
Abstract
Ketogenic diet or very-low-carbohydrate diet gained widespread popularity in the 1990s due to their favorable effects on weight loss and diabetes among others with good short-term safety data. People on ketogenic diets exist in a state of “dietary ketosis” in which the body production of ketone is equal to consumption and no harmful effects of ketonemia occur. However, in face of stress, the harmless “dietary ketosis” can lead to profound acid-base disturbances due to massive overproduction of ketone bodies that overwhelms the acid buffer system of the body. A handful of case reports have been published on this topic calling the safety of ketogenic diet into question. In this article, we chronicle a unique case of ketogenic (Atkins) diet–associated ketoacidosis, and we present a comprehensive literature review on the etiology of ketoacidosis.
Keywords
Introduction
Ketone bodies are formed by the deamination of amino acids and degradation of fatty acids in times of severe stress, diabetes, alcoholism, starvation, and pregnancy. 1 Rarely, a low-carbohydrate ketogenic diet can also give rise to ketoacidosis. 2 We present a case of a young nonpregnant female with no history of alcoholism, diabetes, or starvation presenting with dialysis-refractory metabolic acidosis due to Atkins diet–associated ketoacidosis. Urgent intubation, intensive care, and aggressive fluid resuscitation with insulin therapy led to the successful recovery of the patient. We also performed an extensive literature search and highlighted all reported literature of nondiabetic ketoacidosis (NDKA).
Case Presentation
A 33-year-old Caucasian female was brought to the emergency department with possible syncope following lethargy and extreme exhaustion. Her mother found her on the floor of the restroom after hearing her falling down. According to her parents, she had mild flu-like symptoms, low-grade fever, and multiple episodes of nonbilious vomiting for 3 days before presentation. Her parents denied her ingestion of any medications or toxic substances intentionally or accidentally, and she did not have a past history of suicide attempts or ideation. Past medical history was only significant for high-functioning autism; she worked as a cashier at a fast food restaurant and was living with her parents. Her medications included methylphenidate and sertraline for years without any recent changes.
On presentation, her vitals included temperature 98.2°F, blood pressure 140/71 mm Hg, heart rate 136 beats per minute, respiratory rate 38/min, and oxygen saturation of 96% on ambient air. Examination revealed a Glasgow Coma Scale score of 10/15; mucous membranes were dry, and skin was cold to touch with decreased turgor. Breathing was deep and labored, chest was otherwise clear to auscultation; gastrointestinal and cardiovascular examinations were unremarkable.
Investigations
The laboratory values are shown in Table 1.
Laboratory Studies of Our Patient While She Was in the Intensive Care Unit.

Abbreviations: AST, aspartate aminotransferase; ALT, alanine aminotransferase; ALP, alkaline phosphatase; HbA1c, hemoglobin A1c; pCO2, partial pressure of carbon dioxide; pO2, partial pressure of oxygen; HCO3, bicarbonate; SaO2, oxygen saturation.
Serum and urine toxicology was negative for alcohol, salicylate, acetaminophen, and other toxic alcohols. Urine pregnancy test was negative; however, urinalysis was positive for ketones (+4). Computed tomography scan of head and chest X-ray were unremarkable.
Differential Diagnosis
Initial suspicion of the cerebrovascular accident was ruled out by the normal computed tomography scan of the head. Sepsis, diabetic ketoacidosis, poisoning with toxic alcohols, and pregnancy-induced ketosis were considered, but they were ruled out with the appropriate studies.
Treatment
She was initially stabilized with aggressive volume resuscitation, sodium bicarbonate therapy, and ventilator support. Broad-spectrum antibiotics (vancomycin and piperacillin/ticarcillin) were started due to the possibility of sepsis from unknown origin. Persistent metabolic acidosis in spite of bicarbonate therapy led to one session of hemodialysis that improved serum bicarbonate levels to 16 mEq/L from 2.5 mmol/L. After a few hours of hemodialysis, repeat laboratory tests showed worsening acidosis with serum bicarbonate dipping down to 12 mmol/L. At this point, endocrinology was consulted and serum was tested for possible ketonemia, which turned out to have β-hydroxybutyrate (β-hB) levels of 120.1 mg/dL (normally less than 3 mg/dL). On further questioning, her parents mentioned that she was on a “weight-loss diet” for about 2 months. Suspecting the diagnosis of ketogenic diet–induced ketoacidosis, she was started on intravenous (IV) insulin along with dextrose 10%.
