
Abstract
With the ameliorated resectability prowess of endoscopic techniques, a myriad of diseases previously treated by major ablative surgeries are now endoscopically curable. Endoscopic submucosal tunnel dissection (ESTD) is a relatively new technique that has diversified endoscopic application. Although ESTD has frequently been used for the resection of esophageal neoplastic lesions, the clinical evidence pertaining to its efficacy in the treatment of circumferential Barrett’s esophagus remains sparse. In this study, we evaluated ESTD as a potential therapeutic technique in patients with Barrett’s esophagus-related high-grade dysplasia. The tunneling strategy helped achieve complete en bloc resection at an increased dissection speed, without any procedural complications. This article illustrates that ESTD can be a feasible, safe, and effective treatment for dysplastic Barrett’s esophagus. Future research should aim to stratify the potential risks and complications associated with this optimization of endoscopic submucosal dissection in patients with superficial esophageal lesions.
Keywords
Introduction
Barrett’s esophagus has been estimated to affect up to 1% to 2% of the adult population in Western countries.1,2 It is disconcerting that 7% to 19% of patients with high-grade dysplasia in Barrett’s esophagus may progress to esophageal adenocarcinoma.3,4 Endoscopic therapy is preferred in these patients as it circumvents the morbidity and mortality associated with surgical intervention. 5 Due to curative resection and lower recurrence rates, endoscopic submucosal dissection (ESD) has gained precedence over endoscopic mucosal resection (EMR) for dysplastic lesions and early esophageal neoplasms. 6 Conversely, the widespread use of conventional ESD for the management of Barrett’s esophagus has frequently been hindered due to its relatively long procedure times, technical complexity, steep learning curve, and potential risk for serious adverse events. 6 While treating esophageal lesions, endoscopists may also face difficulty in scope manipulation owing to the thinness of the muscularis propria and the narrow luminal diameter of the esophagus. These factors increase the risk of perforation, rendering the uptake of conventional esophageal ESD a challenge. Therefore, optimization of ESD is warranted to mitigate these disadvantages, especially in patients with circumferential esophageal lesions.
