
Abstract
Invasive Klebsiella pneumoniae infection and pyogenic liver abscess in patients with underlying diabetes mellitus has been well described over the past 3 decades, predominantly in the Southeast Asian population, especially in Taiwan and Korea. K pneumoniae has now become the most common causative pathogen of pyogenic liver abscess in Asian countries. This shift from Escherichia coli to K pneumoniae may also be increasingly occurring in the United States of America and European countries. Compared with the >80% incidence described in Taiwan, the incidence in the United States is still reported to be lower, around 30% to 40%. However, as more evidence and reports come to light, it has become of prime importance to recognize Klebsiella as a significant emerging cause of metastatic infections in patients with uncontrolled diabetes in the United States and not just Southeast Asia, given the significant morbidity and mortality associated with the condition. In this article, we discuss the case of a 53-year-old African American female who presented with diabetic ketoacidosis and was subsequently found to have K pneumoniae pyogenic liver abscess primarily in the left hepatic lobe, bacteremia, and septic metastases to the spleen. She required extensive percutaneous drainage of abscesses and a prolonged course of multiple antibiotics. This case illustrates the growing incidence of invasive K pneumoniae infection in the diabetic population in the United States, and better patient outcomes from prompt recognition and treatment.
Introduction
Invasive Klebsiella pneumoniae infection has been reported with increasing frequency in East Asian countries in the past 3 decades. 1 Diabetes is a well-known risk factor for invasive K pneumoniae infection, which commonly results in pyogenic liver abscess (PLA).1,2 PLA is often complicated by bacteremia, sepsis, and metastatic infection to various organs. 1 Numerous extrahepatic complications of PLA have been reported in the literature, including meningitis, epidural abscess formation, necrotizing fasciitis, septic arthritis, and septic pulmonary embolism.3-5
Few cases of metastatic septic infection from PLA, resulting in multiple splenic abscesses have been reported worldwide. We present an unusual case of splenic abscesses secondary to K pneumoniae pyogenic liver abscess (KPLA) in an African American patient presenting with diabetic ketoacidosis (DKA).
Case Presentation
The patient is a 53-year-old African American female with a past medical history of hypertension and diabetes mellitus type 2 who presented to the emergency department with altered mental status. Her family reported that she had been feeling unwell for 3 days. Her symptoms subsequently progressed to altered mentation and dyspnea. In the emergency department, initial vital signs include a temperature of 36.6 °C, heart rate of 112 beats per minute, blood pressure of 140/72 mm Hg, respiratory rate of 28 breaths per minute, and oxygen saturation of 96% on room air. On physical examination, the patient was confused and agitated. She was tachypneic and tachycardic on heart and lung examination. Laboratory tests (Table 1) revealed leukocytosis with a white blood cell count of 19.9 × 109/L, absolute neutrophils of 89.3%, and a platelet count of 507 × 109/L. The basic metabolic panel revealed a sodium level of 131 mmol/L, potassium of 6.2 mmol/L, chloride of 104 mmol/L, total CO2 of 6, glucose level >38.8 mmol/L, BUN (blood urea nitrogen) of 25 mmol/L, creatinine of 362.5 µmol/L, high anion gap of 28, and acetone was large. Arterial blood gas revealed a high anion gap metabolic acidosis with compensatory respiratory alkalosis. Computed tomography (CT) of the head without contrast was unremarkable. The patient was started on intravenous fluids and insulin infusion and was transferred to the intensive care unit to manage DKA and acute kidney injury.
Illustrates the Trend of Laboratory Values Over the Course of Hospitalization.
