
Abstract
Tumor lysis syndrome (TLS) is a severe metabolic complication that usually occurs in patients with aggressive tumors who undergo treatment with chemotherapy. Traditionally, it was mainly associated with hematologic malignancies. However, over the past 4 decades, there have been increasing reports of TLS in solid tumors. We report a case of TLS in a patient with gastric cancer, as a complication of FOLFOX (5-fluorouracil, leucovorin, and oxaliplatin) chemotherapy. Our patient was a 48-year-old man with metastatic gastric adenocarcinoma who presented with altered mental status and slurred speech. On examination, he was confused and disoriented, but the rest of his examination, including vitals, was unremarkable. Laboratory findings on admission were significant for an elevated uric acid of 14.5 mg/dL, creatinine of 4.1 mg/dL, and phosphorus of 6.9 mg/dL. He had received his first cycle of FOLFOX chemotherapy 4 days prior to admission. The constellation of electrolyte abnormalities and the temporal relationship to chemotherapy led to the diagnosis of chemotherapy-induced TLS. He was treated with aggressive fluid repletion and rasburicase, following which the electrolyte derangements resolved, and he improved clinically. This case highlights the importance of early recognition of TLS in patients with gastric cancer. Initiation of early treatment can reduce the high morbidity and mortality associated with this oncologic emergency.
Introduction
Tumor lysis syndrome (TLS) is a fatal metabolic condition that has traditionally been described in hematologic malignancies as a complication of chemotherapy. It may also occur spontaneously in the setting of high tumor burden. It is a well-known complication of highly aggressive hematologic malignancies, such as Burkitt’s lymphoma and acute leukemia. However, over the past 4 decades, TLS has been increasingly described in solid tumors. We present a rare case of TLS in a patient with gastric adenocarcinoma as a complication of FOLFOX (5-fluorouracil, leucovorin, and oxaliplatin) chemotherapy. We also report other published cases of spontaneous and chemotherapy-induced TLS in patients with gastric adenocarcinoma.
Case Presentation
A 48-year-old gentleman with no known comorbidities presented with epigastric discomfort, early satiety, and unintentional weight loss of 18 kg in 1 year. He had a significant family history of gastric cancer in his older brother, ovarian and breast cancer in his mother, and breast cancer in his maternal grandmother. Computed tomography scan (Figure 1) revealed circumferential thickening of distal gastric body as well as thoracic, abdominal, and retroperitoneal lymphadenopathy. Esophagogastroduodenoscopy (EGD) revealed an exophytic mass. Biopsy was positive for adenocarcinoma with signet ring features (Figure 2). Positron emission tomography scan showed avidity in the supraclavicular and thoracic lymph nodes. He was diagnosed with stage IV gastric adenocarcinoma and started on FOLFOX chemotherapy.

Computed tomography scan of abdomen with contrast. (A) Circumferential thickening of distal gastric body and antrum. (B) Enlarged left para-aortic lymph node.

Gastric biopsy. Poorly differentiated gastric cancer cells (signet ring cells) on hematoxylin and eosin × 400.
Four days after receiving the first cycle of FOLFOX, the patient was brought to the hospital by his family for confusion and altered mentation. Vitals signs on presentation were within normal limits, with temperature of 36.3 °C, heart rate of 89 beats per minute, blood pressure of 129/98 mm Hg, and a pulse oximetry of l00% on room air. On physical examination, he was drowsy and disoriented to person, place, and time. Neurologic examination, limited by altered mentation, revealed spontaneous movement of all 4 extremities. Patellar and ankle reflexes were 2+, and biceps and supinator reflexes were 3+ bilaterally. Cardiopulmonary and abdominal examinations were benign.
Computed tomography scan of head was negative for intracranial bleeding. Laboratory findings (Table 1) were remarkable for elevated serum creatinine of 4.1 mg/dL, elevated phosphorus of 6.9 mg/dL, and elevated uric acid of 14.8 mg/dL. Calcium and potassium levels were within normal limits. He was admitted to the intensive care unit for uremic encephalopathy in the setting of TLS. Electroencephalography showed moderate generalized slowing, reflective of diffuse nonspecific cerebral dysfunction, without epileptiform activity.
Laboratory Results on Admission.

Boldface values represent abnormal laboratory parameters.
He was managed with aggressive hydration and one dose of rasburicase. Over the next 2 days, his mentation and neurologic examination improved, with the patient successfully demonstrating orientation to person, place, and time. His electrolyte abnormalities improved (Table 2), with serum creatinine of 1.3 mg/dL, uric acid of 1.7 mg/dL, and phosphorus of 2.2 mg/dL. He was transferred to the general medicine floor and was discharged in stable condition.
