
Abstract
Intestinal ischemia results from diminished perfusion of the colon resulting in tissue hypoxia. Anecdotal reports suggest that cocaine-induced intestinal ischemia has the highest mortality and longer length of stay among the vasoconstrictors. The present study aimed to summarize the available studies in the literature to assess the effect of routes of consumption on the outcomes of cocaine-induced intestinal ischemia. We conducted a systematic search of MEDLINE from inception through October 2019. Studies of cocaine-induced intestinal ischemia were included if data were available on comorbidities, mortality, and hospital length of stay (LOS). The study’s primary outcomes were mortality and need for surgery, while secondary outcomes included the hospital length of stay, LACE index, and hospital score. Statistical tests used included linear and binary logistic regression. STATA 2015 was used, and P < 0.05 was statistically significant. Of the 304 studies, 8 case series and 45 case reports (n = 69 patients) met the inclusion criteria. Different routes of cocaine use had similar mortality odds and the need for surgery for intestinal ischemia. Hospital LOS showed significant difference among the subgroups. Readmission scores (LACE and hospital score) were higher for intravenous and smoking than ingestion and intranasal use (P < 0.05). In conclusion, different routes of cocaine use appear to have similar mortality odds for intestinal ischemia, which vary significantly among the different routes of cocaine consumption for the length of stay and readmission scores. Prompt recognition of the route of cocaine use is vital to improve the outcome. Large-scale and well-designed observational studies are needed to investigate this topic further.
Introduction
Intestinal ischemia is a well-known complication for cocaine users, and it is the result of diminished perfusion of the colon, which does not suit the metabolic requirements, resulting in tissue hypoxia.1,2 According to the National Survey on Drug Use and Health (NSDUH), cocaine use has remained stable since 2009, especially among the adults aged 18 to 25 years; however, there has been an uprise in the number of users in the older age group. 3 The pathophysiology of cocaine-induced ischemia includes, but is not limited to, mesenteric vasoconstriction, increased platelet aggregation, and focal endothelial injury. 4 Patients will present with the acute onset of crampy abdominal pain and passage of bright red or maroon blood, often mixed with stool. 5 Anecdotal reports suggest that cocaine-induced intestinal ischemia has the highest mortality and longer length of stay among the vasoconstrictors. 6 A limited amount of data has been gathered regarding the extension of intestinal ischemia based on the route of cocaine used. Therefore, we aim to summarize the available data on the outcomes of cocaine-induced intestinal ischemia and the type of route administration.
Methods
Data Abstraction
A systematic literature search was conducted on PubMed, Scopus, and Embase using the PICO framework and is reported under the PRISMA framework (Figure 1). 7 We used “Mesenteric Ischemia” and “cocaine” as the Medical Subject Headings (MeSH) terms (search strategy provided in supplemental files). The first author systematically extracted all the potential data. For inclusion in this review, the patient discussed a diagnosis of mesenteric ischemia with cocaine as its etiology. Another author reviewed the included data’s reference lists to identify other studies that our search strategy might have missed. In cases where more than one publication from the same author was identified, the abstracted manuscripts were cross-examined for replicated patient data. Duplicate information was excluded if an overlap was found related to patient-specific data. Our search was restricted to English-language studies conducted in human participants. Articles were excluded if patients had a secondary or significant concomitant reason to develop intestinal ischemia (eg, adhesions, volvulus, serotonin syndrome, and another definite etiology causing septic shock) to avoid bias. The study design was simplified to case reports or case series. Patient-specific information was recorded for age, gender, race, smoking status, route of cocaine consumption, length of stay, location of affected bowel segment, colonoscopic findings, and whether a surgical procedure was required during the hospital or not. Cocaine use was confirmed by either a positive urine drug screen or during history taking from patients. Data related to colonoscopic findings were recorded for the presence or absence of hemorrhages. Also, patterns of intestinal ischemia were evaluated by colonoscopy reports, computed tomography (CT) images, or surgical findings.