Outcome and Follow-up
She improved rapidly after the start of IV insulin and dextrose infusions. Metabolic acidosis and anion gap (AG) resolved within a day and β-hB levels normalized. She was then extubated and shifted to a general medicine floor on the second day of her presentation. On further questioning, she admitted to following a strict commercially available ketogenic diet (Atkins diet) for the past 2 months. She was discharged home in a stable condition on day 5 of hospitalization with the diagnosis of the ketogenic diet (Atkins diet)–induced euglycemic metabolic ketoacidosis. A follow-up after 3 months revealed that she was doing well and was not following the Atkins diet anymore.
Discussion
Over the past century, numerous different diets have been studied and tried to help weight loss. The 2 basic diets popularized are the low-fat and the low-carbohydrate diet (LCD). The LCD has increased popularity in the latter part of the past century, especially after the introduction of Atkins diet by R. C. Atkins in 1972. 3 Atkins diet is a special type of LCD, which is protein rich and has high-fat contents. The beneficial effect of LCD in an Atkins regime is believed to be due to the use of higher energy ketones rather than glucose for the production of energy. Even though studies have shown that LCD is effective for weight loss and causes improvement in cardiovascular risk factors, there are still controversies surrounding the use of this diet, one of the most serious of which is NDKA. 4
NDKA is the presence of ketoacidosis in the absence of diabetes and is typically associated with starvation, alcoholism, hyperthyroidism, and lactation. However, this can also occur rarely with LCD, especially in patients with comorbid conditions and intercurrent illness. Our case is unique in the sense that it occurred in an otherwise healthy young female with no significant comorbidities.
There are a few mechanisms by which an LCD induces ketosis. Normally in high-carbohydrate states, aerobic glycolysis produces citrate as one of the intermediate metabolites. This citrate is a signal for a high-glucose state and inhibits the activity of carnitine palmitoyltransferase complex-1 (CPT-1). 2 CPT-1 complex is responsible for the β-oxidation of fatty acids, and its inhibition prevents the metabolism of fatty acids and the production of ketones in carbohydrate-rich states. The opposite occurs in low-carbohydrate states. With no citrate, the CPT-1 is activated and extensive β-oxidation of fatty acids occurs. The liver then uses this energy to make ketone bodies, which provide energy to important organs, including the brain, heart, and kidneys. 2 Moreover, fat-rich diet and LCD can enhance glucagon secretion and lower insulin secretion, and a high glucagon-to-insulin ratio also promotes ketosis.5,6 Excessive accumulation of ketone bodies in the body occurs when its production is greater than consumption, leading to ketoacidosis. We believe that the low-carbohydrate and high-plasma fatty acid concentrations, compounded by the absence of carbohydrate-induced inhibition of β-oxidation of fatty acids might be the cause of NDKA in patients on an Atkins diet. The pathophysiology of LCD or Atkins diet-induced ketoacidosis is shown in Figure 1.

Flow sheet of the pathophysiology of nondiabetic ketoacidosis.
A comprehensive literature search using the MEDLINE databases (PubMed and Ovid) showed only a handful of cases on ketoacidosis in nondiabetic patients. Different Medical Subject Headings (MeSH) like “non-diabetic,” “euglycemic,” “normoglycemic,” “normal sugar levels,” “ketoacidosis,” “ketonuria,” “ketonemia,” “ketosis,” “metabolic acidosis,” “fatty acids,” “metabolites,” “acetoacetate,” and “beta-hydroxybutyrate” were combined using Boolean operators. A total of 127 cases were initially obtained; after removing 36 duplicate studies, 93 studies were read in full-text form. Twenty-seven out of 93 cases were found relevant to our study, but only 22 cases had sufficient data for extraction.2,5-25
Further stratification of the selected cases showed that NDKA was most commonly reported in chronic alcoholics (5 case reports including 9 patients) and LCD users (5 cases).2,6,7,9,11,1721 Only 3 cases were reported in pregnancy and lactation each.12,13,15 It is interesting to note that the pregnant and lactating patients had overriding starvation or low-carbohydrate intake as precipitating factors for ketoacidosis. There was only a single case of euglycemic ketoacidosis reported with diets like Dukan diet, diet coke, and fruitarian diet each and a single case each with hyperthyroidism, bariatric surgery, and salicylate use 22 24 (Figure 2). Most of these patients had an underlying condition like pregnancy, asthma, pneumonia, or hyperthyroidism, which might have made them vulnerable to develop ketoacidosis. Our patient is unique as she was a previously healthy individual who presented as syncope mimicking cerebrovascular accident. The underlying cause was the Atkins diet, which has never been reported before as the cause of severe NDKA.