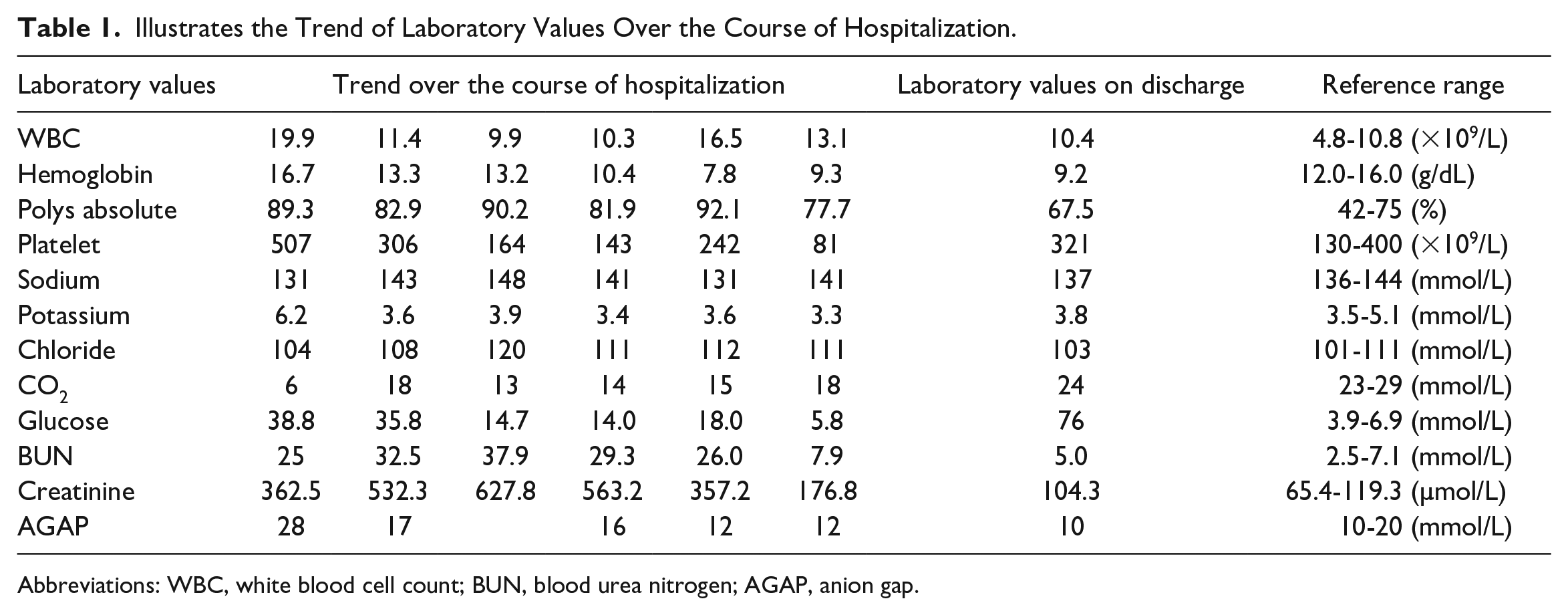
Abbreviations: WBC, white blood cell count; BUN, blood urea nitrogen; AGAP, anion gap.
In the intensive care unit, the patient’s DKA resolved, and altered mentation improved significantly over 3 days; however, her renal function progressively worsened. Her BUN and serum creatinine continued to trend up, and she became oliguric. Given these changes, an Udall catheter was placed for hemodialysis. Of note, the patient had a creatinine level of 88 µmol/L and BUN of 3.6 mmol/L on her outpatient blood work 2 months before this presentation.
In the days following treatment, the patient became febrile, with a Tmax of 39.1 °C and tachycardic, but she remained hemodynamically stable. A septic workup was performed, and empiric broad-spectrum antibiotics were started along with antipyretics. Blood cultures grew K pneumoniae. Ultimately, a CT scan of the abdomen and pelvis with oral contrast showed several hypoattenuating hepatic lesions and heterogeneous splenic hyperattenuation concerning for splenic infarcts. Magnetic resonance imaging of the abdomen and pelvis to further characterize these lesions revealed about 8 lesions in the left hepatic lobe, with the largest lesion measuring 3.9 × 3.2 × 3.7 cm in size, within segment 3 of the left hepatic lobe concerning for hepatic abscess. There were also numerous ill-defined peripherally located lesions within the spleen concerning for abscesses. Piperacillin/tazobactam was de-escalated to ceftriaxone along with metronidazole. Percutaneous drainage of the left hepatic lobe abscess through Interventional Radiology guidance yielded 30 mL of pus that grew K pneumoniae as well (see Figures 1 and 2).

Magnetic resonance imaging showing abscess in the liver and spleen.

Computed tomography scan of the liver abscess.
The patient’s overall condition improved, and repeat blood cultures were negative. Her renal function stabilized, and dialysis was discontinued. A repeat CT scan of the abdomen and pelvis revealed worsening of several ill-defined hypoattenuating splenic lesions with adjacent perisplenic fluid, which required percutaneous drainage of the splenic abscesses.