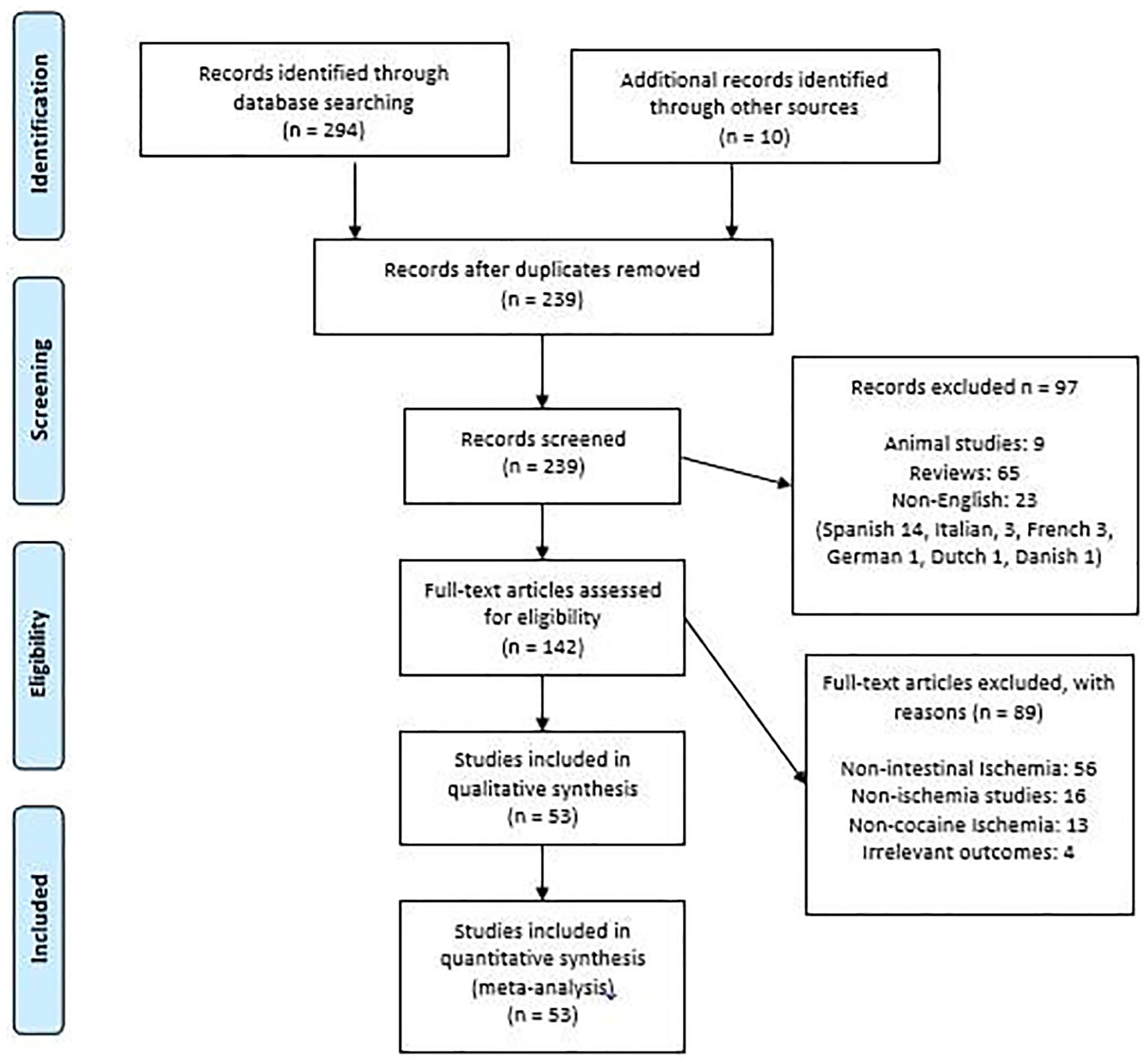
PRISMA flowchart describing study selection and inclusion process.
