
Abstract
Background and aim
Risk factors for progression of gastric atrophy have not been fully elucidated. The aim of this study was to evaluate the risk factors for the development of atrophic gastritis in patients with Helicobacter pylori (H. pylori ) infection.
Methods
We reviewed 206 H. pylori-infected patients retrospectively. Endoscopic gastric atrophy was classified into closed- and open-type. We conducted univariate and multivariate logistic regression analyses on the contribution of age, sex, body mass index, past history of cancer, the first-degree family history of gastric cancer, habitual smoking and alcohol drinking, and endoscopic findings of gastric ulcer or duodenal ulcer for open-type gastric atrophy.
Results
On multivariate analysis, age (odds ratio = 1.079, 95% confidence interval = 1.048–1.11, p < 0.001), family history of gastric cancer (odds ratio = 3.967, 95% confidence interval = 1.414–10.6, p = 0.006) and duodenal ulcer (odds ratio = 0.834, 95% confidence interval = 0.711–0.977, p = 0.024) were the factors independently associated with open-type gastric atrophy.
Conclusions
A first-degree family history of gastric cancer, absence of duodenal ulcer, and old age were independent risk factors for the progression of gastric atrophy among H. pylori-infected patients. Careful examination with upper gastrointestinal endoscopy is necessary in patients with such risk factors.
Introduction
Gastric cancer is one of the major causes of cancer deaths in the world. 1 Progression of gastric atrophy is one of the risk factors for gastric cancer among patients with Helicobacter pylori (H. pylori) infection.2,3 Although H. pylori infection seems to be a prerequisite for atrophic gastritis, not all H. pylori-infected patients will develop atrophic gastritis. Moreover, while some patients do progress to gastric cancer, others do not. Risk factors for the progression of gastric atrophy have not been fully elucidated. The aim of this study was to evaluate the risk factors for the development of atrophic gastritis in H. pylori-infected patients.
Methods
Subjects
Patients (N = 10,251) who underwent upper gastrointestinal endoscopy between January 2009 and December 2012 in Toyoshima endoscopy clinic were retrospectively reviewed. Five patients with gastric cancer history and a previous gastric surgery were excluded from the present study. H. pylori negative patients (n = 1563) and 675 patients who had received H. pylori eradication therapy were also excluded, despite failed eradication therapy; 8418 patients with an unclear status of H. pylori infection were also excluded.
Status of H. pylori infection
The status of H. pylori infection was assessed by 13 C-urea breath test, stool antigen analysis, or H. pylori-specific immunoglobulin G antibodies in the serum. 4 H. pylori infection was confirmed when any one of these tests was positive.
Questionnaire
All patients had provided detailed prior information and answered a structured questionnaire to assess personal and clinical data under the supervision of a well-trained interviewer. The questionnaire included questions on age, sex, body mass index (BMI), past history of cancer, the first-degree family history of gastric cancer, habitual smoking and habitual alcohol drinking.
Endoscopic diagnosis
Upper gastrointestinal endoscopy was performed by eight experienced endoscopists (OT, KS, HY, SY, KH, TK, SM, YI in Toyoshima endoscopy clinic). Endoscopic studies have reported that the area of atrophy in patients with chronic atrophic gastritis extends from the antrum to the corpus.5,6 Kimura and Takemoto divided gastric mucosal atrophy into six stages (C-I, C-II, C-III, O-I, O-II and O-III) based on the endoscopic evaluation. 7 It has been clarified that mucosal atrophy progresses sequentially from C-I to O-III. This endoscopic classification was consistent with the Sydney system of classification of gastric atrophy. 8 We defined gastric mucosal atrophy of stages C-I–C-III as closed-type and that of stages O-I–O-III as open-type. 9 Patients with an endoscopically identified gastric ulcer or ulcer scar were classified into the gastric ulcer group. An ulcer was defined as a localized defect in the gastric mucosa of at least 5 mm diameter and with perceptible depth, whereas smaller lesions were considered as erosions. 10 Similarly, patients with an endoscopically identified duodenal ulcer or ulcer scar were classified into the duodenal ulcer group.
Statistical analysis
We evaluated the effects of age, sex, BMI, past history of cancer, the first-degree family history of gastric cancer, habitual smoking, habitual alcohol drinking, gastric ulcer and duodenal ulcer on atrophic gastritis. The clinical parameters were analyzed by a univariate logistic regression analysis. The predictors found to be associated with open-type gastric atrophy on univariate analysis (p < 0.1) were subsequently assessed by a multiple logistic regression method to identify independent factors. Age and BMI were included as continuous variables in the univariate and multivariate logistic regression method. A p value of less than 0.05 was considered statistically significant. The data were analyzed using the Stat Mate IV software (ATOMS, Tokyo, Japan).
