
Abstract
This narrative review explores the evolution of occlusal splint fabrication, focusing on the transition from traditional analog methods to modern digital workflows, incorporating scanning and 3D-printing technologies. It examines the advantages of 3D printing, including accuracy, efficiency, and patient comfort. The review also explores the materials and techniques involved in 3D-printing occlusal splints, from conventional acrylic splints and alginate impressions to more advanced computer-aided design (CAD)/computer-aided manufacturing (CAM) systems.
The available literature demonstrates that 3D printing accelerates the production of splints, offering greater customization while reducing material waste. However, challenges remain concerning the strength, biocompatibility, and durability of 3D-printed materials in the oral environment. While milled splints are known for their superior strength and longevity, 3D-printed splints provide increased flexibility and faster turnaround times, with printing orientation playing a crucial role in fit accuracy.
In conclusion, 3D printing significantly enhances the procedure for creating occlusal splints, offering notable improvements over traditional methods. Nevertheless, further research is necessary to optimize the performance of 3D-printed materials and address durability concerns to match the longevity of milled splints.
Keywords
Introduction
In the past few years, dentistry has experienced a notable increase in digitalization. Scientific advancements continue to progress, leading to the replacement of traditional, analog methods with modern 3D technologies. Three-dimensional printing, also known as additive manufacturing (AM), is an advanced manufacturing technique. It uses digital models created using computer-aided design (CAD) and common materials to create customized items through computerized processes. 1 It is currently being used by dental professionals, including dentists, dental technicians, and researchers in the field. 2
The industrial process known as AM, or 3D printing, involves adding material layer by layer to produce three-dimensional objects. In contrast, subtractive techniques involve removing material from a solid block. Both methods adhere to ISO guidelines, which comprise rules ensuring consistency, safety, quality, and efficiency. 3
In dentistry, the areas where 3D printing is primarily utilized include oral surgery, prosthodontics, and orthodontics. Some devices are interdisciplinary, such as occlusal splints. Splints work well to treat temporomandibular disorders (TMD), assist orthodontics, and serve as a preventive method. Occlusal splints are especially helpful in relieving stress, decreasing muscle contraction, and reducing the negative consequences of bruxism and TMD. 4
Splint therapy involves using removable devices to balance the masticatory system, reduce parafunctional forces, and ensure even occlusal contact without permanently altering dental occlusion or the intermaxillary relationship. 5 These splints promote harmony among muscles, joints, and related structures, making them effective in the TMD, craniomandibular disorders (CMD), and preventing tooth wear due to bruxism. 6 By disrupting habitual clenching and preventing maximum intercuspation, splints protect the teeth and surrounding tissues. 7
The analog method for making occlusal splints, involving alginate impressions, stone models, and vacuum forming or acrylic curing, is time-consuming for both technicians and clinicians. Based on the literature, the 3D printing industry effectively resolves this issue. Creating occlusal devices through an entirely digital process offers numerous advantages over traditional methods, including a reduced requirement for occlusal adjustments during delivery appointments. This reduction in modifications can lead to decreased chair time, enhancing comfort for both the patient and the dentist. 8
This review will discuss 3D-printed splints, investigating the scientific progress that has enabled the shift from conventional impressions to digital scanning and the creation of 3D-printed splints. Furthermore, the review will analyse the advantages of 3D-printed splints, the production process, and the materials involved, while also considering the potential disadvantages linked to this technology.