Design and Analysis
All the statistical analysis was performed using Stata 15.0 software. Primary outcomes of the study were mortality and the need for surgery, while secondary outcomes included hospital length of stay (LOS), LACE index, and hospital score. Different routes of cocaine use included intravenous (IV), ingestion (for simplicity, the rectal route was grouped under this category), intranasal, and smoking. We reported descriptive statistics as mean ± standard deviations or median and interquartile range (IQR). We assumed that data were not missing at random and used the multivariate imputation by chained equations (ie, MICE) method to account for missing data in the study. The imputation model was constructed using information from all covariates used in regression models and other covariates in the available data without missing information. P < 0.05 was statistically significant. Outcomes were reported after adjusting for age, gender, and race. Binary logistic regression was used for mortality and the need for surgery. Kruskal-Wallis test was used for LOS, followed by post-hoc testing with Dunn’s test. Other covariates were plotted on a histogram to determine the type of regression analysis for variables. For example, negative binomial regression analysis was used to test the difference between different groups of cocaine consumption for hospital score, whereas Poisson regression was used for the LACE index. Of the 304 studies, 8 case series and 45 case reports (n = 69 patients) met the inclusion criteria (Figure 1).
Results
Baseline Characteristics
The initial search resulted in 304 manuscripts for cocaine-induced intestinal ischemia, all of which were screened for inclusion. Overall, 142 manuscripts were eligible for critical evaluation, and ultimately 53 articles met the inclusion criteria. In addition, there were 45 case reports among the included articles.2-4,8-49 In addition to case reports, there were case series.1,50-56 In the final step, manuscripts where the route of cocaine consumption was missing were excluded. Among the study participants (n = 69), 7.2% were of white ethnicity, 21.7 % were of black ethnicity, and 7.2 % were of Hispanic ethnicity (Table 1); 66.6% were female, and 78.2% of the patients did not report a history of smoking. Routes of cocaine consumption were smoking (23), IV (18), ingestion (13), and intranasal (15). Abdominal pain was reported on a presentation by 84.05% of the patients, and bloody bowel movements were reported in 27.5% of the patients. Diagnostic modalities used included colonoscopy 27.5%, sigmoidoscopy 7.2%, CT 42.0%, plain abdominal films 10.1%, and laparotomy 52.1%. Combining findings from all the diagnostic modalities revealed small bowel involvement in 44.9%, large bowel in 37.6%, and small plus large bowel in 13.0%. Findings of severe intestinal ischemia, including ulcers, hemorrhages, and gangrene, were found in 27.5% of the patients on colonoscopy or autopsy. Forty-two patients (60.8%) were managed surgically. Nine surgically treated patients died, and the most common causes of death were cardiac arrest and septic shock, causing multi-organ failure, while 78.6% recovered without any further complications. In this series, nonoperative management had a success rate of 81.5%, while surgical management had a success rate of 78.6%. Based on the available reported dataset, median hospitalization days for patients managed non-operatively were 2.5 (IQR: 4), while patients requiring surgery were 7 (IQR: 16). Patients experiencing the outcome of mortality according to the route of consumption included IV: 2, ingestion: 3, intranasal: 5, and smoking: 3. Patients requiring surgery according to the route of consumption included IV: 9, ingestion: 12, intranasal: 6, and smoking: 15.
Baseline Characteristics of the Patients Included in the Study.

Abbreviation: LOS, length of stay.