Endoscopic submucosal tunnel dissection (ESTD) is a relatively new technique that affords faster dissection when compared with conventional ESD. 7 The effectiveness of tunneling strategy has been demonstrated in the treatment of a multitude of gastrointestinal lesions. 8 However, published medical literature pertaining to its therapeutic applications for high-grade dysplasia secondary to circumferential Barrett’s esophagus remains limited. In this study, we attempted tunneling technique in patients with Barrett’s dysplasia, resulting in curative resection. Given the technical feasibility and better clinical outcomes, we propose that ESTD can be an alternative endoscopic treatment for circumferential Barrett’s esophagus. We hope this article serves to enable clinicians the ability to stratify procedural risks and complications of this technique to select candidates in future and spare such patients from esophagectomy.
Patients and Methods
Case 1
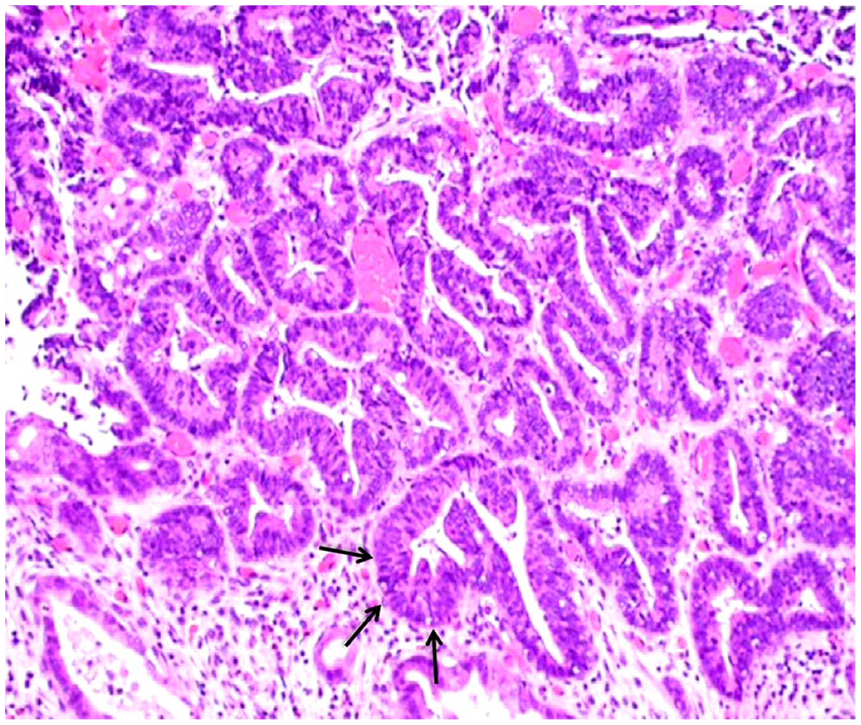
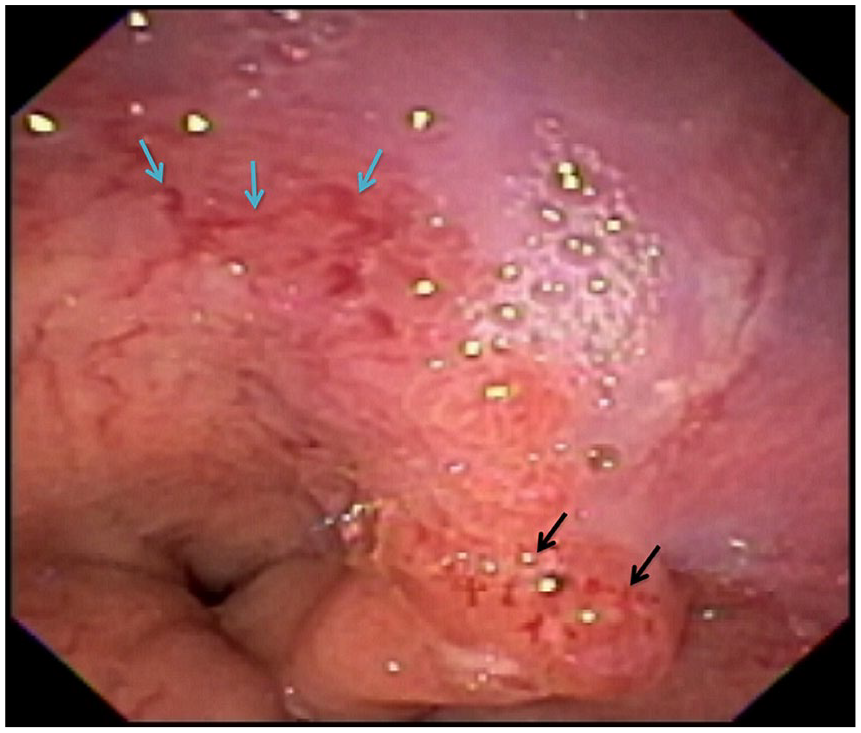
An 85-year-old male with a history of hypertension and benign prostatic hyperplasia underwent evaluation of his previously diagnosed Barrett’s esophagus. His prior endoscopies showed salmon-colored nodular mucosa, with a Paris classification phenotype of 0-IIa+IIc, located at 23 to 35 cm from the incisors (Figure 1). Biopsy confirmed multifocal high-grade dysplasia, with no evidence of carcinoma (Figure 2). The patient was considered a suitable candidate for surgical intervention but he refused the procedure due to the associated risks. As it was a 12-cm long, high-grade, nodular dysplastic Barrett’s lesion, radiofrequency ablation could not form the initial optimal treatment. Due to his favorable geriatric performance status, a multidisciplinary team with expertise in surgery and advanced endoscopy recommended ESTD. The patient was educated about this treatment modality. Informed consent was obtained after discussing benefits and risk of potential complications such as perforation, bleeding, and stenosis associated with circumferential submucosal dissection. Ethical approval was duly obtained for the modification of the conventional ESD procedure.

Endoscopic appearance of the esophagus demonstrating nodular mucosa, extending from 23 to 35 cm from incisors. The Paris classification type was 0-IIa+IIc, indicating superficial elevated lesions (black arrow) as well as areas with central depressions (blue arrow).

Histopathologic examination of the biopsy specimen from nodular esophagus showing Barrett’s mucosa with high-grade dysplasia (arrows), but no evidence of malignancy (hematoxylin and eosin staining; 400×).
