
Abstract
Syncope is a sudden but reversible brief loss of consciousness secondary to an acute reduction of cerebral perfusion. Reflex syncope denotes neurologically mediated syncope, which includes vasovagal, carotid sinus syndrome, and other situational syncope. The most frequent form of syncope is vasovagal, which is triggered by emotional stress or prolonged standing, and may be diagnosed with the tilt table test. A thorough investigation of syncope is necessary as serious cardiovascular disorders may also be a cause. A tilt table test is a widely used tool utilized by clinicians to diagnose vasovagal syncope and is sometimes augmented with isoproterenol, a β-sympathomimetic that acts on the heart. This report seeks to explain a case of a 48-year-old previously healthy woman who experienced inferior wall ST elevations during tilt table test supplemented with isoproterenol. There is reason to believe that the results of this patient’s tilt table test were due to vasovagal syncope in conjunction with right coronary artery vasospasm.
Introduction
Syncope can be defined as a temporary loss of consciousness that may be related to insufficient blood flow to the brain. Although there are many different causes it is usually broken down into neurologically mediated, cardiac syncope, orthostatic, and the most common, vasovagal syncope (VVS). VVS is usually accompanied by a prodrome, an inciting or trigger event, but is often not reported, whereas cardiac syncope is usually sudden in onset with a quick recovery. 1 The diagnosis is aided by the use of multiple tests including 24-hour Holter monitors as well as provocative testing such as the tilt table test (TTT). TTT is a widely used noninvasive tool in assessing patients with unexplained syncope. It has been reported that the TTT has a 30% to 90% positive rate and above 90% specificity in detecting VVS. 2 This relatively safe and effective method is sometimes augmented with medications, such as isoproterenol (ISO) to provoke a stronger response. ISO is a nonselective β agonist that is commonly used in TTT since it is more effective and efficient in inducing positive vasovagal response compared with the standard passive TTT. 3 Its mechanism as a β-agonist is vital in producing coronary vasospasm when used in combination with the TTT. There