
Abstract
The present study reports the clinical data of a patient with small cell lung cancer who developed relapsing polychondritis. We report a case of a 57-year-old female presented with cough, expectoration, and fever. A Computed Tomography (CT) scan performed at the hospital revealed diffuse thickening of bronchial walls in both lungs. Bronchoscopy revealed that the tracheal mucosa was thickened, narrowed, and collapsed, and the bronchoscope could pass through. The bronchial mucosa on both sides was thickened and edematous, the surface was rough, each bronchus was narrow, and the intervertebral ridges were widened. Needle biopsy: considering small cell carcinoma in combination with immunohistochemical results. Her symptom was not improved after anti-infective therapy. The left auricle was red and swollen, the auricle collapsed, and the left eye had subconjunctival hemorrhage during her hospitalization without obvious cause. After multidisciplinary consultation, pulmonary small cell lung cancer cT0N2Mx rumen lymph node metastasis and RP were considered. Treatment: Prednisone, orally for RP. Chemotherapy combined with radiotherapy was given for small cell lung cancer. The chemotherapy regimen was carboplatin combined with etoposide. The patient has already been followed for 1 year after receiving chemoradiotherapy; the condition of the patient is stable at present. Based on the case of our patient, for cases of RP with symptoms such as auricle chondritis, ocular inflammatory disease, and nasal chondritis, we should pay great attention to whether the case is caused by lung cancer with relapsing polychondritis. Because of the rarity of the disease, the clinician should improve the recognition of the disease in order to strive for early diagnosis and therapy.
Introduction
Relapsing polychondritis (RP) is a rare disease. RP is a non-infectious autoimmune inflammatory disease mainly involving cartilage and connective tissue, including auricular cartilage, nose, larynx, and trachea, which results in tracheal stenosis in the cauliflower ear, saddle nose, and larynx. Moreover, conjunctiva and sclera can also be involved, with a recurrent disease course. Its clinical manifestations are diverse, and auricular chondritis is the most common clinical manifestation. 1 Some patients with this disease present symptoms such as fever, local pain, fatigue, and weakness. Although the cause of RP is still unknown, an autoimmune etiology is thought to be closely involved. Due to the immune dysfunction of patients, it causes abnormal cellular and humoral immunity, thus attacking their own cartilage tissue, resulting in the destruction of cartilage structure and other protein-rich tissues.2,3 Its histopathological feature is chondrolysis with perichondritis. Inflammatory cell infiltration is observed in the cartilage at the initial stage, followed by chondrocyte destruction. The cartilage matrix is necrotic and dissolved, and granulation tissue is appeared. Finally, the residual cartilage tissue disappears, with fibrillation of granulation tissue, contraction of scar, and collapsed and deformed tissue. 4
Lung cancer refers to primary malignant tumors in the trachea, bronchi, and lungs. Lung cancer is a bronchogenic carcinoma, including several major types: squamous carcinoma, adenocarcinoma, small cell carcinoma, and large cell carcinoma. Lung cancer is often asymptomatic in the early stages, and some patients may present with cough and blood-stained sputum. The extrapulmonary symptoms of lung cancer are mainly manifested by extrapulmonary metastasis such as bone metastasis and bone pain, and paraneoplastic syndrome.
By referring to a large number of references, it is unclear whether there is a direct relationship between RP incidence and lung cancer, or whether RP is an extrapulmonary paraneoplastic syndrome of lung cancer.
