
Abstract
A 78-year-old male, originally from China, was brought to the hospital for weakness, urinary incontinence, confusion, and poor oral intake. He was started on empiric antibiotics, which were narrowed when blood cultures produced gram-negative bacteremia speciating to Klebsiella pneumoniae, sensitive to ceftriaxone. Computed tomography scan of the abdomen and pelvis demonstrated a large cystic region with air-fluid level in the left lobe of the liver. Suspecting this to be the source of the patient’s bacteremia, the lesion was percutaneously drained and the fluid cultured, which also revealed ceftriaxone-sensitive Klebsiella pneumoniae. While a stool ova and parasite examination on the patient was negative, further workup was positive for Entamoeba histolytica antibody in the serum, detected via enzyme-linked immunosorbent assay and indicative of either current or past infection. This suggested possible prolonged subclinical infection with bacterial superinfection, especially given that Klebsiella pneumoniae is one of the most common organisms cultured from these abscesses. In patients with liver abscesses who immigrated from developing and/or endemic regions or have a relevant recent travel history, an underlying amoebic etiology of an abscess should be considered.
Case
A 78-year-old male, originally from China, with a past medical history of hypertension, diabetes, paroxysmal atrial fibrillation, and a stroke with residual left-sided deficit and waxing and waning mental status was brought to the hospital for weakness, urinary incontinence, confusion, and poor oral intake. On the day of his presentation, the patient was noted to appear weak on the left side more so than at baseline. The patient was brought to the emergency department as a stroke code; computed tomography (CT) scan of the head ruled out acute stroke. Vital signs were significant for a heart rate of 94 beats per minute and respiratory rate of 31 breaths per minute. The patient was admitted to the hospital for sepsis and workup for possible toxic, metabolic, or infectious insults leading to recrudescence.
The patient was started on empiric antibiotics, which were narrowed when blood cultures revealed gram-negative bacteremia speciating to Klebsiella pneumoniae, ampicillin-resistant, but sensitive to ceftriaxone. A CT scan of the abdomen and pelvis demonstrated the presence of a large cystic region with air-fluid level in the left lobe of the liver (Figures 1 and 2). Under the suspicion that this lesion was the source of the patient’s bacteremia, the patient underwent percutaneous drainage of the lesion by Interventional Radiology, which produced 80 cc of purulent fluid, also growing ampicillin-resistant, ceftriaxone-sensitive Klebsiella pneumoniae. While a stool ova and parasite examination on the patient was negative, further workup revealed that the patient was positive for Entamoeba histolytica antibody in the serum, detected via enzyme-linked immunosorbent assay and indicative of either current or prior infection. The patient had lived in the United States for several years, had no recent travel history and, to the knowledge of his family, had never been diagnosed or treated for E histolytica infection in the past; as such, he was started on metronidazole and paromomycin for extraluminal amoebic infection after completing the course of ceftriaxone to treat what appeared to have been a superimposed bacterial infection of a previously subclinical amoebic liver abscess (ALA).
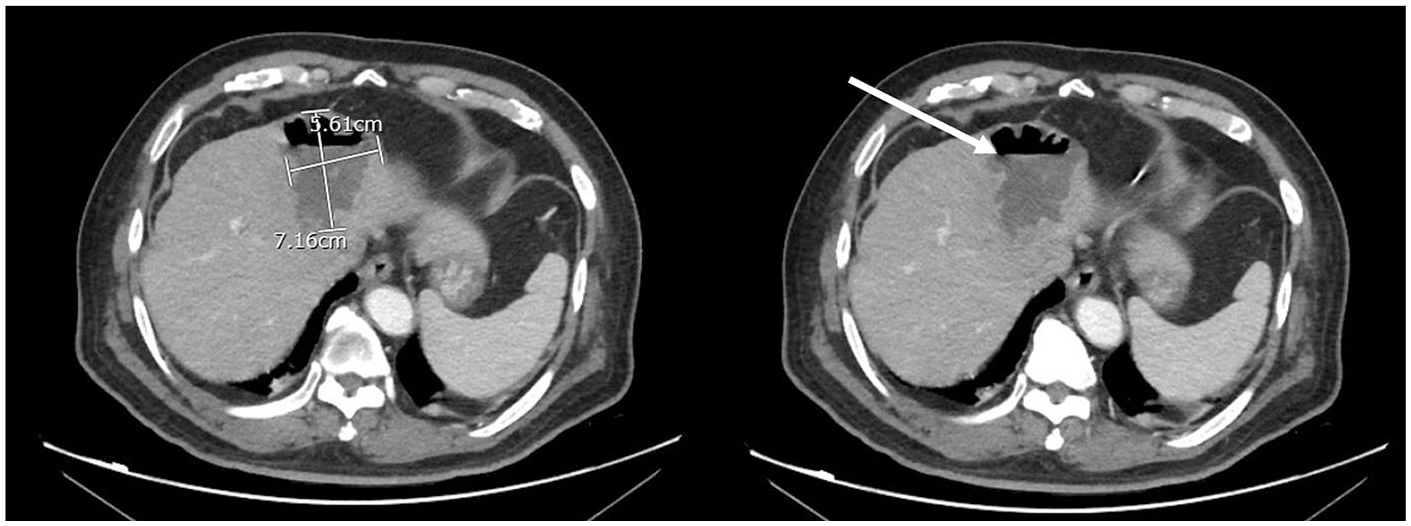
Sequential axial computed tomography images, from rostral to caudal, taken of the patient lying supine, demonstrate a 5.61 × 7.16 cm liver abscess with air-fluid level (arrow).