have been reports of rare yet life-threatening complications with this test including myocardial infarction, ventricular tachycardia, as well as cardiac arrest.4-6 In 50% to 60% of cases, the use of ISO caused coronary vasospasm leading to ST elevation (STE).7,8 In those cases, patients would exhibit a rapid decrease in heart rate prior to complaints of angina and presyncope. Although the mechanism is unclear, it is proposed that the sympathetic stimulation and parasympathetic activation plays a critical role in inducing coronary vasospasm. We present a similar case of a 48-year-old female who underwent TTT and subsequently had coronary vasospasms leading to STEs after infusion of ISO with resolution of her chest pain after administration of nitroglycerin.
Case Presentation
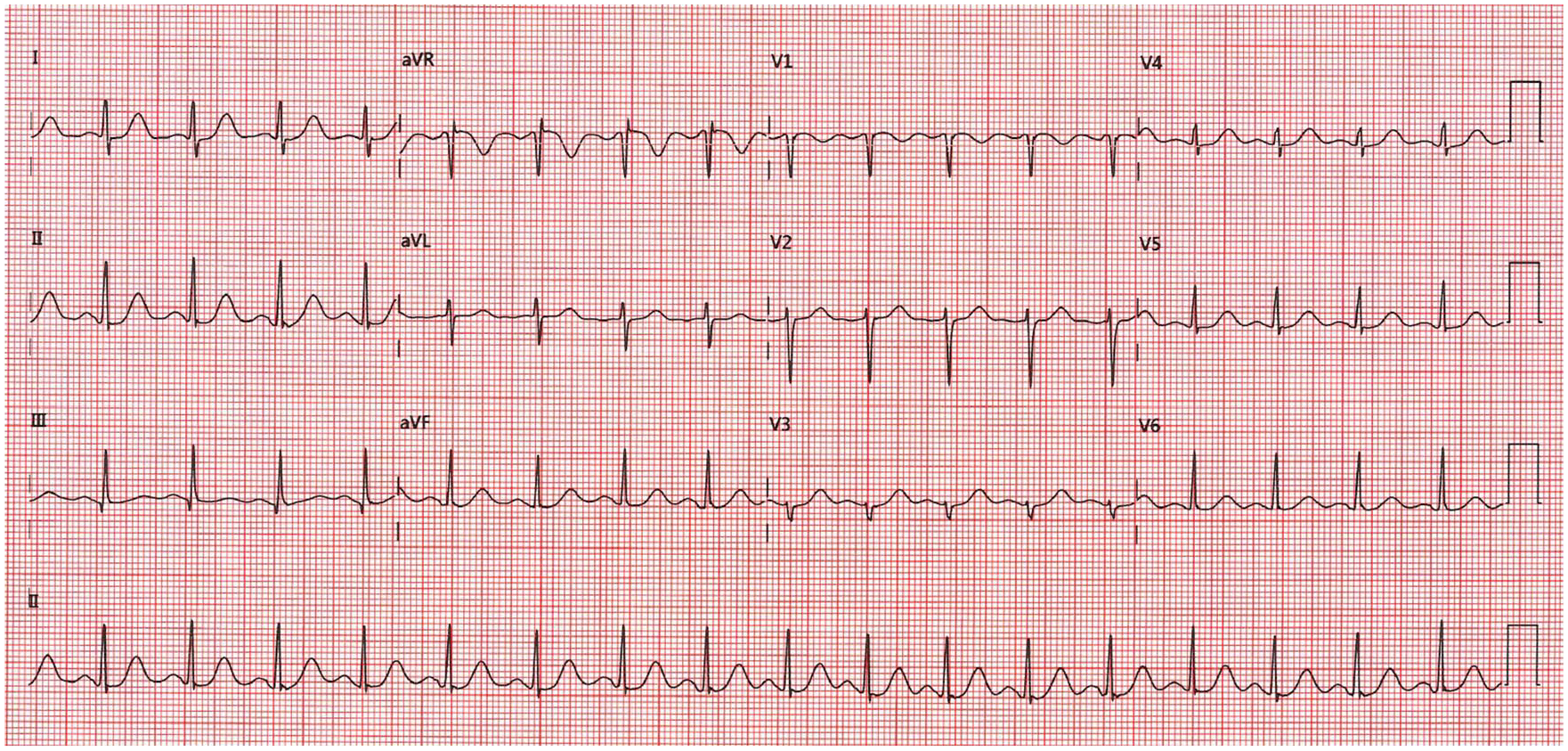
A 48-year-old female presents to clinic for syncopal episodes with associated severe burning sensation in her throat radiating to her chest. Patient underwent tilt table testing for further evaluation. Findings were unremarkable during her initial and exercise phase (Figures 1 and 2). During the second stage, ISO was started at 1 µg/min with increasing dosages between 3 and 5 µg/min. At 3 µg/min, the patient reported blurry vision that quickly self-resolved. ISO was increased to 5 µg/min for 5 minutes and discontinued once the patient reported feeling tired. The patient was brought to a supine position and within minutes reported 10/10 chest pain. Electrocardiogram showed ST segment elevations in leads II, III, and aVF (Figure 3) with bradycardia from 57 to 41 beats per minute and blood pressure of 77/57 mm Hg. Nitroglycerin 0.4 mg, normal saline bolus 250 mL, and supplemental oxygen was immediately administered. Approximately 25 minutes after, the patient reported her chest pain had resolved. She was admitted after to hospital for continued monitoring. During her hospital course, patient underwent coronary angiogram that showed patent coronary arteries without stenosis. Her echocardiogram was also normal with ejection fraction of 60%. The patient had reproducible symptoms. She is currently being treated with calcium channel blockers and long-acting nitrate without recurrence of symptoms.

ECG stage 1 at 0 seconds. Heart rate 57 beats per minute and blood pressure 110/61 mm Hg.