TLS Laboratory Values.

Abbreviation: TLS, tumor lysis syndrome.
Day 1 corresponds to the day of chemotherapy with 5-fluorouracil/oxaliplatin.
Day 5 corresponds to the day of admission.
Discussion
Tumor lysis syndrome is an oncologic emergency that occurs when tumor cells are lysed, either spontaneously or in response to cancer-directed therapy, and subsequently release their contents into the bloodstream. This leads to the characteristic findings of elevated uric acid, potassium, phosphorus, and decreased calcium.1,2 These electrolyte disturbances can in turn cause complications like renal failure, arrhythmias, seizures, and death from multi-organ failure. 1
Fast-growing tumors, especially high-grade lymphomas and acute leukemias, are widely known to be predisposed to TLS.1,2 However, TLS is known to occur infrequently with solid tumors. 3 We accessed medical literature for full-text articles from PubMed, Embase, and MEDLINE using the search terms (“tumor lysis syndrome” OR “tumor lysis”) AND (“gastric” OR “stomach”). Search results yielded 8 additional cases of TLS in gastric adenocarcinoma (Table 3).4-11 Of these, 4 have been spontaneous TLS4-7 and the other 4 were chemotherapy-induced.8-11 Including our patient, the mean age at presentation was 55 years. All 9 patients were male. Latency between the cycle of chemotherapy and development of TLS ranged from 3 to 7 days. All patients (including ours) with chemotherapy-induced TLS received regimens combining fluoropyrimidine therapy (capecitabine, floxuridine, 5-fluorouracil, and tegafur) with platinum-based therapy (cisplatin and oxaliplatin). TLS secondary to FOLFOX regimen has been described with colon cancer. 12 We have described the first case of TLS in gastric cancer, as a complication of FOLFOX therapy.
Reported Cases of TLS in Gastric Adenocarcinoma.
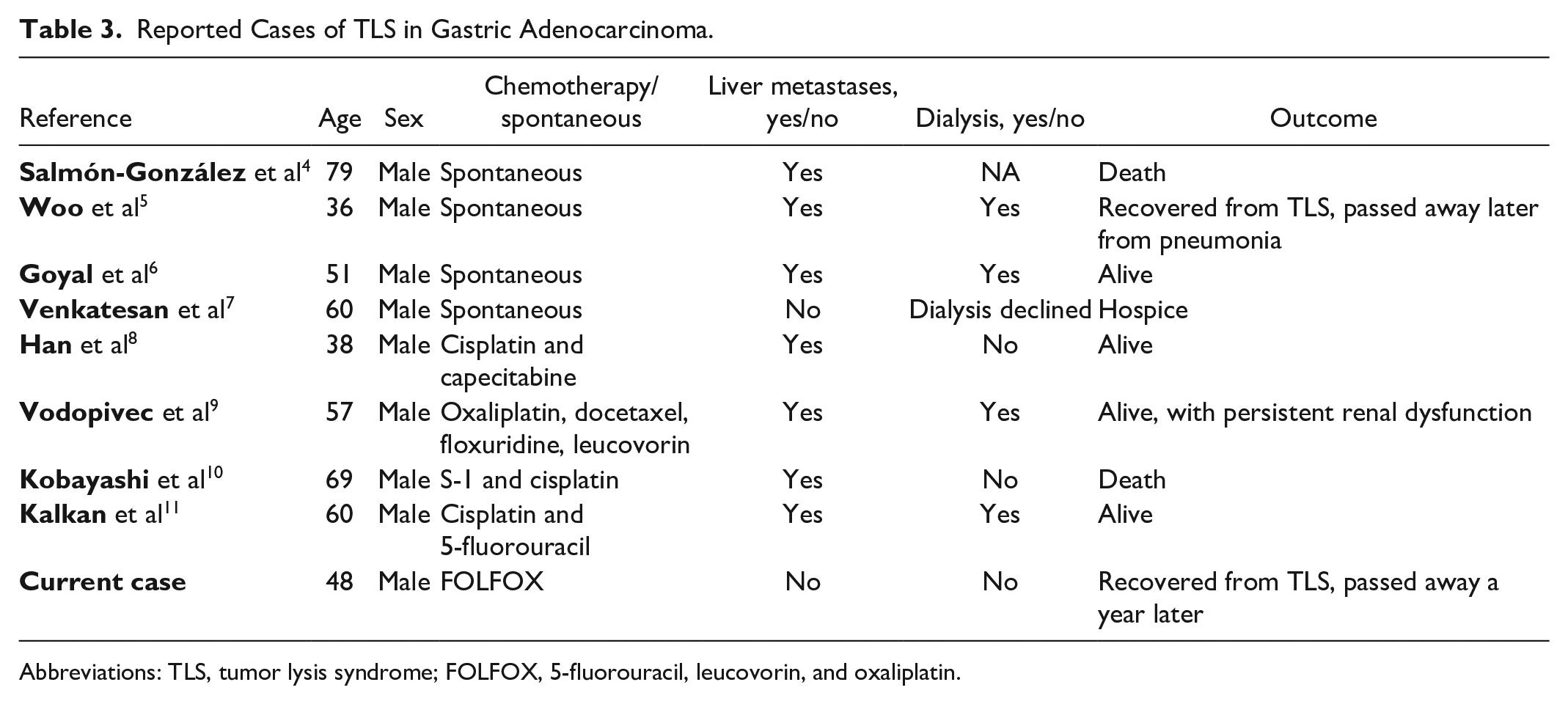
Abbreviations: TLS, tumor lysis syndrome; FOLFOX, 5-fluorouracil, leucovorin, and oxaliplatin.