Evolution of the 3D Printing
The idea of 3D printing can be traced back to the 1940s when science fiction writers imagined machines that could build items layer by layer. In 1945, Murray Leinster wrote about a machine that constructs objects in midair. Advancements began in the 1970s with Johannes F. Gottwald’s metal printing invention. A major development occurred in 1986 when Charles Hull patented stereolithography (SLA), established 3D Systems, and introduced the first 3D printer, SLA-1, in 1987. 9
In the 1990s, 3D printing began to extend beyond industrial applications into the medical field, including dentistry, with notable growth in prosthodontics during the late 1990s. 10 In 2000, advances in material science and CAD/computer-aided manufacturing (CAM) technology further enhanced the capabilities of 3D printing. Ongoing research continues to focus on developing materials and techniques to improve the mechanical properties, biocompatibility, and aesthetics of 3D-printed dental splints and prostheses.9,11
Combining 3D printing technology with digital workflows facilitates the transfer of data and the transition from CAD to the production phase, reducing inaccuracies and decreasing the time required at the chairside. Clinically, this approach offers improved precision, greater patient comfort, more efficient lab procedures, and cost-effectiveness. 11
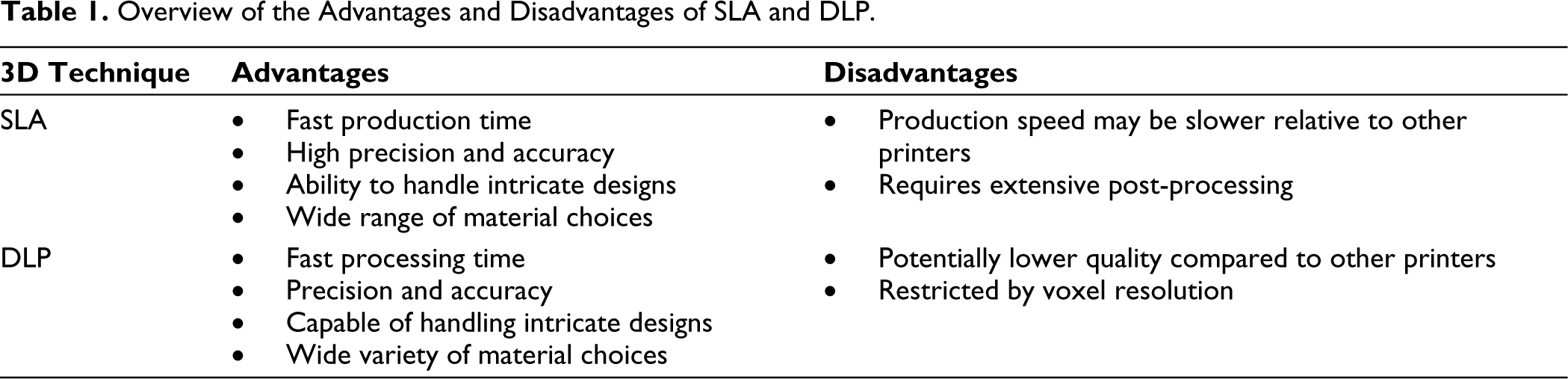
As mentioned briefly above, the first variant of 3D printing is the SLA technique; there are also digital light processing (DLP) and PolyJet technologies. SLA uses lasers to cure the liquid resin with high precision, while DLP employs a projector for faster layer-by-layer curing and PolyJet sprays and UV-cures liquid resin for multi-material and multicolor prints. These technologies, which are widely used in dental, medical, and prototyping, allow for detailed designs, speed, and diversity in 3D printing. 10
The SLA, DLP, and PolyJet 3D printing technologies have various applications in dentistry, including the creation of accurate dental models, orthodontic appliances, and custom surgical guides. Due to their high precision, SLA and DLP are often utilized to create crowns, bridges, and dental retainers, while PolyJet is best suited for multi-material prostheses and study models. Compared to analog techniques, these technologies provide faster, more personalized, and more effective solutions for fabricating numerous dental devices. 10
3D-printed Occlusal Splints
The traditional technique for occlusal splint fabrication involves the use of an elastomeric impression. Alternatively, two other methods involve the initial scanning of the dental arches, followed by either 3D printing or milling the splint.8,12
A primary advantage is the capability of 3D printing to create features with precise accuracy. The most gloss and least surface roughness before polishing can be observed when setting a 0° for manufacturing 3D-printed occlusal splints. Typically, the only post-processing steps required to ensure a comfortable fit without adjustments are washing and curing. For 45° and 90° 3D-printed occlusal splints (allowing more splints to be printed at the same time), polishing with burs and pumice is necessary.14,15 A well-polished occlusal splint enhances wear resistance. 13 Compared to traditional manual methods, the production time of 3D-printed occlusal splints is significantly reduced overall. 14 Furthermore, 3D printers can produce complex and hollow dental parts, including features like undercuts.
One major advantage is that the 3D printer greatly decreases the time needed for fabrication. It is also possible to use the 3D printer and scanner to produce the splint chairside. It can also be associated with the ability to fabricate a variety of dental appliances using a single machine. 15 Although 3D-printable dental resins may have a higher unit price, overall costs are decreased due to reduced material waste and a lower demand for specialized labor. 16
It is worth mentioning that 3D-printed splints are easy to replace if the device gets lost or damaged. Traditional manual replacement methods can be costly and time-consuming, while the digital model can be virtually stored and later reprinted when needed.
In the dental field, the two most well-known types of 3D printers are SLA and DLP (Table 1). These methods are widely used for the fabrication of occlusal splints. 16
Overview of the Advantages and Disadvantages of SLA and DLP.