Case
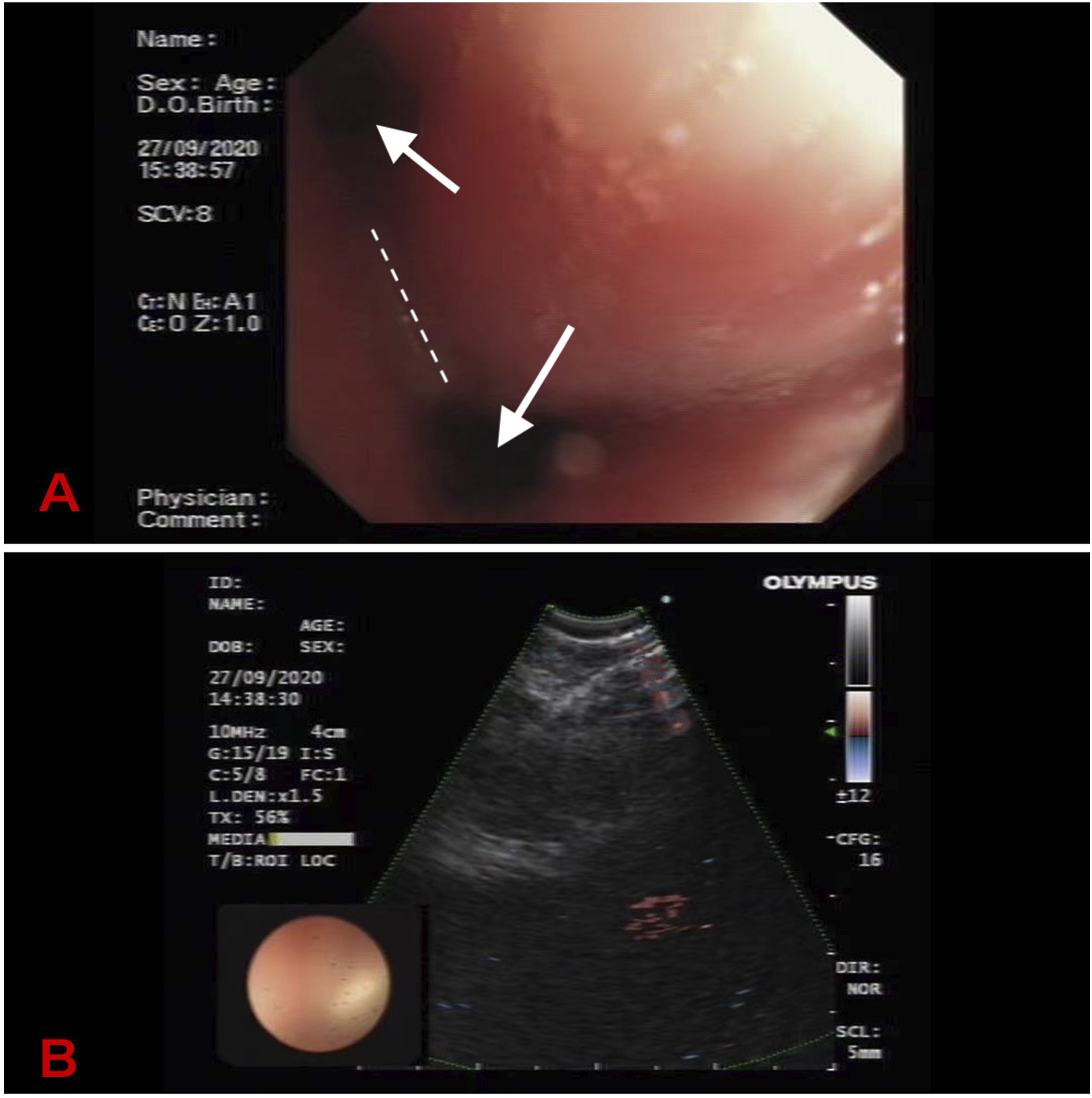
A 57-year-old female patient was admitted into the Department of Respiratory Medicine of Dalian Central Hospital on 25 September 2020 due to “repeated cough and expectoration for 4 months and aggravation for 25 days.” Four months ago, the patient had cough and expectoration with white sputum after upper respiratory tract infection (cold), about 5–7 spats/day, accompanied by shortness of breath, and occasional dyspnea. The patient orally took anti-inflammatory and cough drugs (details unknown) at home, but the effect was poor. Twenty-five days ago, the above symptoms were aggravated, accompanied by intermittent fever of body temperature, with self-measured body temperature up to 37.8°C, without cooling treatment. The patient was admitted to the Department of Respiratory Medicine of Zhongshan Hospital, Dalian University for treatment of 1 week, and the etiology was not clear. The patient was diagnosed with pulmonary lesions of unknown nature, and perfected with the following relevant examinations: on 21 September 2020, Novel Coronary test in Zhongshan Hospital Affiliated to Dalian University showed negative; blood routine: C-reactive protein (CRP): 76.69 mg/L (0–10) and serum amyloid A (SAA): 303.31 mg/L (0–10); the remaining tumor markers, urine and stool routine, blood lipid, D-dimer, coagulation, thyroid function, renal function, electrolytes, myocardial enzymes, troponin, and hepatitis virus series showed no significant abnormalities. Computed Tomography (CT) + enhancement revealed: diffuse thickening of the bronchial wall (see Figure 1(a)). Pulmonary function showed FVC 58.6% predicted, FEV1 35.6% predicted, and FEV1/FVC 80.70%, and mixed ventilatory dysfunction was mainly obstructive type, combined with severe dysfunction of small airway function, mildly reduced diffusion capacity, and negative for bronchodilator test. The symptoms were not significantly relieved after anti-infective treatment (details unknown). During hospitalization, the patient developed left auricle redness, swelling, pain, and ocular congestion due to “excessive internal heat,” and was diagnosed with erysipelas and herpes zoster in the left ear by dermatology consultation. The patient was given symptomatic treatment (famciclovir 250 mg 3 times a day orally, Qingpeng ointment, Cortex phellodendri liquid for external application twice daily, and Bear Bile Scutellaria Eye Drops 5–6 times/day), after which the symptoms were slightly better. The patient was admitted to the Department of Respiratory Medicine of Dalian Central Hospital for further definite diagnosis and treatment on 25 September 2020. The patient had no smoking history. On admission, his temperature was 36.2°C, pulse 74 beats per minute, respiratory rate 20 breaths per minute, and blood pressure 120/90 mmHg. The consciousness was clear, the lips were not cyanotic, the superficial lymph nodes were not significantly enlarged, the left auricle was red and swollen, the auricle collapsed, the left eye had subconjunctival hemorrhage, no dry or wet rales were heard, and no pleural friction rub was heard. The heart rhythm was regular, no murmur was heard in any of the auscultatory valve areas, the liver and spleen were not large, and there was no edema in both lower limbs. Other relevant examinations were perfected: C-reactive protein 25.50 mg/L (0–8), and the remaining rheumatic autoimmune series and blood routine, urine routine, and erythrocyte sedimentation rate at the time of bleeding and coagulation were normal. Superficial lymph nodes showed no abnormal enlarged lymph nodes on ultrasound. Bronchoscopy revealed that the tracheal mucosa was