
Abstract
Relapsing polychondritis (RP) is a rare and, if not treated, potentially lethal autoimmune disorder. Involvement of central nervous system (CNS) in RP is rare and, when present, makes it extremely difficult to diagnose. In this report, we present a case of a 22-year-old Hispanic woman who presented with sudden onset of headache and blurred vision. Magnetic resonance imaging (MRI) of her brain and orbit showed leptomeningeal enhancements in addition to asymmetrical thickening and enhancement of globes. Her lumbar puncture was consistent with aseptic meningitis picture, and she was placed on empirical treatment for presumptive CNS tuberculosis. Her vision deteriorated, and she was diagnosed with RP with CNS and ocular involvement and placed on high-dose steroids with dramatic rapid response. She has been on immunosuppressive treatment, including Sulfasalazine and Methotrexate, since then and her disease has been under control with decreased need for ophthalmic steroid drops. There have been only 19 previous cases found in literature reporting an association of RP with CNS involvement.
Introduction
Relapsing polychondritis (RP) is a rare autoimmune disease that is characterized by inflammation of cartilaginous tissue, affecting particularly the ears, nose, respiratory tract, eyes, and joints. 1 Most common presentation includes unilateral or bilateral inflammation of the external ear. This autoimmune disease affects 3.5 per 1 million people each year. Neurological involvement in RP is present approximately in 3% of cases with most common involvement of cranial neuropathies of the second, sixth, seventh, and eight nerves. Other clinical manifestations previously reported are stroke, meningoencephalitis, polyneuritis, and dementia. 2 The presence of meningoencephalitis is a very rare neurological manifestation of RP, making the diagnosis extremely difficult for it is often missed or unrecognized for months to years. In this case report, a 22-year-old Hispanic woman with RP-related chorioretinitis and central nervous system (CNS) involvement manifested by decreased visual acuity and headache is presented.
Case Presentation
A 22-year-old Hispanic woman was in her usual state of health until she developed severe headache (8 of 10 scale) and blurred vision for last 5 days. She was seen at the ophthalmology clinic with marked reduction in vision of her right eye more than left that slowly progressed over 5 days. The patient reported this progressive loss of vision was interfering with her daily activities. She denied flashes of light and floaters in either eye. Her visual acuity examination showed right eye 20/70 and left eye 20/200. Her intraocular pressures and examination of conjunctivae, corneas, anterior chamber, and irises were within normal limits. The examination of posterior chamber after dilation revealed congestion of optic nerves and prepapilledema. There was subretinal fluid beneath the maculae and surrounding the optic nerves. Due to initial diagnosis of serous chorioretinopathy and its underlying differential diagnosis of autoimmune, infectious, carcinomatous, or paraneoplastic conditions and with coexistence of headache, she was sent to the hospital for evaluation. Upon admission, magnetic resonance imaging (MRI) of brain with contrast revealed generalized leptomeningeal enhancement with “sugar-coating” or “zuckerguss pattern” in her vermis region of cerebellum (Figures 1 and 2). Her orbital MRI showed increased signal thickening at the posterior aspect of globes and focal enhancements (Figure 3). Lumbar puncture showed an opening pressure of 150 mm H2O, glucose 58 (normal range: 40-75) mg/dL, protein 46 (normal range: 15-45) mg/dL, WBC (white blood cell) 180 cells/μL, RBC (red blood cell) count 25, lymphocytes 96%, neutrophils 3%, and macrophages 1%.

MRI brain T1 post contrast showing leptomeningeal enhancement.

MRI brain T1 post contrast showing “sugar coating” or “zuckerguss pattern.”