A forward-viewing endoscope (GIF-H180; Olympus) with a transparent cap (MH-588; Olympus) was advanced to the lesion. The proximal and distal margins of Barrett’s esophagus were marked with DualKnife (Olympus). Submucosal solution was injected and a 2-cm horizontal mucosal incision was made in the posterior wall. With the use of repeat submucosal injection and DualKnife, a posterior submucosal tunnel was created, extending up to the gastroesophageal junction. Similarly, an anterior submucosal tunnel was created. After partially extending the anterior tunnel to the posterior tunnel on the left side, a circumferential mucosal incision was made near to the gastroesophageal junction using DualKnife, which removed the distal mucosal portion. The anterior tunnel was then extended posteriorly on the right side, creating a 360° tunnel. The proximal mucosal incision was extended circumferentially using a combination of Dual and HookKnife electrocauteries (Olympus). Proximal residual Barrett’s mucosa was then dissected. It resulted in the en bloc removal of the 12-cm long, circumferential dysplastic esophageal lesion (Figure 3).

Gross morphology of the esophageal lesion after en bloc circumferential removal using endoscopic submucosal tunnel dissection.
During and after the completion of ESTD, only one actively oozing visible blood vessel was identified. The coagulation was successfully performed with coagulating forceps (Coagrasper, FD-410L; Olympus). A fully covered metallic esophageal stent (Boston Scientific) was placed across the ESTD base and was secured by endosuturing (Supplementary File; Video 1, available online). Postprocedural barium swallow showed no evidence of a filling defect (Figure 4). Pathologic analysis of the resected specimen confirmed dysplastic Barrett’s mucosa, with no neoplastic changes (Figure 5). The horizontal and vertical margins of the resected specimen were free of Barrett’s mucosa.

Postprocedural barium swallow showing no visible evidence of a leak.
The histopathologic analysis of the resected specimen confirmed the presence of dysplastic Barrett’s mucosa (arrows) and there was no evidence of malignancy (hematoxylin and eosin staining; 400×).
Case 2
An 81-year-old male presented to our hospital for the evaluation of Barrett’s esophagus (Prague C3M4), noted at 41 to 44 cm from the incisors. Upper endoscopy showed a mass lesion, morphologically consistent with the Paris classification type of protruding sessile (Is), noted at 42 to 44 cm from the incisors (Figure 6). The gastroesophageal junction mass was located at 4 to 5 o’clock position (Figure 7). On endoscopic ultrasonography, the lesion was mucosal-based, with no regional lymphadenopathy. Biopsy results confirmed high-grade dysplasia in Barrett’s esophagus. The patient was mobile with good geriatric performance status but refused surgical intervention. Given the nodularity and high-grade dysplasia in Barrett’s esophagus, radiofrequency ablation was not considered the optimal first treatment. Based on a multidisciplinary input, it was decided to treat the lesion using ESTD. This therapeutic option was explained to the patient. Informed consent was obtained after discussing the risks, benefits, and limitations of ESTD. Ethical approval was also obtained prior to the procedure.
Upper endoscopy showing Barrett’s esophagus (Prague C3M4), located at 41 to 44 cm from the incisors (blue arrows). A dysplastic mass lesion noted at 42 cm from the incisors (black arrows), the morphology of the lesion was consistent with the Paris classification type, protruding sessile (Is).

Endoscopic features of the gastroesophageal junction dysplastic mass located at around 4 to 5 o’clock position (arrows).
A forward-viewing endoscope (GIF-H180; Olympus) was used to inject submucosal solution into the posterior wall and a linear horizontal mucosal incision was made at 40 cm. Posterior submucosal tunnel was created using DualKnife (Olympus) and was extended into cardia up to 45 cm. Submucosal solution was then injected into the anterior wall. A linear, horizontal, mucosal incision was made; anterior submucosal tunnel was created and extended into cardia. A near-circumferential mucosal incision was made in cardia at 45 cm using a DualKnife in a retroflexed position. Submucosal solution was then injected starting in the right and left positions. After making a linear horizontal mucosal incision, complete submucosal tunnel was created, and extended into cardia. The lesion was now hanging near cardia. After repeat submucosal injection, the lesion was removed with a combination of HookKnife and snare cautery (Olympus). During the last part of dissection, the lesion broke into 2 large and 2 smaller pieces. All pieces were retrieved and placed on gel foam. The resected specimens were sent for histopathologic examination.
A pair of coagulating forceps (Coagrasper, FD-410L; Olympus) was used to coagulate residual vessels at the ESTD base. In order to prevent restenosis, 80 mg of triamcinolone was injected at different spots in the ESTD base. As a precautionary measure against delayed bleeding, 5 mL of human plasma-derived fibrin sealant (EVICEL) was also sprayed at the ESTD base. The en bloc removal of the mass lesion along with the Barrett’s mucosa from 40 to 45 cm from the incisors was completed without any potential complications. Pathologic examination of the resected specimens confirmed negative horizontal and vertical mucosal resection margins for Barrett’s esophagus.