ECG stage 6 at 4:57 seconds. Heart rate 105 beats per minute and blood pressure 97/77 mm Hg.

ECG at recovery stage 1 at 13 seconds. ST elevations in leads II, III, aVF, and V3. Heart rate 57 beats per minute and blood pressure 77/57 mm Hg.
Discussion
Vasovagal syncope is a common and dangerous event many patients often face. It is an autonomic syncope invoked by parasympathetic hyperactivity (bradycardia), and/or sympathetic hypoactivity (vasodilatation). 7 As a result of this response the patient experiences reduced blood pressure and cerebral perfusion. The findings of the patient tested were unremarkable during initial TTT and also initially during exercise mimicking TTT, when the patient was intravenously given ISO. It was shortly after the patient became tired and ISO was stopped that the patient was placed back into supine position and STE were noticed and 10/10 chest pain was reported. Although the patient was supine at the time, this was clearly a positive TTT due to bradycardia and hypotension. The interest drawn from this study is the concomitant inferior wall STE and severe chest pain responsive to nitroglycerin. This finding indicates vasospasm of the right coronary artery, which was later validated by a normal coronary angiogram and echocardiogram.
The exact pathogenesis of coronary vasospasm is still unclear. Studies have shown that involvement of endothelial dysfunction, oxidative stress, chronic low-grade inflammation, and deficient aldehyde dehydrogenase 2 activity may contribute to it. 9 Regarding the use of ISO causing vasospasm, arguments of autonomic nervous system imbalance have been proposed. With regard to changes in heart rate during TTT, studies found increase in parasympathetic activity initially followed by increase in sympathetic activity. 4 While another study proposed that it is a withdrawal of parasympathetic activity that induces coronary vasospasms.5,10 Although conflicting ideas, from these studies we can conclude that the autonomic system does play an important role in coronary vasospasms.
As seen in previous case reports, ISO causes coronary vasospasms leading to STE causing angina. Even though most cases have been reported when it is used during tilt table testing, it can be seen with electrophysiology studies as well, 11 suggesting that ISO may have the potential to cause vasospasm by itself. A study done from 1997 to 2000 on 16 patients ranging from 42 to 75 years of age who underwent tilt table testing with ISO showed that patients who had coronary vasospasms, the right coronary was most frequently affected in 75% of the cases. 7 Similarly, our patient also showed STE in inferior leads correlating with right coronary artery vasospasm. Our patient also showed bradycardia with complaints of chest pain immediately when changed to supine position. This agrees with the explanation of autonomic dysfunction due to repositioning the patient, triggering the coronary vasospasm. With change from upright to supine, this activates parasympathetic response causing bradycardia and hypotension. The contrasting sympathomimetic action of ISO infusion in combination with the parasympathetic hyperactivity induces the coronary vasospasm. This finding is supported by a 15-patient study, which concluded that the TTT test with ISO infusion provoked coronary spasm with syncope or presyncope in 60% of patients with vasospastic angina. In the test positive group a significant reduction in heart rate preceded the vasospastic angina and syncope. The finding suggests that autonomic parasympathetic activation plays an important role in the provocation of coronary spasm in a subgroup of patients with vasospastic angina.3,10
Other studies have proposed that coronary artery vasospasm in the setting of ISO and TTT may suggest that this subgroup of patients have a more severe form of disease as compared with patients who do not develop STE. 2 Additionally, it appears that patients who develop more prominent bradycardia with positive test results indicate higher sensitivity of autonomic dysregulation. 2
Conclusion
Although it is rare, ISO has the potential to cause coronary vasospasms in healthy patients without coronary artery stenosis. It is important to consider this possibility when conducting TTT and to be prepared with nitroglycerin as coronary vasospasm can be fatal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval to report this case was obtained from the institutional review board (IRB #20044).
Informed Consent
Informed consent for patient information to be published in this article was not obtained because patient was lost to follow-up.