Ethics
The study was conducted with the approval of the Ethics Committee of external organization, and informed consent was obtained from all patients. The clinical trial registration number of the University Hospital Medical Information Network was R000018541.
Results
A total of 10,251 patients underwent upper gastrointestinal endoscopy. H. pylori infection status was confirmed in 1839 patients. We investigated 206 patients, after excluding 953 patients without H. pylori infection, 675 patients after H. pylori eradication and five patients with previous gastric surgery.
Characteristics of patients included in the present study
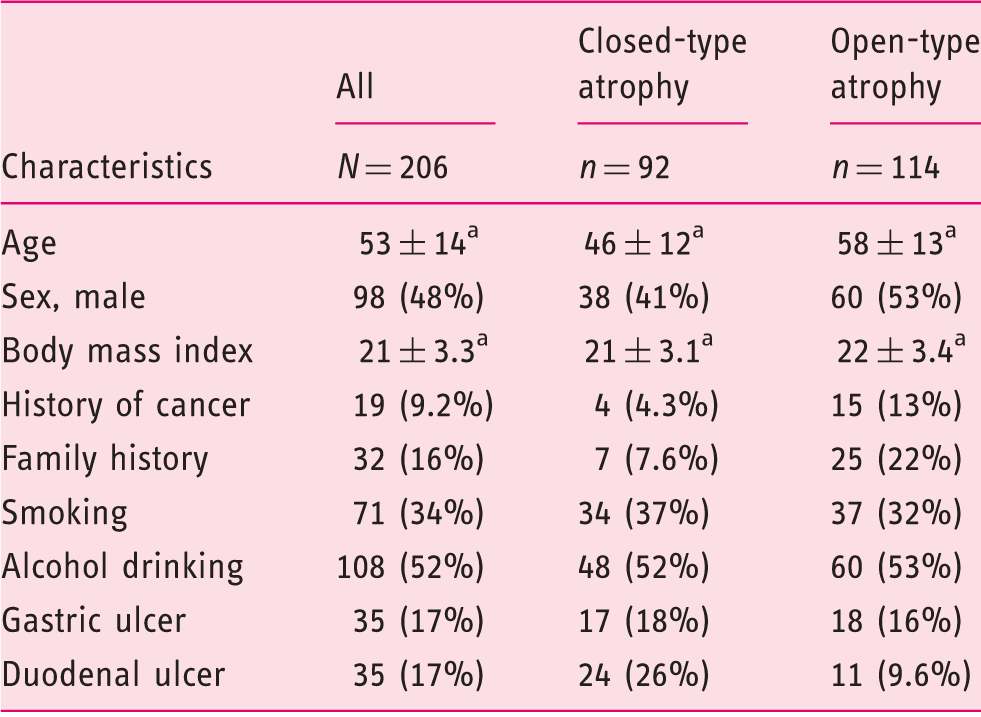
Mean ± standard deviation.
Univariate and multivariate analysis for open-type gastric atrophy
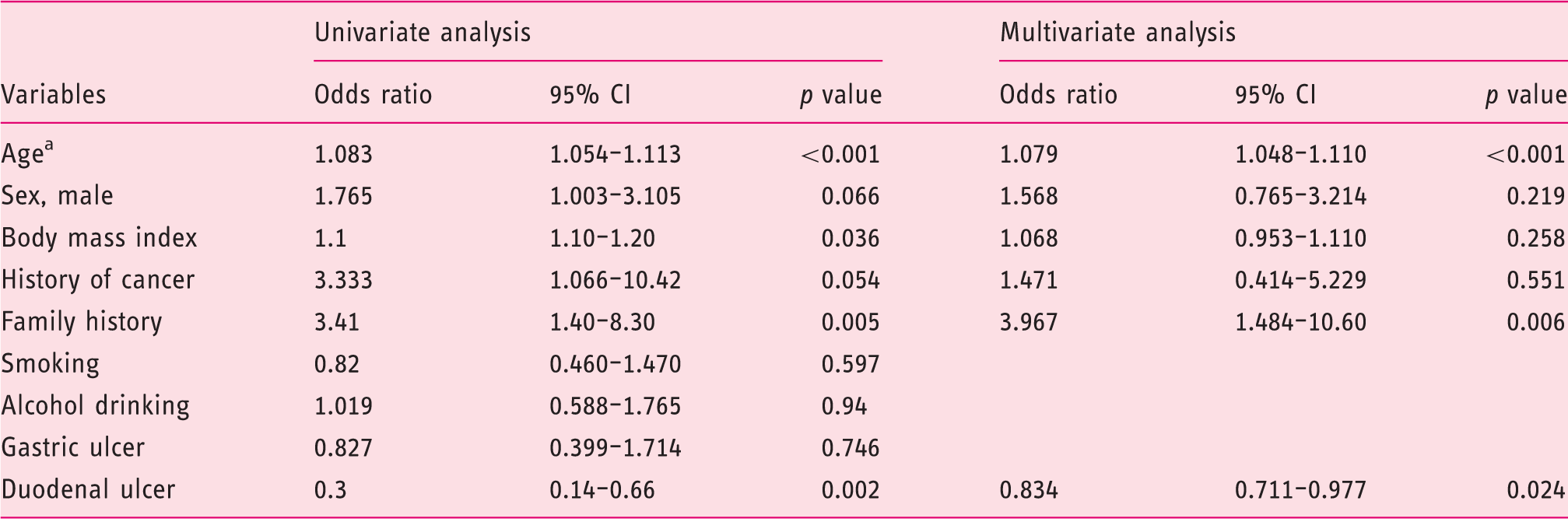
For each one year increment.