Outcomes
For mortality, different routes of cocaine did not differ from each other in terms of adjusted mortality odds (Table 2). IV cocaine route was considered as reference. For mortality, the odds ratio (OR) for smoking was 0.18 (95% CI: 0.11-1.60, P = 0.06), ingestion 0.75 (95% CI: 0.17-3.35, P = 0.71), and intranasal 0.44 (95% CI: 0.14-1.44, P = 0.18). The P-value for adjusted odds of requiring surgery was greater than 0.05, necessitating the acceptance of the null hypothesis. For surgery, the odds ratio (OR) for smoking was 2.33 (95% CI: 0.89-6.07, P = 0.08), ingestion 2.5 (95% CI: 0.48-12.88, P = 0.27), and intranasal 0.86 (95% CI: 0.28-2.55, P = 0.78). There were statistically significant differences among the secondary outcomes in the study: hospital LOS, LACE index, and hospital score. Adjusted readmission scores (LACE and hospital scores) were higher for IV and smoking than ingestion and intranasal use (with P < 0.05) (Figure 2). Kruskal-Wallis test was conducted to examine the differences in LOS according to the route of cocaine consumption. It showed a statistically significant difference (chi-square = 9.38, P = 0.02, df = 3) in LOS due to cocaine-induced intestinal ischemia among the various routes of cocaine use with mean rank LOS scores of 126 for IV, 269 for smoking, 93 for ingestion, and 39 for the intranasal route. Pairwise comparisons using Dunn’s test in the post-hoc analysis showed that an intranasal route tends to have a longer stay than the other routes (intranasal-IV; longer median LOS by 2.69 days, P = 0.02, smoking-intranasal; shorter median LOS by 2.77 days, P = 0.01) (Table 3). Secondary analysis was done for mortality, the requirement for surgery, and LOS based on the length of bowel involved. It was categorized as small intestine, large intestine, or small and large intestine. Adjusted odds ratios for mortality or need for surgery did not reach statistical significance based on the ischemic bowel segment involved (Table 4). Kruskal-Wallis test for LOS based on bowel segment involved did not show statistically significant difference (chi-square = 0.83, P = 0.66, df = 2).
Outcomes.
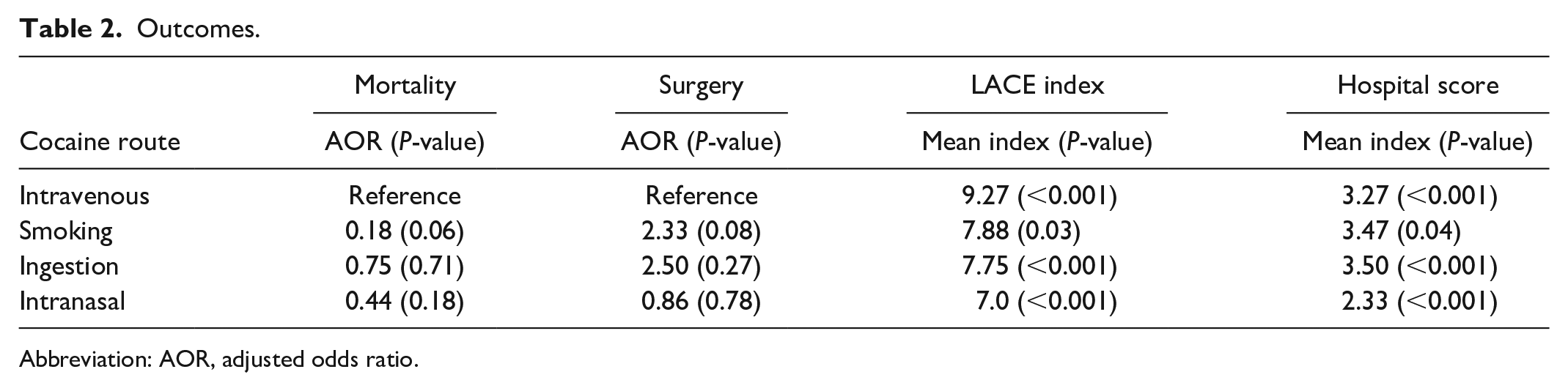
Abbreviation: AOR, adjusted odds ratio.

Distributions of continuous variables.
Pairwise Comparison for Length of Stay.