In addition, several other 3D printing technologies are available in the dental field, including Fused Deposition Modeling (FDM), Selective Laser Sintering (SLS), Selective Laser Melting (SLM), Photopolymer Jetting, Powder Binder Printing, and 3D Laser Bioprinting (LAB).17,18 FDM works only with low-melting-point materials and is a slow printing method. Besides, the printed occlusal splint has a poor surface structure, and the print dimensions are limited. 19 Similar to PolyJet 3D printing, Powder Binder Printing, and LAB printing, these techniques are not yet employed for the production of 3D-printed splints, probably due to the compatibility of available materials and costs for production.20,21 The technologies MEX, FFF, and CLIP for occlusal splints are rarely utilized, with no outcomes available.
Materials Used for 3D-printed Occlusal Splints
Intraoral devices should be fabricated from materials that can alleviate the stress, with microhardness and elasticity modulus typically ranging between 250–800 MPa and 10–20 GPa, respectively. These properties help balance the rigidity of enamel by providing shock absorption, ensuring good wear resistance, and maintaining acceptable surface polishing. Adequate properties help prevent appliance alterations, such as wear, discoloration, microporosity, premature biofilm formation, and occlusal instability. 22
A previous study found that 3D-printed methacrylate-based resins (such as Freeprint and Luxaprint) showed satisfactory tensile strength (TS) (43.7–48.5 MPa), modulus of elasticity (2.01–2.37 GPa), and hardness (11.8–15.0 HV). 23 Standard mechanical property values for occlusal devices are Vickers hardness (VHN) ranging from 10 HV to 20 HV, modulus of elasticity (ME) between 1.5 GPa and 4 GPa, and TS from 30 MPa to 100 MPa. For instance, 3D-printed methacrylate-based resins have TS between 43.7–48.5 MPa, ME of 2.01–2.37 GPa, and HV of 11.8–15.0 HV2. 24 These values can vary based on the material and production method used.25,26
Another important factor to consider when fabricating splints is the patient’s specific oral habits. Splints are often recommended for patients with TMD. Since brux patients may suffer from large occlusal forces in their mouths (ranging from 450 N to 650 N, with an average of 380 N), the materials used to fabricate occlusal splints must have excellent mechanical properties. 27
PMMA (polymethyl methacrylate) remains the most widely used material to make splints, but a growing amount of research is looking for other materials that could work just as well.28,29 PMMA is highly regarded for its good chemical and physical qualities, pleasing aesthetically, and reasonable cost. However, the clinical efficacy and mechanical characteristics of occlusal splints may be adversely affected by polymerization shrinkage and the presence of leftover monomers when using an analog manufacturing method. Even under the best laboratory conditions, partial conversion of monomers to polymers is still present.30,31
According to a report, PMMA that had been conventionally cured had much rougher surfaces than the groups that had been digitally produced. 32 Research indicates that while analog splints tend to accumulate more plaque due to rougher surfaces, 3D-printed samples showed the highest adhesion of Streptococcus mutans. This discrepancy is linked to differences in surface energy and hydrophobicity, as highlighted by Ozel, who noted that PMMA’s higher surface energy improves its hydrophobicity, thereby reducing S. mutans adhesion. Additionally, leftover methyl methacrylate monomers in PMMA resins negatively affect S. mutans cell viability. 33 This also explains why PMMA is associated with allergic reactions. These reactions are also often attributed to under-processed free methyl methacrylate monomer in acrylic resins. Clinically, this manifests itself in the oral cavity as redness of the mucosa and significant sensitivity in the affected area. 34
Other studies also comparing surface roughness and microbial adhesion (specifically S. mutans) on conventional and digital splints reveal differences in how manufacturing methods influence these factors. According to one study, traditional thermoformed or pressed resins showed lower microbial adhesion to S. mutans than 3D-printed resins. These results imply that although surface characteristics such as roughness are important, other elements may also play a role in microbial development, especially in the case of fungal adhesion, which was noticeably greater on 3D-printed and milled splints than on those made using other techniques.35,36
Research on materials for the fabrication of occlusal splints is limited. Prpic et al. (2019) compared two 3D-printed materials: VarseoWax (non-acrylic) and Ortho Rigid (acrylic). They found that material choice impacts mechanical performance more than the production method (Table 2). Acrylic resin consistently shows higher surface hardness, while non-acrylic resins offer greater flexibility. 28
Overview of the Materials Used to Fabricate 3D-printed Occlusal Splints.
