
Abstract
Choledochoduodenal fistula (CDF) is an abnormal communication between the common bile duct and the duodenum. It accounts for about 5% to 25% of the total biliary fistulas and is usually due to a perforated duodenal ulcer, choledocholithiasis, and complications secondary to tuberculosis or could be iatrogenic. Primary intrabilliary tumors usually cause obstructive jaundice and rarely biliary metastasis arising from other organs like colon, breast, and lungs can cause obstructive jaundice. There has been a case report of metastasis from ovarian cancer to the major papilla of the duodenum but no reported cases of it causing a CDF. We report a rare case of an 83-year-old female with ovarian cancer who developed a metastatic lesion to the duodenum eventually resulting in a CDF.
Keywords
Case Report
An 83-year-old African American female with chronic kidney disease, high-grade serous carcinoma of the ovary status post-surgery and chemotherapy, untreated Hepatitis C, and duodenal ulcer. She was started on adjuvant chemotherapy in February 2013 and completed a total of 6 cycles of carboplatin/taxol in June 2013. The patient was last seen in Oncology clinic in 2015 for surveillance, and imaging computed tomography (CT) chest, abdomen, and pelvis did not show any evidence of recurrence and she was deemed to be in complete remission. She then returned to the clinic in 2018 and was admitted initially for fever, altered mental status, and constant generalized abdominal pain of 4 days duration. The admission vital signs were stable. Routine laboratory tests were performed on admission that was unremarkable except for normocytic anemia with hemoglobin of 7.8 mg/dL and mild prerenal acute kidney injury with a creatinine of 1.5 (baseline 1.3). Examination showed diffuse abdominal tenderness with negative Murphy’s sign. CT abdomen showed distended gallbladder with gallstones, dilated intra- and extrahepatic bile ducts, and pneumobilia. Magnetic resonance cholangiopancreatography showed similar findings. Due to concerns for cholangitis, an urgent endoscopic retrograde cholangiopancreatography (ERCP) was performed for a sphincterotomy and stent placement. ERCP also revealed a 13-mm duodenal ulcer superior to the major papilla and a high-grade obstruction in the proximal common bile duct (CBD) indicative of a stricture. Concomitant fluoroscopy showed that the location of the ulcer was in approximation to the high-grade stenosis of the proximal CBD, suggestive of duodenal ulcer (inflammatory vs malignancy) causing CBD stricture and the pneumobilia. After the stent placement, the patient was discharged home in a stable condition. The pathology of the biopsies taken from the ulcer site revealed small bowel mucosa with fibrosis, chronic inflammation, and reactive epithelial changes without any evidence of malignancy.
Seven months later, the patient was readmitted with melena of 3 days duration. On admission, the heart rate was 120 beats per minute and a hemoglobin of 5.6 mg/dL. The esophagogastroduodenoscopy (EGD) revealed progression in the size of the necrotic duodenal ulcer seen in the first part of the duodenum with a possible fistulous tract. There was no active bleeding seen on EGD. Helicobacter pylori testing was negative, and no apparent cause of the ulcer was known. Serum tumor markers revealed high CA 125 (162.2 U/mL) and α-fetoprotein (7.6 ng/mL), but normal carcinoembryonic antigen and CA 19-9. Magnetic resonance imagining of the abdomen showed a fluid collection around the duodenum and pancreatic head with a possible CDF. Repeat EGD was done to biopsy the fistula and pathology were consistent with poorly differentiated serous carcinoma with morphology and immune profiling consistent with the initial high-grade serous carcinoma of the ovary (Figures 1-5).

Esophagogastroduodenoscopy showing duodenal ulcer.
Endoscopic retrograde cholangiopancreatography showing biliary stenosis, common biliary duct stricture.

Repeat esophagogastroduodenoscopy (EGD) showing duodenal fistula. Second portion duodenum was carefully viewed using the standard EGD followed by the side-viewing duodenal scope: protruded major papilla with previously placed common bile duct stent seen extending into the duodenal lumen. A small fistula with brown, particulate fluid content likely bilious fluid flowing into the duodenal lumen was seen at approximately 2 duodenal mucosal folds superior or proximal to the major papilla.

Magnetic resonance cholangiopancreatography showing fistula. Soft tissue, fluid, and gas collection centered within the region of the duodenum/pancreatic head with suggestion of communication with the common bile duct. This may reflect a duodenal ulcer complicated by choledochoduodenal fistula and/or abscess.