Likewise, her hospital course was complicated by acute right femoral, popliteal, and peroneal vein deep vein thrombosis, for which she was started on high-range heparin infusion, which was discontinued after 2 days due to a steep decline in hemoglobin level. An inferior vena cava filter was subsequently inserted. A colonoscopy revealed a 15-mm polyp in the cecum and nonbleeding hemorrhoids. Her hemoglobin level subsequently stabilized following blood transfusions. She continued to improve clinically on the current antibiotic regimen. Ultimately, she was discharged to complete a 6-week course of antibiotics through a peripherally inserted central catheter line to follow-up outpatient with nephrology, infectious disease, and primary care physician.
Discussion
Invasive K pneumoniae infection commonly results in PLA. PLA is a rare but serious and life-threatening infection that leads to bacteremia, septic shock, liver, and kidney failure, and in extreme cases, it can lead to end-organ failure. 6 It is characterized as a space-occupying lesion in the liver, for which bacteria is the causal organism. 7 The incidence of PLA is low, however, growing, and current data suggest an incidence rate of 3.59 cases per 100 000 population per year in the United States.7,8
PLA is a polymicrobial infection and is generally caused by Escherichia coli, streptococci, Enterobacteriaceae, and anaerobic organisms.6,7,9 However, recent studies show K pneumoniae, particularly serotypes K1 and K2, as a cause of PLA and is predominantly seen in Taiwan, China, and the Far East.6,7
Historically, the etiology of PLA was attributed to trauma and intraabdominal infections, in particular, appendicitis. Recently, the etiology has shifted to pathological conditions related to the biliary tract. 10 Some of the most common etiological factors associated with PLA include biliary tract infections, biliary tract obstruction with cholangitis, portal bacteremia, direct invasion from cholecystitis or contiguous sites of infection, or perinephric abscess, or systemic bacteremia, and pyelonephritis.7,9 Despite these facts, in more than 55% of the cases, a direct predisposing risk factor cannot be identified and is considered “cryptogenic.”10-12
In addition to biliary pathologies, diabetes is a known risk factor for PLA.6,13 In an observational study by Wang et al, 145 out of 178 patients diagnosed with a liver abscess had diabetes mellitus. 14 Wang et al concluded that patients with diabetes mellitus are more susceptible to acquiring bacterial liver abscess. 14 Additionally, patients with a history of gallstones increases the higher risk of PLA diabetes patients. 15
These patients with diabetes are more likely to suffer from complications secondary to PLA and may experience prolonged fevers and longer hospitalizations.6,16 Other documented reports noted diabetes as a significant risk factor for Klebsiella liver abscess in Asia, with diabetes being observed in up to 75% of patients. However, the incidence of diabetes in patients with KPLA was lower in the studies seen in the United States. 17
Not only is diabetes recognized as a significant risk factor for KPLA, but it is also associated with increased septicemic complications.6,7 The most common septicemic complications include brain abscess, septic pulmonary embolism, and endophthalmitis. 18 Patients with K pneumoniae splenic abscess have a significantly increased prevalence of underlying diabetes mellitus compared with those of non-Klebsiella splenic abscess. 19 Uncontrolled diabetes and poor glycemic management impairs the immune system and alter the neutrophil phagocytosis process, resulting in the growth of the pathogen within the tissues. 19
Consequently, the blood sugar level should be closely regulated and controlled to prevent serious and life-threatening complications.6,20 Uncontrolled diabetes mellitus in our patient was a key risk factor in the initial infection and abscess development.
The clinical symptoms and presentation of pyogenic abscess can be nonspecific including abdominal pain, fever, nausea, and vomiting, fullness, and jaundice. Thus, early recognition and diagnosis are particularly important due to the vague clinical presentation and to allow recovery without long-term complications and sequelae. 10 Culture and radiological findings are the mainstay of diagnosis in PLA.6,7 Some of the imaging modalities include ultrasound and CT with intravenous contrast. Diagnostic features on CT that are suggestive of Klebsiella liver abscess include solitary abscess often more than 5 cm, involving 1 lobe most commonly the right lobe with either solid or multiloculated appearance. 6 Uniquely, our patient had multiple hepatic lesions.
Third-generation cephalosporins are commonly used,6,7 others suggest the use of metronidazole to cover for anaerobic or amoebic infections. Further adjustments can be made based on the cultures and sensitivities to aid in the choice of antibiotics. While the duration of antibiotics is not completely clear, a regimen of 6 to 8 weeks is commonly used. 7 In select cases that fail antibiotic therapy or in larger abscesses, a pigtail catheter draining of the abscess aids in the management.6,7 Proper recognition of liver abscess is crucial to reduce further complications such as life-threatening metastatic endophthalmitis 21 or central nervous system infections.22,23
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.