thickened, narrowed, and collapsed, and the bronchoscope could pass through. The bronchial mucosa on both sides was thickened and edematous, the surface was rough, each bronchus was narrow, and the intervertebral ridges were widened. Mucosal biopsies were taken from the lower lobe of the right lung and the upper and lower interlobar ridges of the left lung. The ruminal lymph nodes and right hilar lymph nodes were explored by replacing the ultrasound endoscope, and 3 shots were given for each of the two groups of lesions under ultrasound guidance for histological and cytological examination (see Figure 2). Needle biopsy: a small amount of atypical cells were observed, considering small cell carcinoma in combination with immunohistochemical results. Immunohistochemically: CK (paranuclear foci +), TTF-1 (+), CD56 (+), Syn (weak +), CgA (−), Ki-67 (+60%), NapsinA (−), and P40 (−). (Upper and lower interlobar ridges of the left lung) biopsy: chronic inflammation. (Right hilar lymph node) needle biopsy: no definite atypical cells were seen. Immunohistochemically: CK (−). (Right lower interlobar ridge) biopsy: chronic inflammation and active focal epithelial hyperplasia, please combine with clinical findings. Special staining: acid-fast staining (−), methenamine silver (−), and PAS (−) (see Figure 3). Ear lesions consultation by otolaryngology department: examination: auricular congestion and slight swelling in the left ear, no obvious tenderness, no abnormality of external auditory canal and tympanic membrane, no congestion, and swelling of auricle in the right ear; electroaudiometry: acoustic deafness in both ears; acoustic immittance: AS type map in both ears; preliminary diagnosis: perichondritis in the auricle of the left ear, acoustic deafness in both ears, squeezing the auricle was prohibited, and nutritional nerve vasodilator therapy was recommended. Ophthalmology consultation was requested for subconjunctival congestion, considering subconjunctival hemorrhage in the left eye, and attention was paid to blood routine and bleeding and coagulation. Rheumatology and immunology consultation was requested in combination with the above symptoms, considering the possibility of RP. After multidisciplinary consultation, pulmonary small cell lung cancer cT0N2Mx rumen lymph node metastasis and RP were considered. Treatment: prednisone, 12 tablets, 60 mg, once a day, orally for RP. Chemotherapy combined with radiotherapy was given for small cell lung cancer. The chemotherapy regimen was carboplatin combined with etoposide (carboplatin 397mgD1 and etoposide 0.156gD1-D3) for 6 cycles. Chest CT retest was performed on 20 February 2021 during chemotherapy period and no evidence of tumor progression showed (see Figure 1(b)). Local radiotherapy was performed on submediastinal metastatic lymph nodes and adjacent lymph node areas as well as tracheal bulge and corresponding thickened tracheal wall areas from 2021.03.29 to 2021.04.29. Conventional fractionation of the irradiation dose of 54 Gy/30 F GTV and 45 Gy/25 F CTV was given. The patient’s condition gradually stabilized after the above treatment. Repeat abdominal CT showed no clear signs of tumor metastasis, and brain MRI examination showed no signs of tumor metastasis. Contrast-enhanced CT of the chest showed no evidence of tumor progression showed (see Figure 1(c)). (a) Lung CT revealed: diffuse thickening of the bronchial wall. (b) CT showed the no tumor progression compared with that before. (c) CT showed no progression compared with that before. CT: Computed Tomography. (a) Bronchoscopy revealed that the bronchial mucosa on both sides was thickened and edematous, the surface was