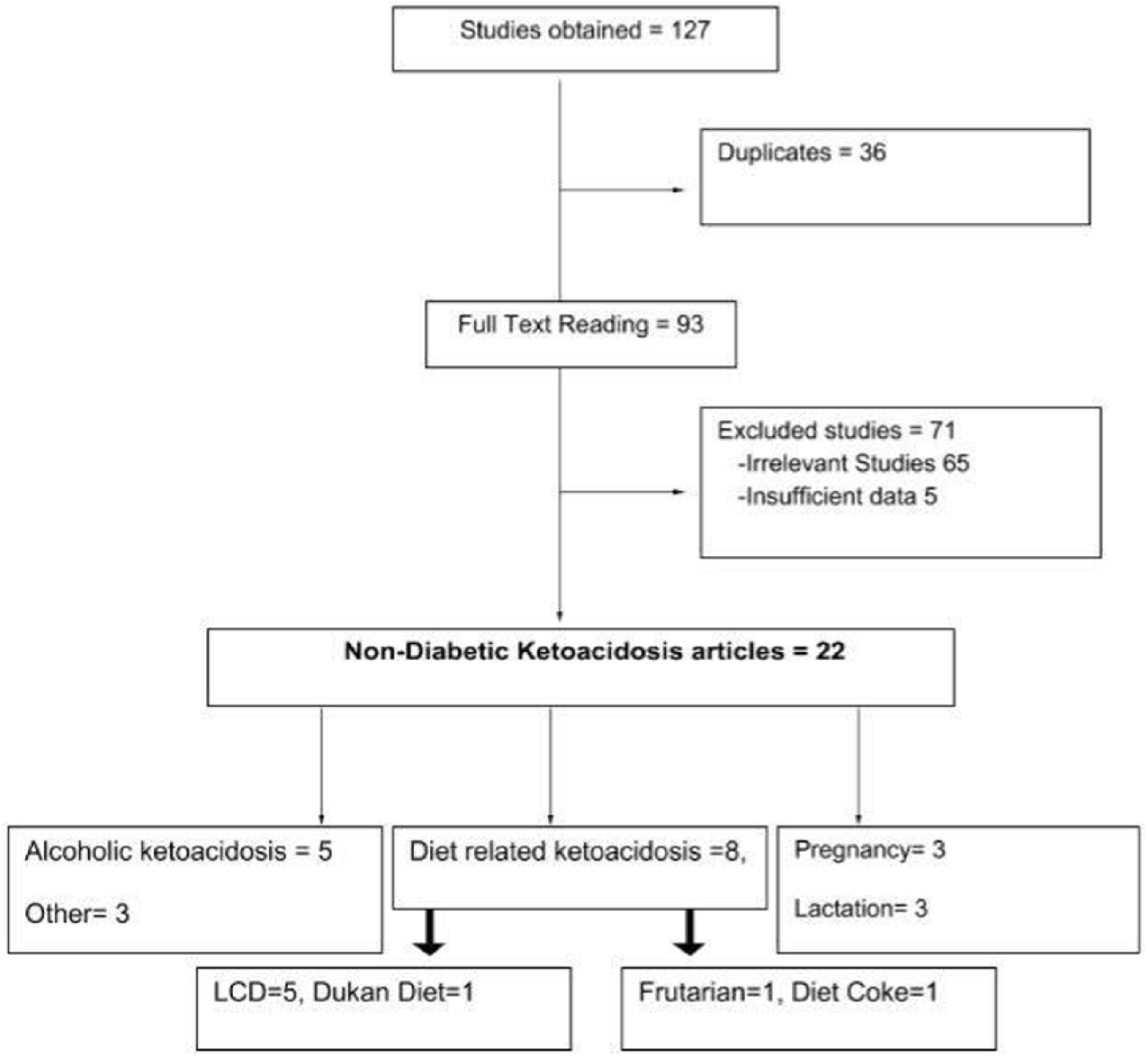
Flow sheet of studies on nondiabetic ketoacidosis.
