
Abstract
Tick-borne illness has been increasingly on the rise, since the first human case was reported in the late 1980s. Ehrlichia chaffeensis is one of the most common reported causes of tick-borne illness, particularly in the southern states of the United States. The clinical picture presents as a paradigm to the clinician, often missing the diagnosis without an appropriate history being taken and sometimes mistreated for other conditions. With the number of cases on the rise, new manifestations and clinical presentations due to E chaffeensis continue to be reported. Our case report is one such case in a 46-year-old male from Arkansas, with known exposure to multiple tick bites who presented with classical symptoms and laboratory values of tick-borne illness leading to atrial flutter. This unusual manifestation of atrial flutter due to tick-borne illness is rare and poorly understood. Further studies on tick-borne illness due to E chaffeensis may be needed to understand the systemic causes of the bacteria. In addition, in our case report, we bring to attention the standard presentation (symptoms, signs, and laboratory values) of tick-borne illness due to E chaffeensis along with the current standard for diagnosis and treatment.
Introduction
The number of Ehrlichia cases due to Ehrlichia chaffeensis reported to the Centers for Disease Control and Prevention (CDC) has increased steadily since the first year of disease reporting. In the year 2000, only 200 cases of ehrlichiosis were reported, while in 2018, 1799 cases were reported by the CDC.
Ehrlichiosis is the general name used to describe diseases caused by the bacteria E chaffeensis, E ewingii, or E muris eauclairensis in the United States. The majority of reported cases are due to infection by E chaffeensis as per the CDC. Ehrlichiosis used to be known as human monocyte ehlrichisosis, but this term is no longer used. Human disease due to Ehrlichia was only recognized in the late 1980s as per the CDC. Since then more number of cases and different clinical manifestations are being reported.
Ehrlichiosis can present with a varied clinical picture. Early signs and symptoms, usually within the first week of the tick bite, include fever, headaches, muscle aches, and rash. As per the CDC, about 1 in 3 people with ehrlichiosis present with a rash, although it may be more common in children. The highest reported rates of ehlrichiosis include Mississippi, Oklahoma, Tennessee, and Arkansas.1,2
Case
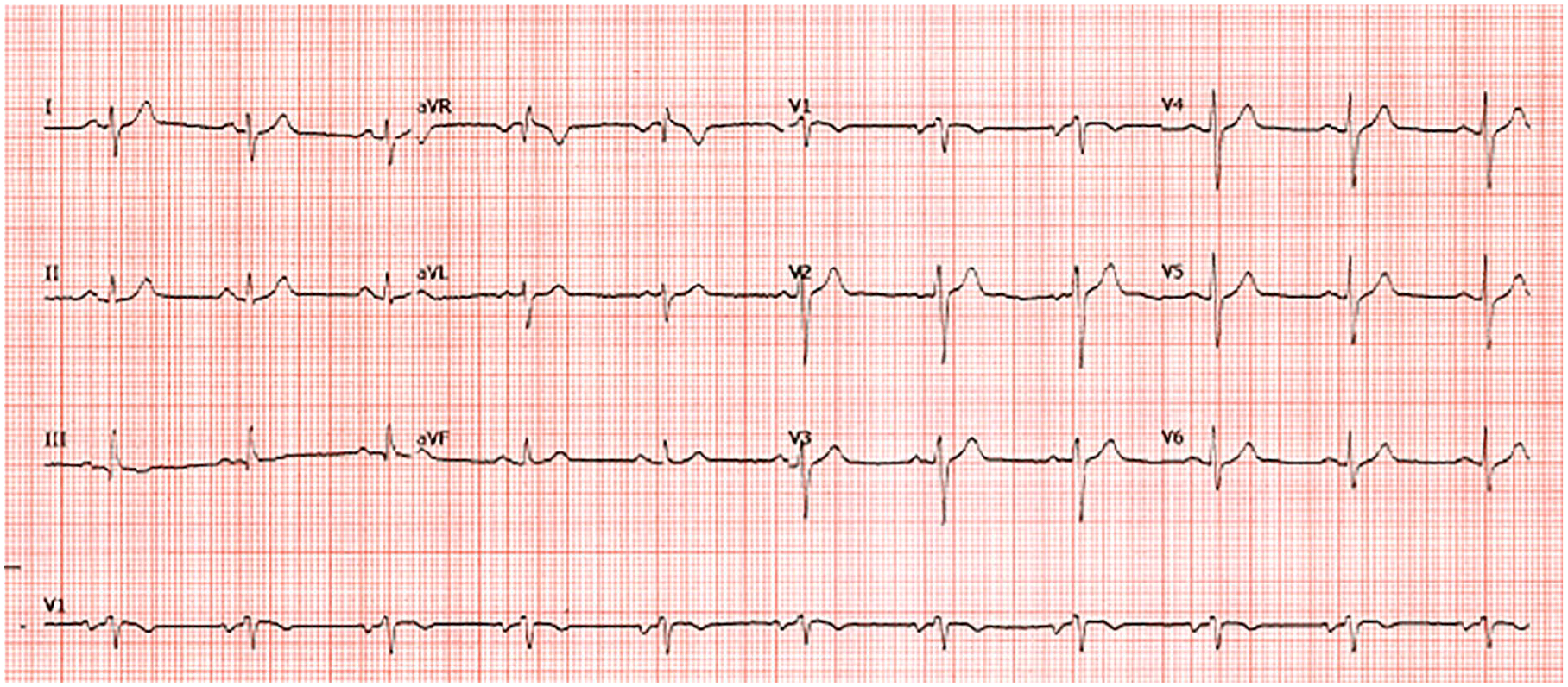
A 46-year-old Caucasian male from Arkansas with a past medical history of multiple sclerosis, plaque psoriasis presented with generalized weakness of 1 week duration. He also had associated fever and chills for the past day. He did admit to multiple tick bites (2 days ago) from recent travel in Arkansas prior to the symptoms starting. He does not know the duration of tick attachment and did not notice any engorged ticks on removal. On examination, he had a fever of 100.5 °F and a heart rate of 70 beats per minute that was irregularly irregular. Significant laboratory values include a white blood cell count of 4200/µL with 77% neutrophils, platelets