Predisposing factors for TLS include patient-related factors as well as tumor-related factors. Patients with preexisting oliguria, elevated uric acid, renal insufficiency, dehydration, or acidic urine are at an increased risk for TLS. Tumor-related factors include high cell turnover rate, size, and sensitivity to chemotherapy.1,2 Hepatic metastasis is a strong risk factor for development of TLS in solid tumors and was found in 82.8% of cases in one review of solid tumors with TLS. 13 This could be due to high purine pools, high tumor load, or defective uric acid metabolism. 13 In all but one case of TLS in gastric adenocarcinoma published, the cancer was metastatic to liver. However, computed tomography scan did not show liver metastases in our patient.
The Cairo-Bishop criteria are widely used to define TLS. TLS can be classified into laboratory TLS or clinical TLS. 2 Laboratory TLS consists of a constellation of metabolic abnormalities like elevated uric acid, serum potassium, and phosphorus with decreased serum calcium levels. Two of the 4 criteria must be met to diagnose laboratory TLS. When clinical complications, such as renal insufficiency, seizures, and cardiac arrhythmias, are seen in patients with laboratory TLS, the syndrome is referred to as clinical TLS. 2 Our patient fulfilled 2 criteria for laboratory TLS and 1 criterion for clinical TLS.
Mainstay of management of TLS is aggressive hydration with intravenous fluids, with the aim of improving renal perfusion and preventing the precipitation of uric acid crystals.1,2 Uric acid levels can be reduced with the use of allopurinol or rasburicase. Efficacy of allopurinol is limited, as it does not catabolize the preexisting uric acid. Moreover, it converts uric acid to xanthine, and accumulation of xanthine may result in xanthine nephropathy. Rasburicase is superior to allopurinol as it directly breaks down uric acid and prevents xanthine accumulation. Compared with allopurinol, it has been shown to reduce the need for dialysis. 1 Rasburicase may lead to hemolysis in patients with G6PD (glucose-6-phosphate dehydrogenase) deficiency. 3 Complications from TLS, such as hyperkalemia, hypocalcemia, hyperphosphatemia, and cardiac dysrhythmias, should be treated. Dialysis may be required for severe renal dysfunction in some cases. In our literature review, 5 out of 6 cases, where the clinical course was described in detail, required dialysis.
TLS-associated mortality rate is higher in patients with solid tumors (around 35%) when compared with those with hematologic malignancies. This is likely due to protective measures being executed more often in hematological malignancies than in solid tumors. 14 ln our literature review, 2 patients died from complications of TLS, and another patient deteriorated and opted for hospice care.
Our case also demonstrates the importance of early identification of TLS in the appropriate clinical setting. Electrolyte abnormalities like hyperphosphatemia and hyperuricemia may also be seen in patients with acute kidney injury, in which case, the creatinine would also be high. However, having a high index of suspicion for TLS and timely administration of rasburicase can be potentially lifesaving.
Conclusion
Tumor lysis syndrome is an oncologic emergency that may be underrecognized and underreported with solid tumors. Patients with preexisting renal impairment or with high tumor burden are at greater risk. TLS must be kept in mind when patients present with altered mentation or with deranged electrolytes and renal impairment, especially, after recently receiving chemotherapy. Given reported higher mortality with solid tumors, early recognition of this syndrome, timely initiation of rasburicase, aggressive hydration, and appropriate management of complications can reduce the high morbidity and mortality associated with this condition.
Footnotes
Authors’ Note
This case has been presented in abstract form at the American College of Gastroenterology 2019 Annual Meeting on October 27, 2019, in San Antonio, Texas.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases.
Informed Consent
Informed consent was not obtained because the patient passed away, and we were not able to reach the family.