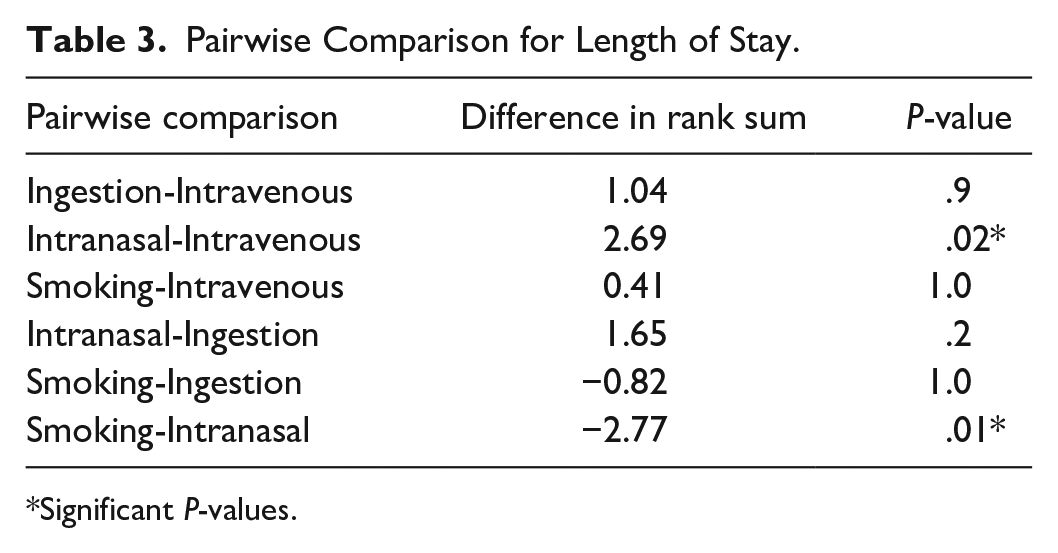
Significant P-values.
Secondary Analysis for Different Region of Bowel Segment Involved.
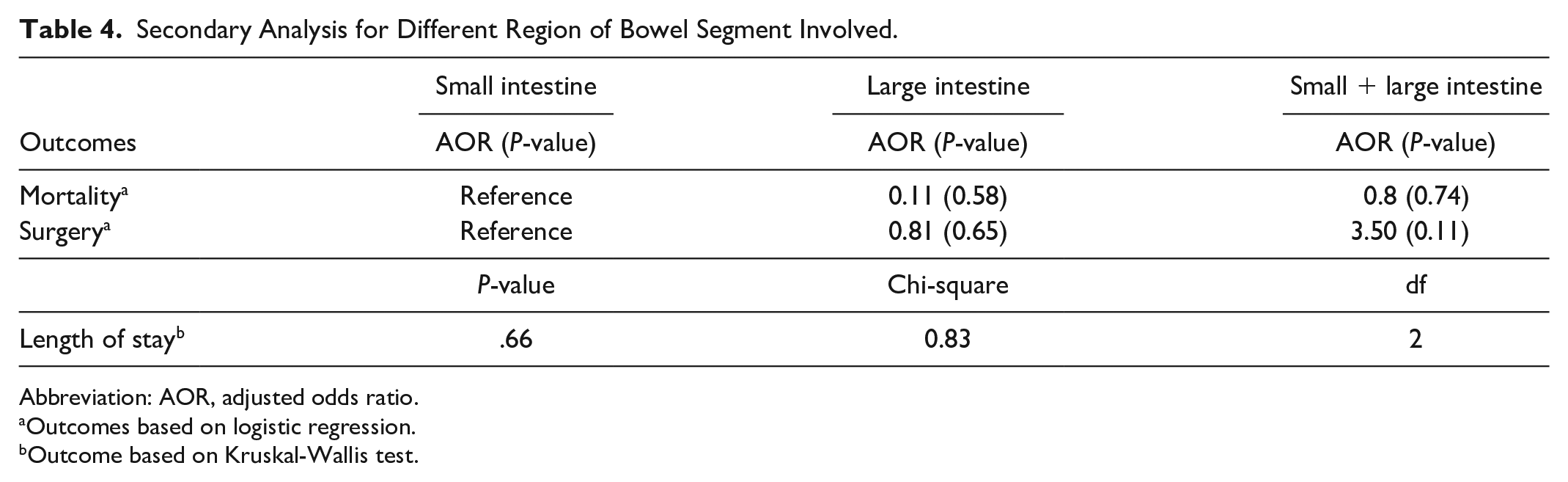
Abbreviation: AOR, adjusted odds ratio.
