
Abstract
Odontogenic bacteremia, most commonly involving gram-positive oral flora, can result from daily self-care practices or professional dental procedures. Though usually transient and quickly cleared by the immune system, the presence of periodontal disease increases the frequency of exposure and risk of persistence of oral-systemic infections. Comorbidities such as asplenia, alcoholism, and immunocompromise increase the risk of complications of hematogenous spread and severe systemic illness. Capnocytophaga is a genus of anaerobic fastidious gram-negative bacilli, which is a common member of human oral flora, and its density is proportional to mass of dental plaques and periodontal diseases. Capnocytophaga spp that colonize humans are less virulent and are uncommon causes of bacteremia when compared with the Capnocytophaga typical of canines. C gingivalis has been rarely reported as a cause of disease in immunocompromised or immunocompetent hosts. In this article, we present a case of an immunocompromised 70-year-old man with poor oral hygiene, on methotrexate and prednisone for rheumatoid arthritis and sarcoidosis, who was admitted for chronic obstructive pulmonary disease exacerbation and developed C gingivalis bacteremia and septic shock after an episode of upper gastrointestinal bleeding. Poor oral hygiene in our patient is believed to have increased his risk as an immunocompromised patient to developing C gingivalis bacteremia. This case highlights the importance of oral care in immunocompromised patients especially while hospitalized, and those about to receive transplant, chemotherapy, or on immune modulators.
Introduction
Bacteria of the genus Capnocytophaga are anaerobic or microaerophilic, fastidious, and fusiform gram-negative bacillus that are part of oral flora of humans, dogs, and cats.
Capnocytophaga gingivalis is one of 6 identified human colonist species found in adults and children. So far C canimorsus and C cynodegmi are the 2 species identified as part of animal oral flora.1-3
Capnocytophaga spp have a worldwide distribution across all ages as normal flora of the oral cavity. Pathologically, they can cause nonfulminant diseases such as periodontitis, caries, and plaque across all ages. 4 Comorbidities such as diabetes and malignancies in children increase the oral bacterial burden of Capnocytophaga spp isolated.5,6 The Capnocytophaga animal microbiota may be transmitted through bites, scratches, or nontraumatic contact with dog or cat saliva. 2 C canimorsus and C cynodegmi are more virulent than species found as human flora, and fulminant infections can be seen in immunocompetent patients, though they are more prevalent in immunocompromised patients with comorbidities including alcoholism, asplenia, or malignancies. The infections cause can range from localized cellulitis to fulminant life-threatening illnesses.7-9 C canimorsus, however, is the most frequently isolated species in fulminant life-threatening disease.
In contrast, C gingivalis has rarely been reported as an invasive pathogen in humans, which could be a result of only genus-level identification with previous microbiologic technologies. In this case, we present an elderly immunocompromised man with severe C gingivalis infection.
Case Presentation
A 70-year-old man presented with 3 days of loose watery stool, worsening generalized weakness, 1 day of confusion, and inability to walk. He had a history of chronic medical problems including asthma/chronic obstructive pulmonary disease (COPD) requiring 4 L of home oxygen therapy, rheumatoid arthritis, sarcoidosis, and chronic kidney disease. He was on long-term 17.5 mg methotrexate weekly and 10 mg prednisone daily.
Vital signs recorded on admission included normal temperature with normal heart rate and blood pressure. On initial physical examination, he was noted to be awake but lethargic and had poor oral hygiene with multiple dental caries. On auscultation, there was reduced air entry into his lungs, and bilateral wheezing, and his abdomen was tender to palpation. He was noted to have extensive bruising over his left hand and bilateral pitting pedal edema. He was admitted and managed for COPD exacerbation and dehydration due to diarrhea.
On admission, he was started on intravenous methylprednisolone and bronchodilator treatments; on day 2, his mental status became more altered. He was later intubated urgently after failure of bilevel positive airway pressure (BiPAP) trial for acute on chronic hypercapnic respiratory failure. He was also started on diuretics initially and later hemodialysis for acute kidney injury. After 3 days of intubation, his mental and respiratory status had improved remarkably, and he was successfully extubated on day 5 of admission.
On day 9 of admission, he developed fever of 38.7 °C. Blood and urine cultures were collected, and he was promptly started on empiric vancomycin, cefepime, and metronidazole.