rough, each bronchus was narrow (see arrows), and the intervertebral ridges were widened(see dotted line). (b)Ultrasound endoscope: puncture the ruminal and right hilar lymph nodes. (A) (staining, H&E; magnification, ×4) needle biopsy: atypical cells. (b) (staining, H&E; magnification, ×200) needle biopsy: a small amount of atypical cells were observed. (c) Immunohistochemically (magnification, ×200): CK (+). (d) Immunohistochemically (magnification, ×200): TTF-1 (+). (e) Immunohistochemically (magnification, ×200): CD56 (+). (f) Immunohistochemically (magnification, ×200): Ki-67 (+60%).The yellow particles in the arrows in C-F are cancer cells, where the protein expression is positive. Considering small cell carcinoma in combination with immunohistochemical results.

The patient was followed up for nearly 1 year, and was in stable condition at present without obvious auricular redness, swelling, pain, or conjunctival congestion.
Discussion
In recent years, lung cancer has been the most prevalent malignant tumor in China, and has become the leading cause of cancer death and threatening human life. 5 Most patients have no obvious clinical symptoms in the early stage of lung cancer, and some patients present with cough, expectoration, hemoptysis, dyspnea, chest pain, and other discomfort symptoms. A few patients present extrapulmonary symptoms. The extrapulmonary symptoms of lung cancer are mainly manifestations of extrapulmonary metastasis such as bone pain in bone metastases, liver pain in liver metastases, gastrointestinal symptoms, and manifestations of paraneoplastic syndromes such as cachexia, acropachy, acanthosis nigricans, Cushing’s syndrome, and hypercalcemia. However, cases presenting relapsing polychondritis (RP) are very rare.
In 1960, Pearson et al. used the term “relapsing polychondritis” to describe a series of 12 cases that presented with clinical features that were characteristic of the disease. 1 RP is a disease involving multiple systems throughout the body, 1 with recurrent progressive inflammatory destructive lesions, which can involve cartilage and other connective tissues, including the ears, nose, eyes, joints, and respiratory tract. Clinical manifestations are more common in ear, nose, and respiratory chondroinflammation with ocular involvement symptoms. 6 In this case, the patient had recurrent symptoms of left auricular redness and swelling, auricular collapse, and subconjunctival hemorrhage in the left eye, which were consistent with the common symptoms of the disease reported in the literature.
Imaging findings such as lung CT show thickening and calcification of the tracheal and bronchial walls, stenosis and deformation, enlarged mediastinal lymph nodes, and inflammatory infiltration of the bronchi and lobules.7,8,9 In this case, the patient developed diffuse thickening of bronchial wall, bronchitis changes. In this case, it was compatible with the imaging findings reported in the previous literature.
Bronchoscopy can be used to directly observe the affected airway and to show the degree of tracheobronchitis, deformation, and collapse, with erythema, edema, granuloma-like changes, or atrophy of the mucosa seen; moreover, cartilage ring destructing shows airway collapse, and by taking a biopsy under the microscope, it helps to confirm the diagnosis. 10 Bronchoscopy in this case revealed that the tracheal mucosa was thickened, narrowed, and collapsed. The bronchial mucosa on both sides was thickened and edematous, the surface was rough, each bronchus was narrow, and the intervertebral ridges were widened. The patient was diagnosed with small cell lung cancer based on pathological examination.