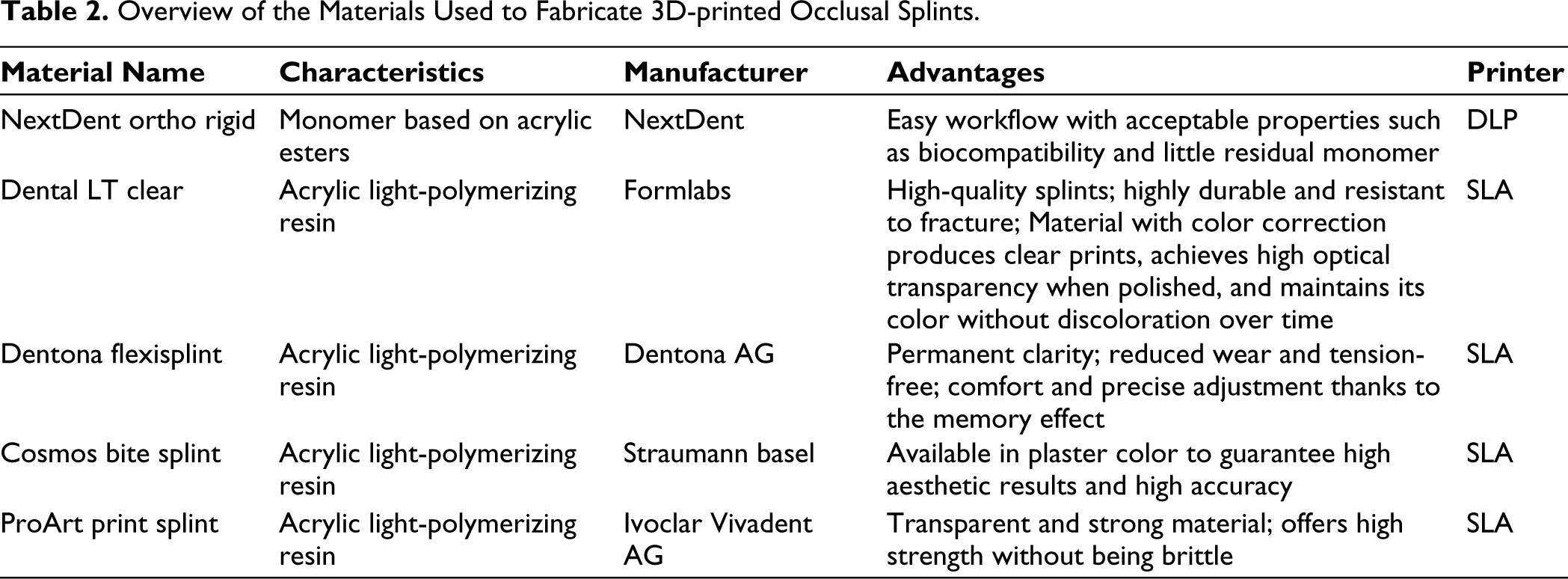
More recent research by Pripic further investigates various 3D-printed materials suitable for splint fabrication. In another study, five different brand names were analyzed: NextDent Ortho Rigid, Dental LT Clear, Dentona Flexisplint, Cosmos Bite Splint, and ProArt Print Splint. NextDent Ortho Rigid is composed of a monomer based on acrylic esters, while the other four brands all utilize the same material, specifically an acrylic light-polymerizing resin. 18 They reported that the flexural strength of most 3D-printed materials and their surface hardness values are still inferior compared to the milled or cold-polymerized materials.