By day 10, his mental status declined, and he was again in hypercapnic respiratory failure. He failed BiPAP trial again and had to be re-intubated. At time of intubation, a pool of blood was noted in mouth and hypopharynx and 2.5 L of bloody fluid suctioned from his stomach. He was placed on pantoprazole infusion for suspected gastrointestinal (GI) bleeding and aspiration was strongly suspected. Broad antibiotics that had been started the prior day were continued. A few hours later, norepinephrine infusion and stress-dose hydrocortisone were started due to persistent hypotension. Esophagogastroduodenoscopy revealed esophageal erosion, gastric, and duodenal ulcers.
On day 11, he still required high doses of norepinephrine despite resolution of fever. Urine culture obtained on day 9 had >100 000 colony forming units/mL of Escherichia coli. Vancomycin and metronidazole were stopped to target urinary tract infection with E coli. Computed tomography scan of abdomen showed bilateral lower lobe consolidations suspicious for pneumonia.
Blood cultures obtained on day 9 became positive on the fourth day of culture, with Gram-negative bacilli in one anaerobic bottle of 4 culture bottles, his antibiotic was switched to piperacillin-tazobactam and tobramycin. The isolate was identified 2 days later, on hospital day 14, as Capnocytophaga spp. The infectious disease (ID) team was consulted, piperacillin-tazobactam and tobramycin was discontinued in favor of renally dosed ampicillin-sulbactam. During a discussion with his wife by the ID team on day 15 of admission, she reported having a dog that was not usually in contact with her husband, and she reported that the patient chews tobacco, stores, and then re-chews tobacco that he stored at room temperature for varying lengths of time. Patient’s right upper extremity remained edematous and a venous duplex confirmed suspicion of a deep vein thrombosis in the right internal jugular and right brachiocephalic veins, which was associated with the central venous catheter.
The patient was taken off vasopressors on hospital day 16 and extubated on day 17. The patient was treated for 4 weeks with renally dosed intravenous ampicillin-sulbactam for endovascular infection due to the occlusive thrombosis detected while patient had bacteremia.
Using 16s rRNA gene sequencing, Capnocytophaga spp isolated was reported to be C gingivalis by Quest Diagnostics, Nichols Institute, Chantilly, Virginia. He was counseled and advised to keep up his dental appointments and stop re-chewing his tobacco.
Discussion
Bacteremia resulting from a break in mucosal barrier is common: from the oral cavity, routine activities such as brushing and flossing regularly cause transient bacteremia with oral flora. Odontogenic diseases pose an increased risk of persistent bacteremia due to undrained foci of infection. Bioburden, such as in extensive dental plaques, or mucosal disruption in gingivitis, oral ulcers, gastritis, colitis, peptic ulcer disease, and inflammatory bowel diseases can also increase the risk of microbial gut translocation.10-12 Our patient had been on methotrexate and prednisone for rheumatoid arthritis causing him to be immunocompromised. Prolonged use of glucocorticoids and methotrexate have individually been shown to lower the integrity of the gut mucosa leading to ulcerations, perforations, and increased risk of bleeding.13-15
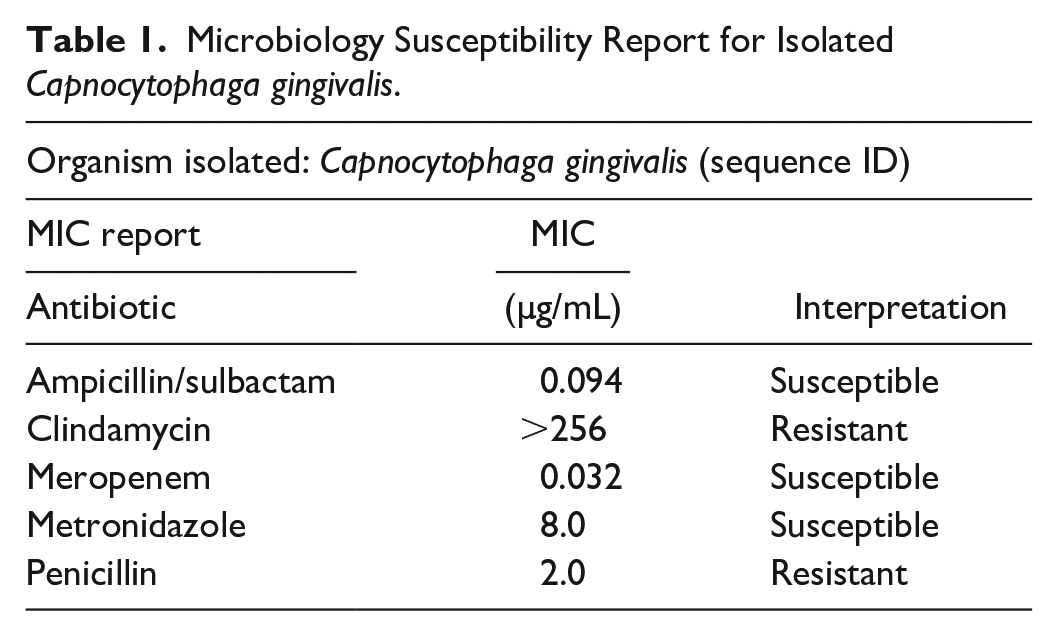
Only one case of bacteremia due to Capnocytophaga has been previously reported in a patient with rheumatoid arthritis on methotrexate. This individual subsequently died of disseminated intravascular coagulation, and acute respiratory distress syndrome from C canimorsus infection following dog bite. 16 Our patient notably had poor dentition with dense plaques, multiple dental caries, and a habit of re-chewing saved tobacco, stored at room temperature, which may have contributed to increased oral bacterial colonization. The mechanism of his bacteremia in this patient was thought to be translocation of oral flora colonized with C gingivalis through compromised gastric mucosa due to the upper GI bleeding. The Capnocytophaga isolated was finally reported to be C gingivalis using 16s rRNA sequencing sensitive to ampicillin-sulbactam, meropenem, and metronidazole, resistant to clindamycin and penicillin (Table 1).