MR Orbit T1 post contrast showing increased signal thickening at the posterior aspect of globes and focal enhancements worse on left.
She was started on empirical antifungal and antituberculosis medications due to the chronic aseptic meningitis picture. In the next following 15 days, she did not improve clinically and instead developed new symptoms. Her new symptoms included tinnitus in left ear, vertigo, hyperacusis, photophobia, retroorbital pain, and loss of color perception. She underwent 3 additional lumbar punctures to rule out increased intracranial pressure with similar cerebrospinal fluid (CSF) findings (Table 1). Comprehensive workup (Table 2) was unrevealing; therefore, her antifungal treatment was stopped.
CSF Panel.
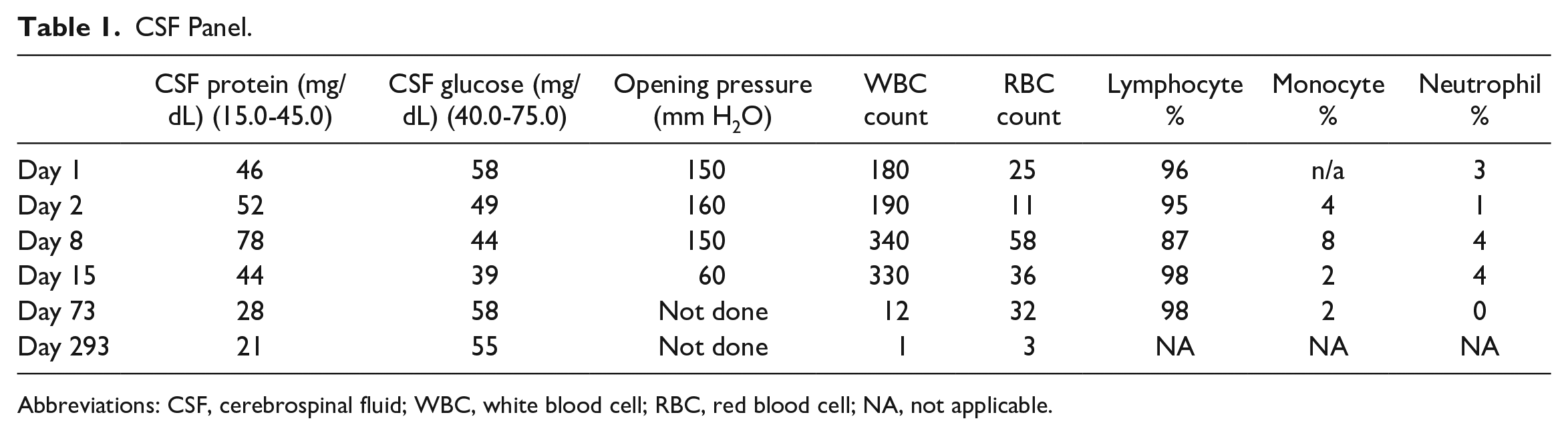
Abbreviations: CSF, cerebrospinal fluid; WBC, white blood cell; RBC, red blood cell; NA, not applicable.
Cerebrospinal Fluid and Serum Workup.

Abbreviations: AFB, acid-fast bacteria; ACE, angiotensin-converting enzyme; PCR, polymerase chain reaction; HSV, herpes simplex virus; LCMV, Lymphocytic Choriomeningitis virus; MTB Comp, Mycobacterium tuberculosis complex; VDRL, venereal disease research laboratory; ANA, antinuclear antibody; IFA, indirect immunofluorescence assay; CCP, cyclic citrullinated peptide; CRP, C-reactive protein; FTA-ABS, fluorescent treponemal antibody absorption; HIV, human immunodeficiency virus; PTT-LA, Partial Thromboplastin Time - Lupus Anticoagulant; DRVVT, Dilute Russell viper venom time; RPR, Rapid Plasma Reagin; Cocci, coccidioidomycosis; Immunodiff, Immunodiffusion; IgG, immunoglobulin G; IgM, immunoglobulin M; Ag, antigen; Ab, antibody; Hep, hepatitis; Surf, surface; TB, tuberculosis; Sm, Smith; RNP, ribonucleoprotein antibody; TSI, thyroid stimulating immunoglobulins.
Upon further detail intake of her medical history, it was found that she had an episode of epistaxis accompanied with nasal cartilage inflammation and nasal septal deviation in the past. She has complained of rib cage pain on multiple occasions and also endorsed joint stiffness and pain involving her hands and back in the past. Her chest x-ray (CXR) and hand x-rays were unremarkable. The thoracic spine x-ray revealed moderate degenerative arthritis. Her mother disclosed to have a known diagnosis of seronegative rheumatoid arthritis and it was always a fear that she had passed it to her daughter. She also mentioned that she sought medical evaluation for her daughter at the age of 12 but never followed up thereafter. On further examination, she was found to have thinning of bilateral pinna without erythema. She met the criteria and diagnosis of RP with chorioretinitis and CNS involvement. She was initiated on pulse therapy with high dose of methylprednisolone 1000 mg for 3 days. During her pulse therapy and following days after, her visual acuity improved, color vision returned, and vertigo and hyperacusis resolved.
Her multidisciplinary team decided to complete 12 months of empirical tuberculosis treatment and she was discharged on prednisone 60 mg daily with plan to slowly taper and move to steroid-sparing immunosuppression. Follow-up lumbar punctures showed significant improvement (Table 1). Her follow-up brain MRI also showed resolution of leptomeningeal enhancement and sugar-coating enhancements in her vermis. Since then, over the last 3 years she has been followed up in ophthalmology and rheumatology clinics. She also underwent several minor relapses of her chorioretinitis without CNS involvement. She is currently responding to sulfasalazine, methotrexate, and ophthalmic steroid drops.
Discussion
Currently in literature, there are only 19 previously reported cases of RP with CNS involvement. Neurological involvement is an extremely rare complication in RP which occurs in only 3% of patients. Among the previous 19 cases, the average age of the patients was 56 years. What makes our case even more unique is that till date there have been no cases reported in literature in which the patient was below the age of 30 years. 3 There is a report published of 13 men and 6 women showing a slight male predominance. The diagnostic criteria established so far for RP are known as the McAdam criteria (Table 3), which require the existence of 3 or more clinical findings. 4 These criteria were later modified, adding the presence of at least 1 McAdam criterion and positive histological confirmation, or 2 McAdam criteria and positive response to administration of corticosteroids or dapsone. 5 In our case, the patient experienced ocular inflammation, vestibular/cochlear dysfunction, and polyarthralgia and had a positive response to corticosteroids, thereby satisfying the McAdam diagnostic criteria for RP. The patient’s complaint of costochondral pain is typical of RP. Furthermore, the patient had moderate degenerative arthritis of vertebral spine which was unusual for her age. Vertebral column involvement in RP is rare, and only 1 case has been reported thus far. 6 Onset of RP manifestations for most patients include dizziness, arthralgia, fever, weight loss, and fatigue. However, patients with RP complicated by CNS involvement are notorious to present with fever, headache, and signs of meningeal irritation. 7 In our case, although the patient did not present with any fever throughout her hospitalization, she had continuous prolonged headaches.
Diagnostic Criteria of Relapsing Polychondritis, According to Different Authors.