Outcomes based on logistic regression.
Outcome based on Kruskal-Wallis test.
Discussion
Cocaine is an alkaloid obtained from the erythroxylon coca plant, inhibiting the presynaptic reuptake of norepinephrine, dopamine, and serotonin. It is an ester of benzoic acid and nitrogen-containing base. They also displace the neurotransmitter from the membrane eliciting a sympathomimetic response and increase the endothelial cell membrane’s calcium flux, causing a direct vasoconstrictor effect. 2 In addition, cocaine stimulates alpha-adrenergic receptors in the mesenteric arteries that trigger vasospasm and intestinal ischemia, direct vasospasm from calcium channels, and indirect vasospasm by releasing norepinephrine and reducing its reuptake, platelet, and endothelial cell activation by thromboxane B2 release and thrombosis due to endothelial damage from the low release of endothelin; these are some of the mechanisms of cocaine-induced intestinal ischemia. 57 Cocaine has a medium half-life of 1.5 hours in new users and 3 hours in chronic users. It takes 7.5 hours for the cocaine metabolites to leave the system. 44
Cocaine is used recreationally through nasal, parenteral, and oral routes. The increased use of inexpensive crack cocaine has contributed to the increased incidence of cocaine-induced enteropathy. The national cocaine database indicates that men are twice as likely to have cocaine use disorder than women. Health care disparity results in delay in getting medical care and hence the presentation with complications from cocaine use as intestinal ischemia and colitis could be a potential reason for this gender distribution.
Cocaine-induced gastrointestinal disorders include gastric ulcerations, visceral infarction, intestinal ischemia, gastrointestinal tract perforation, and retroperitoneal fibrosis. 3 We sought to compare the effects on the outcomes of cocaine-induced intestinal ischemia of different routes of cocaine consumption. Patients usually present with abdominal pain and bloody diarrhea, which were the presenting symptoms in most patients. The mortality rate did not vary depending on the route of administration. This is likely because once it reaches the bloodstream, the mechanism of action on the receptors remains the same to cause intestinal ischemia.
Cocaine administration more than twice per week for more than 6 months is associated with mesenteric thrombosis, perforation, and ischemia irrespective of the administration route. 57 Colon ischemia due to any cause involving the right route has been reported to have worse outcomes. Still, the secondary analysis in our study showed no difference with respect to the intestinal segment involved for cocaine-induced intestinal ischemia in particular.58,59 In our study, we found that for the majority of the time, the small intestine is involved. This is the first synthesized systematic review of all the reported cases of 69 patients with cocaine-induced intestinal ischemia. There was also no significant difference in mortality or surgery requirement based upon the bowel segment involved in our study.
Our study found the significant differences in the LACE index and hospital score for cocaine-induced intestinal ischemia based on the route of administration. LACE index is a tool used to predict the 30-day non-elective readmission risk after hospital discharge in both surgical and nonsurgical patients. 60 Similarly, the hospital score also risk-stratifies patients for 30-day readmission. 61 Although the LACE score and hospital score are well-studied internally validated parameters, there has not been a study that compares these two parameters for cocaine-induced ischemia. IV and ingestion routes were found to have an overall higher odds of readmission scores (LACE index and hospital score) than smoking and intranasal routes (P < 0.05). Rapid availability to bind receptors, comorbid complications arising from intravenous drug use, including immunodeficiency viral syndrome for IV route, and direct interactions with bowel mucosa with more potential to cause bowel necrosis and hemorrhages for ingestion route are possible explanations for these higher adjusted odds for readmission scores.