NDKA was most commonly reported in female patients (n = 16) when compared with male patients (n = 11). The age distribution ranged from 5 to 79 years. More than 80% of the patients were at the extreme of ages and with other comorbid conditions signifying that stressful or lower metabolic reserve makes patients susceptible to NDKA. Our patient, however, was unique that flu was the only association, and she was relatively younger than the majority of reported patients. Most patients presented with gastrointestinal symptoms like nausea, vomiting, and diarrhea (n = 13) or mild central symptoms like a headache, dizziness, and confusion (n = 5). Cardiovascular symptoms like palpitations (n = 3) were also noted in a few cases; our patient surprisingly presented with syncope with a low Glasgow Coma Scale score of 10/15 and respiratory failure. Almost all patients were normotensive and were maintaining oxygen saturation at room air. All of them were found to have positive urinary ketones or serum ketonemia in association with high AG metabolic acidosis in the absence of hyperglycemia and a history of diabetes. This was confirmed by arterial blood gases, serum and urinary ketones, and an HbA1c. The β-hB was the most commonly used tested ketone body with a value ranging from 80 till 9000 µmol/L in the previously reported cases; in our case, the value was above 10 000 μmol/L. High AG metabolic acidosis in reported cases was spread between a pH of 6.8 to 7.2, HCO3 2.9 to 10 mEq/L, and AG 21 to 28. In our patient, however, the pH was very low 6.6, HCO3 of 2.6, and AG 30. These findings were alarming for us and are important for readers suspecting that Atkins diet is associated with serious NDKA in terms of its presentation and laboratory findings. It also signifies that a ketogenic diet can cause severe symptoms and complications like syncope and respiratory failure even in a previously healthy young patient when they encounter a stressful condition like seasonal flu. The characteristics of previously reported cases are summarized in Table 2.
Previously Reported Cases of Nondiabetic Euglycemic Ketoacidosis a .
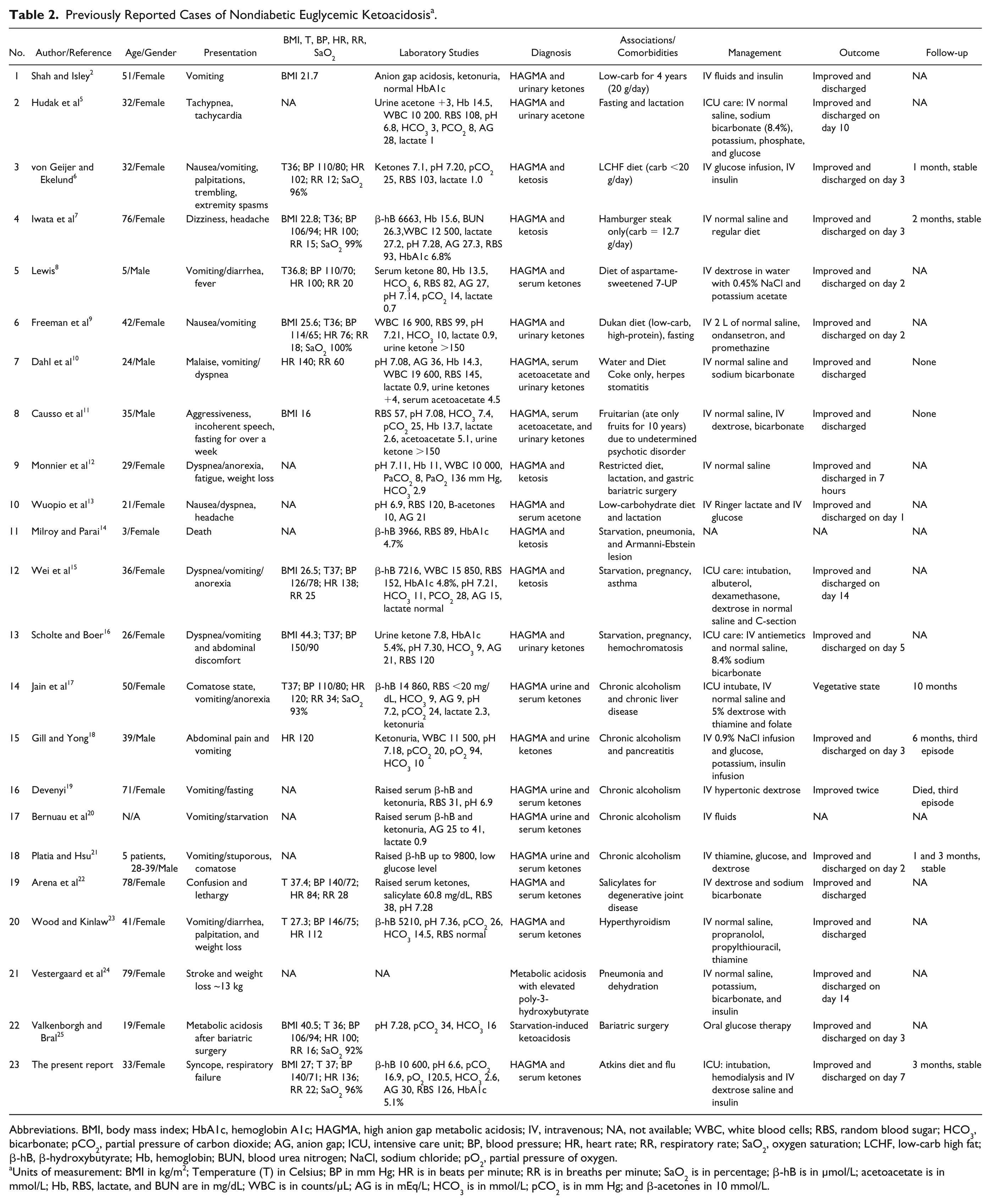
