cancer Institute of Canada Clinical Trials Group/Gruppo Italiano di Valutazione Interventi in Oncologia trial and the Fédération Francophone de Cancérologie Digestive Trial 9002. The results showed that recurrence-free survival was prolonged in the adjuvant chemotherapy group, although overall survival did not change. In recent years, there have even been reports of shorter overall survival in the adjuvant chemotherapy group. 15 Thus, we elected to perform follow-up without adjuvant chemotherapy after the radical surgery, and the patient remains alive and without any recurrence at 29 months after the first surgery.
The guidelines for the treatment of colorectal cancer 1 recommend resection of hematogenous metastases if they are deemed resectable. However, further cases are needed to evaluate this strategy. In our case, because the pancreatic tumor was discovered after surgery for colorectal cancer, we considered the possibility of hematogenous metastasis from colorectal cancer to the pancreas. Thus, we performed a detailed whole-body search and carefully examined the surgical specimens for evidence of distant metastases. Our results suggest that curative resection of the metastasis may improve the patient’s prognosis.
Conclusion
After initial surgery for Stage IV sigmoid colon cancer with pulmonary metastasis, curative resection was successfully performed for pancreatic metastasis. We believe that curative resection may be useful for pancreatic tumors that involve hematogenous metastasis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The patient provided informed consent and the report was approved by the appropriate ethics review board.
Informed Consent
Verbal informed consent was obtained from a legally authorized representatives for anonymized patient information to be published in this article.