Sequential coronal computed tomography images, from anterior to posterior, taken of the patient lying supine, demonstrate the liver abscess with air (arrow) visualized rising to the top of the abscess in the anterior-most slices.
Discussion
Entamoeba histolytica infection is uncommon in the developed world; in endemic regions in the developing world, it can be contracted via consumption of fecally contaminated water or food containing mature cysts. 1 In the small intestine, the parasite releases trophozoites that penetrate the mucosa of the colon causing flask-shaped ulcers (intestinal disease). These trophozoites can infect the liver, brain, lungs, pericardium, and other sites by gaining access to portal venous system (extraintestinal disease). In asymptomatic carriers, cysts are passed in stool and trophozoites remain confined to the intestinal lumen (noninvasive infection). The inflammatory reaction in the liver caused by the amoebae can necrotize the hepatocytes, thereby producing an abscess. 1 This occurs in 3% to 9% of people who become infected with Entamoeba. 2
India, Africa, Mexico, and Central and South America have high rates of amoebic infection; it is also seen in the Middle East and Asia. It most commonly affects men between the ages of 18 and 50 years. 3 The most common extraintestinal manifestation of amoebiasis is ALA. The classic presentation of ALA (seen in ~80% of patients) includes fever and right upper quadrant pain within 2 to 4 weeks of exposure and infection, with ~35% of patients developing gastrointestinal symptoms. Unlike intestinal infection, patients can present with ALA months to years after travel to an endemic area, therefore making it imperative to obtain a thorough travel history. 3 E histolytica may be difficult to diagnose due to lack of history of intestinal disease within 1 year and inability to differentiate between amoebic and pyogenic abscesses on CT or magnetic resonance imaging. 4 Methods of diagnosis are outlined in Table 1. Although, historically, serologic analyses reportedly lacked sensitivity,5,6 more recent studies report high diagnostic sensitivity (>94%) and specificity (>95%). 7

Abbreviations: ALA, amoebic liver abscess; PCR, polymerase chain reaction; US, ultrasound; CT, computed tomography; MR, magnetic resonance.
As in our patient, E histolytica infection can remain subclinical. A study by Blessman et al noted that >50% of ALA residues were identified by ultrasound in subjects with no previous ALA history. 8 Their sonographic appearances were virtually identical from those found in individuals with a known ALA history. All subjects were free of clinical symptoms, confirming the existence of subclinical ALA. 8
One of the most serious complications of ALA is secondary bacterial infection, which occurs in ~20% of cases. 9 A study by Tayal et al showed that multiple ALA are not uncommon and can be super-infected or co-infected with pyogenic organisms. 10 Gram-negative rods like Escherichia coli and Klebsiella pneumoniae are the most common organisms cultured from these abscesses 11 ; as such, an underlying amoebic etiology must be considered in these cases, especially if the patient is an immigrant from or has a recent history of travel to an endemic area.
Pyogenic liver abscess (PLA) tends to occur in patients with certain underlying risk factors including diabetes, underlying hepatobiliary or pancreatic disease, liver transplant history, or chronic use of a proton pump inhibitor. 12 It is also more common in hospitalized patients, with one review showing an incidence of 8 to 22 cases per 100 000 hospitalized patients. 13 PLA accounts for 48% of all visceral abscesses in the United States. 14 It is possible that our patient’s abscess was a primary PLA and the positive E histolytica serology was merely a coincidence; however, given his status as an immigrant, no known history of Entamoeba diagnosis or treatment, and positive serology, bacterial superinfection of a clinically silent ALA cannot be ruled out, and, as such, the appropriate treatment was administered.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Institutional review board approval is not required for case reports at our institution.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because our institution does not require informed consent for individual case reports.