CI: confidence interval
Discussion
A first-degree family history of gastric cancer, absence of duodenal ulcer, and old age were independent risk factors for the progression of gastric atrophy among H. pylori-infected patients.
Some studies showed that the first-degree relatives of patients with gastric cancer and H. pylori infection have an increased risk of atrophic gastritis.11–14 However, other studies have failed to show a significant association.15–19 A recent meta-analysis reported the risk of first-degree relatives developing gastric cancer in comparison with controls who had no family history of gastric cancer. For gastric atrophy and H. pylori prevalence, the pooled odds ratios with 95% CI were 2.20 (1.266–3.824) and 1.925 (1.419–2.611), respectively. 20 First-degree relatives of gastric cancer patients had a significantly higher risk for developing gastric atrophy, and this paralleled with a significantly higher risk of harboring H. pylori. Most studies did not match the population by H. pylori infection status, although one study matched that in order to reduce confounding effects of H. pylori infection status. 18 Therefore, the role of family history as a risk factor for atrophic gastritis was not conclusive. The present study of H. pylori-infected patients clearly showed that family history was an independent risk factor for atrophic gastritis.
Tsukui et al. also reported that the presence of duodenal ulcers reduced the risk for atrophic gastritis in dyspeptic patients. 21 Some reports showed that the presence of duodenal ulcer reduced the risk of gastric cancer.9,22,23 Lu et al. reported that the presence of dupA gene was related to increased risk of duodenal ulcers, as well as that it provided increased protection against gastric atrophy and gastric cancer. 24 A recent meta-analysis confirmed the importance of the dupA gene for duodenal ulcers, 25 in line with our present study.
Our study showed that old age was an independent risk factor for the progression of gastric atrophy. It is believed that H. pylori infection is acquired during early childhood in the majority of the infected individuals. Therefore, aging reflects the duration of H. pylori infection. We previously reported significant improvements in gastric atrophy after H. pylori eradication therapy, especially in the earlier phase of infection.26–28 These results indicate that early eradication would be desirable.
The present study has several limitations. First, we did not assess other factors such as daily salt and nitrite/N-nitrosodimethylamine intake. 29 Dietary salt intake is directly associated with risk of gastric cancer, 30 and high consumption of nitrites and N-nitrosodimethylamine could increase the gastric cancer risk. 31 The questionnaire to assess daily salt and nitrite/N-nitrosodimethylamine intake has limited value, and it is difficult to estimate them. Second, gastric mucosal atrophy was diagnosed by endoscopic findings. Miwata et al. investigated interobserver and intraobserver agreement for endoscopic gastric mucosal atrophy using the Kimura–Takemoto Classification. The kappa value for the interobserver agreement in the experienced endoscopists was 0.474. The kappa value of intraobserver agreement in the experienced endoscopists ranged from 0.585 to 0.871. The interobserver agreement for gastric mucosal atrophy was moderate, although the intraobserver was good to excellent in the experienced endoscopists. 32 In our study, the interobserver agreement might be moderate. Further studies are warranted to clarify the factors for gastric mucosal atrophy.
In conclusion, we found that a first-degree family history of gastric cancer, absence of duodenal ulcers, and old age were the independent risk factors for gastric atrophy among H. pylori-infected patients. Careful examination with upper gastrointestinal endoscopy is necessary in patients with these risk factors.
Footnotes
Acknowledgments
We appreciate the expertise of Shuhei Matsumoto and Yoshihiro Isomura for their endoscopic procedures.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.