Microbiology Susceptibility Report for Isolated Capnocytophaga gingivalis.
A detailed literature search was conducted using the search words “Capnocytophaga gingivalis” in PubMed. Ninety-three abstracts were found for Capnocytophaga gingivalis as shown in flow diagram in Figure 1. Capnocytophaga gingivalis + Filters: Humans yielded 71 abstracts. Addition of filter case reports yielded 7 abstracts. This contained 4 human case reports of C gingivalis systemic infections, 1 Japanese abstract, 2 periodontal diseases abstracts, and 1 molecular immunology abstract. This initial search erroneously eliminated a previously found case report, prompting a manual review after alternate search parameters were used. Finally, search using Capnocytophaga gingivalis [Title] Filters: Abstract yielded 14 abstracts that included all 5 case reports for C gingivalis systemic infection in humans, which is reflected in Figure 1.

Case reports search flow diagram.
Polymicrobial and primary oral/periodontal abstracts were excluded from this review. Five case reports of human non-oral C gingivalis infections were found and included in this case review. Three of the cases were related to lung infections, 2 cases were in immunocompromised hosts, 1 joint infection, and 1 related to oral infection. The cases included bacteremia in a 6-year-old with acute lymphocytic leukemia and gingivitis, 8 pneumonia, and bacteremia in 30-year-old man post autologous stem cell transplant, 17 lung abscess in a normal host, 18 insidious joint infection in a normal 3-year-old, 19 and an acute COPD exacerbation 20 (Table 2).
Capnocytophaga gingivalis Case Report Summary.

Abbreviation: COPD, chronic obstructive pulmonary device.
Antimicrobial susceptibilities in the identified cases followed no specific pattern as 4 of the 5 cases had class resistance reported, with only one multi-drug resistant case resistant to 4 classes of antibiotics. As in our case, many of the C gingivalis strains appear to remain susceptible to cephalosporins and β-lactam/β-lactamase inhibitor combinations.
In conclusion, in this case, poor dental hygiene with periodontitis posed an increased risk of infection with human oral strains of genus Capnocytophaga in immunocompromised patients. Optimal oral care while inpatient can reduce the oral bacterial burden in the event of aspiration and is an important part of the ventilator acquired pneumonia bundle. This case highlights the importance of oral care in immunocompromised patients and the risk of bacterial translocation with GI bleeding or aspiration.
Footnotes
Authors’ Note
The contents of this article do not represent the views of the Department of Veterans Affairs or the US government. This work was previously presented at the Southern Regional Meeting, New Orleans, Louisiana, 2019.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The material is the result of work supported with resources and the use of facilities at the Charlie Norwood VA Medical Center. The funding organizations had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. The contents of this publication are solely the responsibility of the authors and do not represent do not necessarily reflect the views, opinions or policies of The Department of Veterans Affairs, or the the U.S. Government. Mention of trade names, commercial products, or organizations does not imply endorsement by the U.S. Government.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published article.