Non-acrylic light-polymerizing resins offer several benefits, including fewer allergic reactions, excellent biocompatibility, strength, durability, and rapid, cost-effective processing. These materials reduce shrinkage, enhance the final fit and working conditions, and provide superior aesthetics with a polished finish and strong resistance to external factors. However, shrinkage remains a challenge in 3D-printed dental devices due to the layer-by-layer solidification process. Technologies like DLP improve dimensional accuracy, but further advancements in material science, printing techniques, and specialized dental CAD software are essential to address shrinkage effectively.37,38
The degree of conversion of 3D-printed resin materials is affected by different post-curing techniques. The polymerization environment is important, according to studies; for instance, curing in an oxygen-free environment (such as nitrogen polymerization) produces superior outcomes because oxygen prevents correct polymerization. Additionally, the hardness and flexibility of the material can be affected by various rinse techniques, such as ethanol or isopropyl alcohol treatments. The printed resin is typically exposed to UV light for prolonged periods of time during post-curing procedures; changes in curing time frames also impact the final quality of the material.39,40
A pilot study compared the performance of milled splints and occlusal splints printed from thermos-flexible resin. The thermo-flexible resin appears to be a good substitute for milled splints for at least three months of clinical use, according to this randomized pilot trial. However, more research is required to evaluate its long-term efficacy. 41
An in vitro study evaluated flexible occlusal splints using three 3D printing resins: KeySplint Soft, IMPRIMO LC Splint Flex, and V-Print Splint Comfort. V-Print is acrylate-based, while KeySplint Soft and IMPRIMO LC are methacrylate-based. KeySplint Soft showed the lowest water sorption and highest flexural strength, elastic modulus, wear resistance, fracture toughness, and degree of conversion among the materials. 42
A study aimed to compare the fracture resistance of occlusal splints made of different materials after thermomechanical aging. The evaluated materials included two 3D-printed polymeric materials, a PMMA disc for CAD/CAM, and a conventional heat-cured acrylic resin (PMMA, resin splint, Nightguard Flex resin, and Disco ProArt CAD). The study found that the milled splints demonstrated the highest resistance to fracture. Among the printed splints, those made with a rigid flexural resin withstand the applied forces within acceptable ranges, suggesting that their clinical use may be preferable. 43
Comparison in Durability, Strength, and Biocompatibility
As of now, it can be summarized that 3D-printed devices are still less reliable compared to their analog or milled counterparts. In a study conducted by Prpic et al. (2023), the flexural strength and surface hardness of 3D-printed occlusal splints were evaluated against those of cold-polymerized and milled PMMA splints. 18 It was observed that 3D-printed splints generally exhibited lower flexural strength and VHN, except for one material that matched the strength of conventional splints. Similar results were also noted by Berli et al. (2020), Gibreel et al. (2022), and dos Santos Neto et al. (2023), and these findings were further supported by Valenti et al. (2024). Moreover, it was found that the subtractive method had a reduced surface roughness compared to the conventional method. 44 A systematic review by de Paula Lopez (2023) highlighted the superior mechanical properties of subtractive resins in terms of hardness, wear resistance, flexural strength, flexural modulus, and fracture resistance. 45 Grymak et al. (2022) also affirmed this by showing that subtractive materials had the least volumetric and vertical loss, but there was no statistically significant difference for the conventional method. 46 Regarding biocompatibility, the cytotoxicity of commercial 3D-printed resins was comparable to that of conventional splints.27,47,48 Additionally, Wedekind et al. (2021) found that 3D-printed splints released more THFMA after being exposed to water. 49
Customized Splints
The digital workflow in dentistry, featuring intraoral scanning and 3D printing, is used for creating surgical guides, models, and reconstructions.50,51 A precise jaw impression ensures a well-fitting detachable dental product like a splint. Kong (2022) found that intraoral scans and traditional methods offer a 3D accuracy below 0.1 mm. 52 3D printing involves fewer steps, resulting in consistent and precise fits. 53 Pillai’s research also highlights the accuracy of patient-specific splints through 3D printing. 54
Taking impressions can be challenging for individuals with periodontal issues. Attachment loss can create undercuts and gaps between teeth, where elastomeric materials might tear or distort when removed. This complication hinders the accurate creation of well-fitting splints and makes it hard to achieve precise impressions. However, digital scanners address these challenges without compression of tissues, which significantly enhances the probability of obtaining a splint that fits better. In digital workflows, a virtual articulator (VA) can be used, whereas traditional methods often require a physical articulator to align models and determine the jaw’s position. The VA digitally replicates the jaw connection, reducing issues like material deformation and misalignment that could affect the accuracy of occlusal contact reproduction. 55
The precision of a splint is also affected by the orientation in which it is printed. According to Vasques (2018), printing 3D-printed occlusal splints at a 0° orientation results in the best internal fit and accuracy. Accuracy gradually decreases when printing splints at 30° and 90° angles. 56 A better fit is ensured by printing at a 0° angle, which reduces the impacts of layer stepping and distortion, particularly on surfaces that come into contact with the teeth and surrounding anatomy. 56 Furthermore, Marcel’s study examined the accuracy of milled and 3D-printed splints and discovered that the findings were similar, with variations based on the measurement technique. 57 According to a different study, milled splints had improved flexural properties and greater wear resistance than 3D-printed splints. 58
Efficiency and Cost-effectiveness of 3D Printing
The fabrication of 3D-printed occlusal splints is a trending topic in the literature, as it is a relatively new area of study with limited information. For instance, there is still uncertainty regarding the production time for 3D-printed splints, as well as the materials used in this process. Much of the existing research focuses on crown and bridge fabrication, where the use of intraoral scanners has been shown to be faster compared to conventional methods. 59 This suggests promising potential for the production of splints through digital scanning techniques.