Outcomes and Follow-up
In Case 1, the total procedural time was 105 minutes. The patient was discharged from the hospital in a stable condition after 2 days of endoscopic curative resection. He recuperated rapidly in the aftermath of the ESTD treatment, with prompt improvement in his clinical condition. At the 1-week follow-up, he had no complaints and was tolerating solid food. The esophageal stent was removed after 2 months. At the 6-month follow-up, the patient developed a post-ESTD mild, short distal esophageal stricture that was easily managed by balloon dilation. Endoscopic examination, at the 12-month follow-up visit ruled out recurrence. At the subsequent endoscopic follow-ups as per the postresection surveillance guidelines of the American Society of Gastrointestinal Endoscopy for Barrett’s esophagus-related high-grade dysplasia, no complications or recurrence was evident. The patient continues to do well to date, totaling 5 years and 3 months.
In Case 2, the whole procedure took 60 minutes, with no immediate periprocedural complications. His length of hospital stay was also short, comprizing of 2 days. The subsequent endoscopic follow-ups at 3, 6, 9, 12, and 18 months ruled out recurrence, stricture, or any other delayed procedural complications, with a total follow-up duration of 1 year and 11 months. He continues to be symptom-free, with no evidence of recurrence of the disease thus far. In both cases, no residual dysplasia or intestinal metaplasia was noted on surveillance endoscopic biopsies.
Discussion
Linghu et al first coined the term endoscopic submucosal tunnel dissection in 2013 after they published their research regarding the use of tunnel technique for large circular early esophageal cancer. 9 At present, the application range of this technique covers a variety of gastrointestinal disorders. The lesions, such as superficial esophageal squamous cell carcinoma, esophageal leiomyoma, large esophageal mucosal lesions, submucosal esophageal and gastric precancerous lesions, ulcerative early gastric cancer, lesser gastric curvature superficial neoplasms, intramural esophageal bronchogenic cysts, giant colorectal subpedunculated neoplastic lesions, colorectal lateral spreading tumors, and large superficial rectal neoplasms, are shown to be amenable to ESTD.10-12 Recently, a few studies also reported the use of a concoction of the tunnel technique and the clip-with-line traction method to perform esophageal ESD for the treatment of superficial esophageal neoplasms.13,14 However, in patients with circumferential Barrett’s-associated high-grade dysplasia, the application of tunneling technique remains limited. The present study further adds to the existing clinical evidence and highlights the efficacy of ESTD in the treatment of Barrett’s esophagus.
In comparison to conventional ESD, ESTD has a higher dissection speed, yields fewer adverse events, and has better curative rates. The backbone of this technique is the creation of a submucosal tunnel to secure a working space. It provides a “good view” for dissection that ultimately helps in the lateral stretching of the mucosa. Air insufflation is of relative ease and the effect of submucosal injection is prolonged. 10 Major benefits of tunnel creation include the prevention of mucosal collapse due to the intratunnel pressure and easier identification of proper submucosal cutting planes. 15 Imperatively, the tunneling greatly decreases the time required for wound healing. Furthermore, the risks of perforation and gastrointestinal infection are significantly decreased. 10 ESTD is also associated with a relatively shorter hospital stay and low recurrence rates, making it more feasible. 5 In this study, the total hospital stay in Cases 1 and 2 was 2 days, respectively.
The risk of peri- or postprocedural hemorrhage ranges from 0% to 5.9% in ESTD. 10 However, the provision of a better visual field makes primary hemostasis easier to achieve in ESTD than conventional ESD. 16 If bleeding occurs in the submucosal tunnel, it can be controlled by pressing the bleeding point by tip of the endoscope. After preparing for hemostasis, the pressing is released and coagulation of the bleeding point can be performed by hemostatic forceps. 17 Therefore, a vast majority of patients with minor bleeding can be effectively managed using the aforementioned method in the submucosal tunnel. Even though major bleeding events are extremely rare, identification of the culprit vessel with water jet followed by blind coagulation with hemostatic forceps might be warranted in some patients. Endoscopic hemoclip placement may also be used to curb bleeding from large residual vessels if conservative treatment fails to secure hemostasis. 17 Although reactionary hemorrhage rarely occurs after ESTD, it can usually be managed endoscopically. 17
Perforation remains an important potential complication of ESTD, with an estimated risk of up to 4%.10,18 When it occurs, the perforation usually measures <10 mm and can easily be controlled with metal clipping. Multiple clips in a zipper fashion are preferred to achieve complete closure. A recent over-the-scope clip (OTSC) technique may secure up to a 20-mm perforation with adequate compression impact. 18 The larger defects are managed with fully covered self-expandable metal stents, but their migration may pose a challenge. 19 Surgery can be indicated if endoscopic closure fails, patients develop severe mediastinal infection, and/or in the setting of hemodynamic compromise. In this study, the total procedural blood loss in Cases 1 and 2 was <5 mL, respectively. Delayed bleeding and perforation were effectively ruled out by the post-procedure endoscopy and barium-swallow.