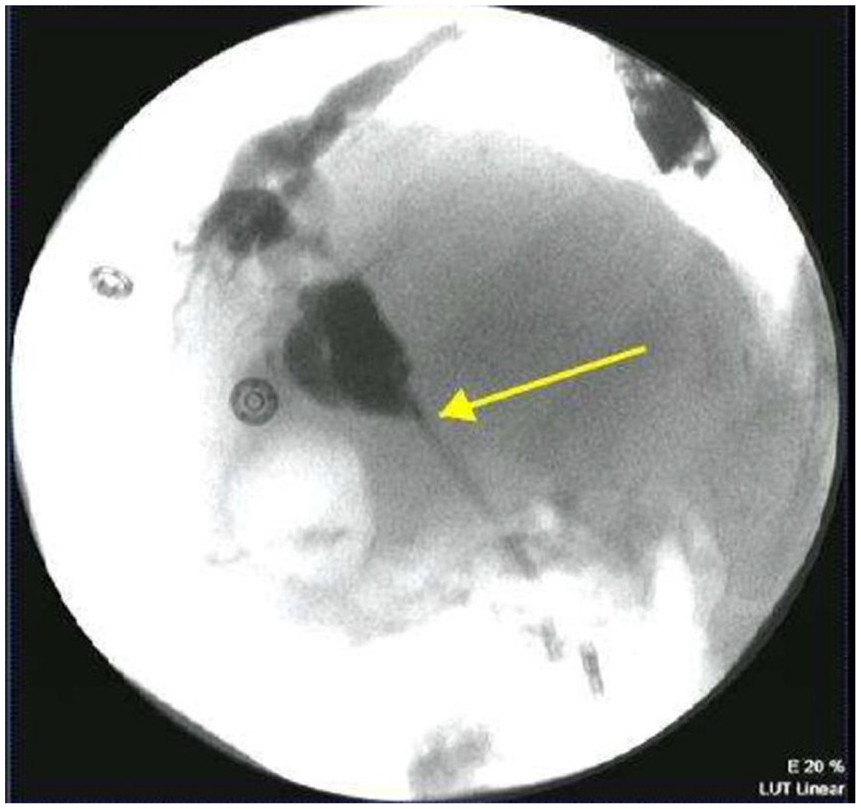
Computed tomography of abdomen and pelvis showing pneumobolia in the left lobe of the liver.
The CT of abdomen and pelvis revealed peritoneal metastatic disease surrounding the distal CBD and probable right pleural metastasis. Oncology recommended Caris molecular intelligence testing of recent biopsy to determine if she could be a candidate for targeted therapy. The patient was a poor surgical candidate and different treatment options were discussed with the family and the patient including (1) expectant management with palliative care, (2) chemotherapy with carboplatin, and (3) Caris determined targeted therapy. At the time, the patient and family decided to wait until the results of Caris returned before making a decision. However, even before the results of molecular testing were back patient decompensated acutely and developed multiple complications. She had a small bowel obstruction and multiple pulmonary emboli requiring anticoagulation. Her course was complicated by a major gastrointestinal bleed and bilateral hydronephrosis. After a discussion with the family, it was decided to take her home with hospice to minimize her suffering and make her comfortable.
Discussion
Spontaneous biliary tract fistula is a rare entity, with cholecystoduodenal (61% to 77%) being the commonest followed by cholecystocolonic (14% to 17%) and cholecystogastric (6%), and the least common is the choledochoduodenal type. 1 They are caused by gallstones (90%), peptic ulcer disease (6%), and malignancy or trauma (4%).1,2 Patients with CDF lose the barrier of papilla so there is an exposure of the biliary system to gut flora and also chronic fluid and electrolyte wasting in the biliary system and malabsorption mimicking the symptoms of cholelithiasis. 3 It can also present as pneumobilia, the air in the biliary tree.
There have been a few reported cases of CDF from intrabiliary metastasis from distant organs such as adenocarcinoma of the colon. 4 Adenocarcinoma of the distal CBD 5 and intraductal papillary mucinous neoplasm of the bile duct 6 have also been known to cause a similar presentation of CDF. 5 Other malignancies including gallbladder cancer can also lead to a CDF. 3
Ovarian cancer is the second most common gynecologic malignancy and the most common cause of gynecologic cancer mortality in the United States. The most common epithelial ovarian cancer histologic subtype is the serous type. Approximately 90% of serous carcinomas are high grade, and 10% are low grade. For women with stage I, low-grade serous carcinoma, very little information is available in terms of prognosis. In a review of the Surveillance, Epidemiology, and End Results (SEER) data set, the mean overall survival for patients with stage I disease was 123 months; the median overall survival had not yet been reached, while women with high-grade serous carcinoma achieved an overall survival of 39 months.7,8
The clinical presentation of ovarian cancer is very varied, ranging from an asymptomatic adnexal mass to significant symptomatology including bloating, early satiety, urinary urgency, and abdominal or pelvic pain. In more advanced cases, women may also present with pleural effusion or bowel obstruction. The most common sites of distant metastases for ovarian cancer are liver, lungs, peritoneum, and lymph nodes. 9 Takasaki et al reported a case of mechanical jaundice in an ovarian cancer patient with metastasis to duodenal major papilla and did not have any evidence of CDF. 9 Our patient had metastasis to the duodenum from ovarian cancer, resulting in a duodenal ulcer and subsequent CDF leading to pneumobilia, which to our knowledge is the first reported case. The abundant lymphatic vessels in the duodenal papilla make it a possible cause for its spread.
The primary aim of the treatment is debulking, and resection of any residual tumor including distant metastases. Patients with disseminated disease undergo cytoreductive surgery to achieve minimal residual disease (ideally no gross residual disease) is the standard. In an analysis of Gynecologic Oncology Group women with grade 1 (low grade) and serous carcinomas were accrued. Women with microscopic residual disease post-surgery experienced a better progression-free survival (median, 97 vs 35 months) compared with women with residual disease >1 cm. 7
Conclusion
Our patient was a poor surgical candidate due to her age and multiple comorbidities. It is important to remember CDF as differential in patients presenting with pneumobilia or cholangitis symptoms. Early diagnosis of CDF and its surgical correction, especially in younger patients, can lead to better outcomes. CT and ERCP are the imaging modality of choice in these patients. Although further research is recommended to facilitate early diagnosis of these lesions given their fatal prognosis.
Footnotes
Authors’ Note
This article was presented as a poster at the Annual Scientific Meeting Abstracts, American College of Gastroenterology, held at San Antonio, Texas, on October 29, 2019.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
No ethical approval is needed by our institution to report individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.