Abbreviations. BMI, body mass index; HbA1c, hemoglobin A1c; HAGMA, high anion gap metabolic acidosis; IV, intravenous; NA, not available; WBC, white blood cells; RBS, random blood sugar; HCO3, bicarbonate; pCO2, partial pressure of carbon dioxide; AG, anion gap; ICU, intensive care unit; BP, blood pressure; HR, heart rate; RR, respiratory rate; SaO2, oxygen saturation; LCHF, low-carb high fat; β-hB, β-hydroxybutyrate; Hb, hemoglobin; BUN, blood urea nitrogen; NaCl, sodium chloride; pO2, partial pressure of oxygen.
Units of measurement: BMI in kg/m2; Temperature (T) in Celsius; BP in mm Hg; HR is in beats per minute; RR is in breaths per minute; SaO2 is in percentage; β-hB is in µmol/L; acetoacetate is in mmol/L; Hb, RBS, lactate, and BUN are in mg/dL; WBC is in counts/µL; AG is in mEq/L; HCO3 is in mmol/L; pCO2 is in mm Hg; and β-acetones in 10 mmol/L.
NKDA is usually managed with IV dextrose along with insulin, IV bicarbonate, correction of electrolyte imbalances, and supportive treatment until the acidosis is resolved. Though NDKA is a serious and potentially life-threatening condition, timely diagnosis and proper management as in our case leads to good outcomes. Outcomes were not reported in all the cases; however, in cases where details were available, all the patients recovered with no significant long-term sequelae.
Conclusions
Starvation, pregnancy, lactation, and ketogenic (Atkins) diet–associated ketoacidosis can be severe and possibly fatal if not treated promptly.
Physicians should consider diet-associated ketoacidosis in previously nondiabetic patients presenting with severe metabolic acidosis.
Hemodialysis is only helpful as a temporizing measure but has no role as definitive management.
Intravenous insulin is the mainstay of treatment even in patients with normal glucose levels; however, intravenous dextrose should be given to avoid hypoglycemia.
To summarize, Atkins diet and other previously reported diets like Dukan, fruitarian, aspartame, and other low-carb high-fat diets should be considered as an extra “D” in the mnemonic “MUDPILES” for causes of high anion gap metabolic acidosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.