Postprocedure stenosis or stricture formation can be a particularly debilitating complication. In a study of 84 esophageal ESD patients, the stenosis rate of ≥3/4 circular lesions was 90%. 20 Therefore, the prevention of this adverse event after circumferential ESTD should be considered exceedingly imperative. Chai et al 10 suggested a fully covered metal stent placement for a period of 4 to 8 weeks. Furthermore, hormone injection or oral administration, balloon dilatation, endoscopic radical incision, auto balloon dilatation, and autoplastic flap transplantation are among other commonly used methods in clinical practice.20-22 However, no standard therapy is available to prevent postoperative stricture after ESTD. In this study, we deployed an esophageal stent in Case 1, whereas a steroid injection was administered in Case 2. The patients showed excellent clinical recovery with resolution of their prior symptoms. At the subsequent follow-ups, the first patient showed a mild stricture formation after stent removal, which was successfully treated with endoscopic balloon dilatation. The second patient had no signs of gastrointestinal blood loss or stricture formation at long-term follow-up.
With regard to post-resection surveillance in patients with dysplastic Barrett’s esophagus, current guidelines of the American Society of Gastrointestinal Endoscopy are largely based on expert opinion and low-quality clinical evidence. 23 Initial endoscopic evaluation at 3 to 6 months after achieving complete eradication of intestinal metaplasia (CE-IM) is recommended followed by surveillance intervals on the basis of pretreatment histopathologic features. In patients with baseline detection of high-grade dysplasia, surveillance endoscopic examination every 3 months in the first year after CE-IM followed by endoscopies every 6 months in 2 years followed by yearly endoscopies has been suggested. In cases with low-grade dysplasia who have achieved CE-IM, the most recent guidelines suggest surveillance every year for 2 years and then every 3 years. 24 The guidelines favor the histologic confirmation of recurrent intestinal metaplastic or neoplastic changes by surveillance biopsy sampling after achieving CE-IM.25,26 The patients involved in this study underwent endoscopic post-ESTD surveillance in accordance with the aforementioned guidelines. At the follow-up visits, no clinical or endoscopic evidence of recurrence was noted in these patients. Surveillance endoscopic biopsies ruled out residual dysplasia or intestinal metaplasia in both the cases. Thus, ESTD emerged as a safe and efficacious modality for the excision of dysplastic epithelium in Barrett’s esophagus.
Learning Points
ESTD can be considered a part of the armamentarium for the management of Barrett’s esophagus.
It allows the en bloc resection of the large and circumferential dysplastic Barrett’s mucosa, with relatively shorter dissection time and decreased incidence of intraoperative complications than conventional ESD.
Given the low risk of recurrence and fewer adverse events, this organ-sparing technique may-be beneficial over other endoscopic treatments and surgical resection, especially in patients with Barrett’s-related high-grade dysplasia.
This case series prompts endoscopists to conduct further studies on the long-term efficacy of ESTD. The comparison of this technique with other interventional therapies for Barrett’s esophagus is also warranted.
Footnotes
Acknowledgements
We would like to express our gratitude to Ms Eman Shahzad and Mr Arham Razzaq, who helped us in preparing the manuscript.
Authors’ Note
This paper was presented as an abstract at the Digestive Disease Week, May 21-24, 2016, in San Diego, CA, USA.
Author Contributions
FI: conception and design of the study, the acquisition, analysis, and interpretation of data for the work, performing the literature review, and drafting, reviewing, and revising the manuscript critically for important intellectual content. SW: contribution to the case presentation, drafting and reviewing the manuscript. AM: performing the literature review, contribution to the discussion, and revision of the manuscript. BM: reviewing the literature and contribution to the discussion and drafting of the manuscript. SI: reviewing the manuscript, suggesting pertinent modifications, and drafting and revising the work. All authors read and approved the final manuscript, and are accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.