The pathogenesis of RP was not clear. Some scholars believe that RP is associated with mesoderm dyssynthesis or abnormal proteolytic enzymes. Studies have shown that immune-mediate may be the key to pathogenesis. RP is an autoimmune reaction produced by the body mainly against type II collagen, resulting in cartilage destruction. In addition, cartilage glycoproteins, elastin, and other collagens can also induce autoimmune reactions. 2 Other autoimmune diseases are associated in 25%–30% of cases. Some cases were positive for antinuclear antibodies, rheumatoid factor, or circulating immune complexes. Yoshiro Horai et al. have reported a case of relapsing polychondritis associated with auricular cartilage infiltration of immunoglobulin G4-positive plasma cells and lung cancer with positive autoimmune series. The patient was found to have lung squamous cell carcinoma during hospitalization for RP. 11 It is believed that the pathogenesis of RP may not be lung cancer paraneoplastic syndrome because lung cancer surgery does not change the occurrence and development of RP, and no IgG4-positive cells are found in the pathology of specimens after lung cancer resection. It is unclear whether there is a direct relationship between the occurrence of RP and lung cancer. Hara Y et al. believe that lung tumors may produce bioactive protein or polypeptide substances, and tumors may cause autoimmune reactions or immune complexes; moreover, immunosuppression may trigger extrapulmonary symptoms such as recurrent polychondritis.12,13 Serial examinations of blood rheumatic autoimmunity were negative in this patient. No previous autoimmune disorders. In this case, the patient had repeated cough and expectoration for 4 months before admission to our hospital, had redness, swelling, pain, and ocular congestion in the left auricle, and was misdiagnosed as erysipelas and herpes zoster in the left ear in an outside hospital. After admission to our hospital, the patient was diagnosed with small cell lung cancer and had RP symptoms again during hospitalization. In this case, the patient was treated with chemotherapy combined with radiotherapy, without surgical resection, so there was no surgical specimen of lung cancer. Combined with RP symptoms before the diagnosis of small cell lung cancer, it was unclear whether RP was primary or lung cancer paraneoplastic syndrome.
Glucocorticoid, 14 immunosuppressive agents like cyclosporine, methotrexate and dapsone, and biological agents are used for common treatment. 15 Indomethacin can be used for the treatment of chronic intractable cases. 16 In this case, the patient was given oral prednisone 60 mg once/day for RP, and the symptoms of auricular redness and swelling, auricular collapse, and subconjunctival hemorrhage in the left eye were gradually relieved. Aldo Pezzuto et al. believe that different therapeutic in lung cancer have a relatively good survival time. 17 Guidelines suggest that radiotherapy is used in stage IV NSCLC. 18 Rami-Porta R et al. believe that the use radio-chemotherapy in unresectable lung cancer, it can be successful in improving progression-free survival. 19 Chemotherapy combined with radiotherapy was given for small cell lung cancer in this patient. The chemotherapy regimen was carboplatin combined with etoposide. Local radiotherapy was performed on submediastinal metastatic lymph nodes and adjacent lymph node areas as well as tracheal bulge and corresponding thickened tracheal wall areas. The patient was in stable condition at present without conjunctival congestion. It was compatible with the findings reported in the previous literature.
Conclusion
Small cell lung cancer complicated by RP is very rare in clinical practice with atypical early symptoms; therefore, misdiagnosis is incidental. In the diagnosis and treatment process, we should strengthen the tumor awareness and adhere to the two-point method (the disease is divided into benign and malignant). For some relatively rare clinical manifestations and diseases, the possibility of malignant tumor should be considered first in the diagnosis. Given that the malignant tumor cannot be excluded, further examination or consultation and referral should be performed. For cases of RP with cartilage and other connective tissue, including ears, nose, eyes, joints, respiratory tract, and other symptoms, we should pay great attention to whether the case is caused by lung cancer. The key lies in comprehensively examination and reasonably combination of a variety of examination techniques, so as to timely detect primary disease and further reduce misdiagnosis and missed diagnosis.
Footnotes
Author contribution
Yuan Liu and Jian Xu: conceptualization, methodology, formal analysis, investigation, and writing—original draft. Ning Wang: validation, investigation, and writing—review and editing. Chunfang Liu and Meng Dai: formal analysis and investigation. Ying Bi and Xue Han: writing—review and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.