Pleocytosis was present in all 19 reported cases among patients except for one. Mononuclear cell predominance in CSF was seen in literature presenting in 13 of the 19 cases, along with polymorphonuclear leukocytes. However, all cases in conjunction with ours displayed high levels of CSF protein.7,10 Our case along with others showed increased opening pressure of CSF. It seems that pleocytosis, increased opening pressure, and high level of protein in CSF are common characteristics of aseptic meningitis of RP. However, these findings have a spectrum of differential diagnosis, and a complete workup is needed to exclude other conditions (Table 2). It is also reported that RP patients may have a false-positive venereal disease research laboratory test. 1
Along with clinical evaluation and laboratory tests, it is recommended that the workup include MRI imaging as it can aid in identifying CNS lesions. Shen et al reported a case of aseptic meningitis in RP in which MRI imaging showed obvious thickened and enhanced meninges on T1-weighted sequence. 11 Ota et al showed a slight thickening of the dura matter in patient with similar diagnosis. 12 This fits alongside our case which presented with increased abnormal meningeal enhancement, primarily in cerebellar vermis region. Most reported cases showed thickening of the meninges in RP with CNS involvement; therefore, it is believed that this positive radiological finding is commonly present in RP patients presenting with involvement of the CNS. It is believed that this common radiological finding is present in CNS involvement in RP patients.
There are currently no evidence-based guidelines for the treatment of RP related to CNS involvement due to its rarity and variety of clinical presentations. The pharmacological approach is mainly based on previous literature. Corticosteroids are currently being used as the primary treatment for all reported cases and have shown to result in improvement and resolution of clinical symptoms. Oral prednisone is usually initiated with a dose ranging from 0.25 to 1 mg/kg daily; reducing or increasing the dose is varied depending on severity of patients’ symptoms. In the literature, it is shown that 16 of the 19 patients, along with ours, showed an overall good response rate to corticosteroid therapy. However, due to the risk of relapse, it is highly recommended to continue steroid therapy long term; thus, commonly other drugs along with corticosteroid therapy are initiated to avoid complications of end organ failure or other life-threatening diseases. Other drugs include cyclophosphamide (1 mg/kg/day for 2 weeks increasing dose by 25 mg every 2 weeks), azathioprine (2 mg/kg/day), cyclosporine (5 mg/kg/day), and methotrexate (15-25 mg/week orally). 5 In 2012, biological agents, including anti-TNF (tumor necrosis factor) agent (infliximab), opened new perspectives for patients resistant to classical immunosuppressive treatments. 13 In our case, administration of prednisone initially resulted in improvement of our patient’s headache and vision. However, the patient experienced multiple episodes of relapse with ocular inflammation and arthralgia during the periods of steroid taper. With the addition of sulfasalazine, followed by methotrexate, her symptoms were under better control with fewer relapses. Of note, sulfasalazine was used first because the patient was concerned about the teratogenic side effect of methotrexate. However, when her symptoms were not as well controlled with steroid eye drops and sulfasalazine 500 mg twice daily, she agreed to add methotrexate. She also was educated and complied with contraceptive use. Our case illustrates that sulfasalazine may not be as effective as methotrexate in treating RP.
Conclusion
This case report highlighted the rarity and uniqueness of CNS involvement secondary to RP, along with explanation of this very easily misdiagnosed condition. Thorough clinical assessment, exclusion of other infectious diseases, and radiological imaging comprehensively lead to the appropriate diagnosis. Corticosteroids and immunosuppressive agents are found to serve as the best form of treatment, yet it is recommended that each case be individualized.
Footnotes
Acknowledgements
This case was orally presented at the American Federation for Medical Research (January 2019), Carmel, CA, USA. This case was also presented at Kern Medical Research Forum (2020) Bakersfield, CA, USA.
Disclaimer
Views expressed in this article are our own and do not the official position of the institutions listed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval to report this case was obtained from the Kern Medical Institutional Review Board (Approval ID: 20031).
Informed Consent
Informed consent for patient information to be published in this article was obtained.