of 83 000/µL. Sodium was 131 mEq/L. His BUN (blood urea nitrogen) was 12 mg/dL and creatinine was 1.4 mg/dL. Liver enzymes were within normal limits. Electrocardiogram (EKG) obtained showed variable block atrial flutter with heart rate <100 beats per minute (prior EKG showed normal sinus rhythm; Figure 1). The patient was treated empirically with doxycycline, intravenous fluids, and metoprolol tartrate. E chaffeensis immunoglobulin M (IgM) Ab was positive with titers >1:40 consistent with tick-borne illness due to E Chaffeensis. The patient’s symptoms improved over the next couple of days and eventually discharged. Repeat EKG 1 month later showed normal sinus rhythm (Figure 2).

Electrocardiogram showing variable block atrial flutter.
Electrocardiogram 1 month later showing resolution of atrial flutter.
Discussion
Ehrlichia chaffeensis is an obligate intracellular bacterium that belongs to the family Anaplasmataceae. The main vector for E chaffeensis in the United states and in Arkansas is the lone star tick, Amblyomma americanum.3,4 White tailed deer (Odocoileus virginianus) are the main reservoirs for the E chaffeensis in Arkansas 5 and usually remain persistently infected by the bacteria. 6
Ehlrichiosis can present with an early- and late-stage disease. The early stage, within a week of the tick bite, presents with symptoms of fever, muscle aches, headache, and rash. The rash of ehrlichiosis is usually described as a red splotch or pinpoint red dots. The classic associated laboratory abnormalities include anemia, leukopenia, thrombocytopenia, and elevated liver enzymes.7,8 In the late stage of the disease, usually after 2 to 3 weeks of illness, patients can present with severe disease manifested as acute respiratory distress syndrome, meningoencephalitis, seizures, and multi-organ failure. 8 Early antibiotics use significantly reduces the risk of progression to severe disease state. 8
The diagnosis of E chaffeensis is usually made based on the history of a tick bite or exposure to an area with ticks known to cause ehrlichiosis, the presence of signs and symptoms of infection, and pathognomonic laboratory findings. Confirmatory laboratory diagnostic tests include polymerase chain reaction (PCR; sensitivity decreases if done after administration of antibiotics 7 ) and immunofluorescence antibody (IFA) for IgG. The IFA IgG and PCR are collected from serum samples. The IFA IgG is sometimes paired with IgM antibodies, is considered the gold standard, and is the most commonly used confirmatory test. 9 As per the CDC, the presence of antibodies, particularly IgM antibodies in the absence of clinical symptoms and signs, reduces the diagnostic value remarkably. The IgG antibody is often negative within the first week of acute illness. 3 Negative serological markers does not exclude the diagnosis, especially during an acute illness. 3 A single IgG titer of at least 256, seroconversion from negative to positive antibody status (with a minimum titer of 64), and a 4-fold rise in titer during convalescence is highly supportive of the diagnosis (Table 1).10,11
Timeline of diagnostic laboratory laboratory values in ehlrichiosis.