In our study, the hospital LOS differed significantly among the various routes, and pairwise testing using Dunn’s test revealed the significant differences in two of these pairs. The intranasal route had a longer median LOS by 2.69 days (P = 0.02) than IV, while smoking had a shorter median LOS by 2.77 days (P = 0.01) from the intranasal route. Thus, the surgically managed patients had a median LOS longer than the patients managed medically; the LOS difference also stems from other predictors, possibly inherent, and is an arena for further studies.
Cocaine-associated colitis has a mortality rate of 28.5%, whereas, in a hybrid case-control study, mortality associated with ischemic colitis with cocaine use was 20%. With non-cocaine-associated ischemic colitis, it was 7.7% (P < 0.0366).5,62 The mortality was found to be 25.0% in our study dataset. The cause of death usually is attributed to progressive intestinal ischemia, septic shock, and multiorgan failure, as was found in our study. 5 Our study reported that there is no association of mortality rate with the route of administration of cocaine. This is vital to consider as it reinforces that any form of cocaine intake can have a similar mortality rate. Early diagnosis is crucial due to the high morbidity and mortality and is usually treated medically unless there is a life-threatening complication such as peritonitis and perforation. Sixty percent of the patients in our dataset required surgical intervention indicating the complexity and comorbidity burden rendered due to cocaine-induced intestinal ischemia. However, medical management had a higher success rate than surgical management as surgery is attempted when medical management fails and is reserved for advanced and more severe diseases.
There are several shortcomings in our study. The main limitation of our study is the small sample size and, thereby, low power. The lower level of evidence of the included studies contributes to lower power as well. Confounding bias could also be a potential limitation as we used only age, race, and sex in our study. Other factors could potentially affect cocaine use, including other substance abuse, alcohol intake, and psychiatric comorbidities, among a few. Some of these variables could not be extracted in the selected articles due to not being reported in some studies. The studies included were restricted to only English language. Despite these limitations, this is the first study to our knowledge that reports and summarizes the available data on the effects of the routes of cocaine consumption on intestinal ischemia.
Conclusions
The routes of cocaine administration are associated with a marked difference in the length of hospital stay and readmission rate for cocaine-induced intestinal ischemia, with intravenous routes having higher hospital stay and readmission risk compared to the other routes of consumption. The routes of cocaine consumption are not associated with differences in mortality and surgical outcome. However, the medical management of cocaine-induced intestinal ischemia was found to have better outcome than surgical management in our study; hence, conservative management should be considered first unless there is a life-threatening surgical emergency. As the recreational use of cocaine rises, intestinal ischemia should be kept in the differential diagnosis of patients presenting with abdominal pain and bloody stools. The possibility of cocaine abuse should be considered for patients diagnosed with intestinal ischemia.
Supplemental Material
sj-docx-1-hic-10.1177_23247096211051921 – Supplemental material for Does the Route of Cocaine Use Affect the Mortality and Outcomes of Cocaine-Induced Intestinal Ischemia?: A Systematic Review
Supplemental material, sj-docx-1-hic-10.1177_23247096211051921 for Does the Route of Cocaine Use Affect the Mortality and Outcomes of Cocaine-Induced Intestinal Ischemia?: A Systematic Review by Umer Farooq, Amlish B. Gondal, Ammu Susheela, Zahid Ijaz Tarar, Adnan Malik, Muhammad Usman Zafar, Aftab Sharif and Ghulam Ghous in Journal of Investigative Medicine High Impact Case Reports
Footnotes
Author Contributions
Conceptualization: Umer Farooq and Amlish Bilal Gondal; Formal analysis and investigation: Umer Farooq, Adnan Malik, and Zahid Ijaz Tara; Writing—original draft preparation: Umer Farooq, Aftab Sharif, and Ammu Susheela; Writing—review and editing: Umer Farooq and Muhammad Usman Zafar; Supervision: Amlish Bilal Gondal and Ghulam Ghous
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series that are already published in the literature. This study is based on systematic review of already published cases.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because our study is a systematic review of already published cases in the literature. We followed PRISMA reporting guidelines in this systematic review.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.