Abbreviations: PCR, polymerase chain reaction; Ig, immunoglobulin.
Doxycycline is the drug of choice for treatment of tick-borne illness, usually dosed at 100 mg per os twice a day for a period of 3 to 5 days after symptoms of acute illness of fever have resolved. 9 For those with central nervous system involvement, a longer duration of treatment of 10 to 14 days is recommended. 9
Tick-borne illness including E chaffeensis is a primarily diagnosis based on history and clinical and laboratory findings, which may be confirmed by PCR, IFA-IgG, and IgM. Although the classic clinical presentation is well known, this illness can present atypically as in this patient who presented with atrial flutter in the setting of acute tick-borne illness. The incidence of tick-borne illness due to E chaffeensis is on the rise. Atypical and novel presentations of the illness continue to be reported.
Ehrlichiosis affecting the cardiovascular system is rare. Some of the cardiovascular manifestations due to ehlrichiosis that have been reported based on our literature search are listed in Table 2.
Case reports on cardiac manifestations due to ehrlichiosis.

Abbreviations: AST, aspartate aminotransferase; ALT, alanine aminotransferase; EKG, electrocardiogram; PCR, polymerase chain reaction; MRI, magnetic resonance imaging.
In ehrlichiosis, the host systemic inflammatory response rather than direct effects of the pathogen is likely to be largely responsible for many of the clinical manifestations of ehrlichiosis. 18 Unlike RMSF (Rocky mountain spotted fever), direct vasculitis and endothelial injury is rare in ehrlichiosis. 10 The pathophysiology on how the bacteria cause atrial fibrillation or atrial flutter is unclear, thus warranting further understanding on these mechanisms. With case reports showing evidence of myocarditis and pericarditis related to ehrlichiosis, this could be a potential pathophysiological mechanism for underlying cardiac manifestations related to ehrlichia but more studies would be warranted to confirm the diagnosis.
In Lyme carditis, animal studies in both monkeys and mice have shown that inflammation within heart is seen transmurally, which is predominantly macrophage and lymphocyte infiltrates. 19 However in Lyme carditis, atrioventricular conduction block of varying severity was the most common manifestation.20,21
With the number of cases of ehrlichiosis on the rise, this case teaches the clinician another rare cause of new-onset atrial fibrillation and/or flutter could be due to E chaffeensis–associated illness. One particular cause of an increasing incidence of tick-borne illness in the southern states of the United States has been attributed to the increasing population of white tailed deer, which serves as a natural reservoir for the bacteria. 22 Early identification of the illness based on history, signs and symptoms, and laboratory findings warrants treatment with antibiotics to prevent complications of late illness, which can be severe.
Prevention of tick bites by avoidance and immediate removal of ticks remains the best approach 2 for prevention of the illness. Studies have shown the tick requires at least 4 to 24 hours of attachment to transmit the disease and therefore immediate removal is the mainstay of prevention. 23 There has been no evidence for preventive antibiotic treatment in those who are not ill. 1
Footnotes
Authors’ Note
This case has been presented as a poster presentation at the Southern Society of Clinical Investigation (SSCI)—Southern chapter in February 2020.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Verbal consent was obtained from the patient regarding publication of the case report.