A 2018 article by Berntsen demonstrates that 3D printing offers a cost-effective and time-efficient approach to fabricating occlusal splints (Figure 1). This efficiency is attributed to the use of scanning and 3D printing technologies, which eliminate the need for intermediate procedures and physical materials. 60 Another study concluded that producing dental splints with a 3D printer is faster than using conventional methods. This increase in speed is attributed to streamlined manufacturing processes and a reduction in the number of appointments. 61 In addition, the 2022 study by Patzelt et al. demonstrates that the total time required to fabricate occlusal splints using conventional methods is significantly higher than the average time needed for digital production. 62
Example of a 3D-printed Splint Using Dental LT V2 Material (Formlabs).

The effectiveness in terms of cost is also very important. According to an article by Balhaddad, there are major advantages to using a 3D printer even if the initial cost and infrastructure costs might be high. For example, economic reductions over time might result from the ability to make customized splints effectively, especially in high-volume applications. 63
A highly relevant topic currently under discussion is the significant environmental impact of the healthcare sector. Sustainability is increasingly important in this field due to the substantial material waste it generates. According to Prasad’s conclusion, 3D printing is better in line with sustainability objectives since it generates less material waste than conventional manufacturing techniques. 64
Technical Challenges with 3D-printed Occlusal Splints
A new manufacturing method in dentistry, such as the introduction of 3D printing, also brings new challenges. There are differences and limitations among various types of printers, as well as among the different materials that can be used in 3D printing, necessitating thorough research.
Since 3D printing is still a relatively new technology, it is important to start by addressing the most obvious drawback. Previous research showed that in order to successfully incorporate AM technology into the dentistry industry, there is a need to significantly raise the level of expertise with 3D printing within dental offices. According to the study, better training for distributors, resellers, and staff members, as well as greater public knowledge of technology, is necessary to accelerate the implementation of this breakthrough.64–66 Furthermore, little is known about the behavior of 3D-printed materials in the oral environment. The mouth presents various specific factors, such as saliva, pH fluctuations, and external influences, which can affect 3D-printed materials. Furthermore, there is a lack of information on the general biocompatibility of 3D-printed polymer materials, as well as plaque formation and elution behavior. 66
There are still limitations regarding the speed of splint fabrication and material thickness. It is commonly recognized that the thickness of each individual layer has a significant impact on this. Longer processing periods are associated with thinner construction layers, which also provide finer gradation. Another constraint on splint manufacturing speed is the build space’s size and the maximum construction speed that can be achieved. 67 Additionally, there is a drawback related to the materials available for 3D printing, because the range of resins that can be used is severely limited by this dependence on photopolymers. 68
According to an article by Grymak, focusing on the material qualities of 3D-printed splints, it can be assumed that their wear resistance, surface hardness, and bending strength are typically lower than those of standard PMMA or milled materials. 69
In a recent study, it was shown that the mechanical and surface characteristics of 3D-printed soft occlusal splint materials were affected by post-curing methods under various atmospheric conditions (air and nitrogen gas) and printer types (DLP and LCD). Flexural strength, flexural modulus, fracture toughness, VHN, water sorption, water solubility, and degree of double bond conversion (DC%) were among the parameters that were evaluated. While the DLP printer created materials with better flexural strength, modulus, and toughness, the LCD printer produced smoother surfaces with higher conversion rates and less water absorption. In particular, the mechanical characteristics improved by 10%–15% after curing in nitrogen, especially when using the DLP printer. 70
3D-printing or Milling?
The future of dental milling and 3D printing is dynamic, with each technology offering distinct benefits. Milling remains a reliable method for durable and biocompatible restorative devices, thanks to advancements in efficient, multi-material machines. In contrast, 3D printing excels in design flexibility and quick production of complex geometries. The chairside concept allows for rapid in-office production of splints, reducing patient wait times and enabling same-day fit. Although initial costs are lower for 3D printing and it reduces long-term expenses by minimizing labor, milling remains superior for certain materials and applications. However, 3D printing is particularly advantageous for high aesthetic outcomes and fit. 71 Moreover, additional research linking hybrid designs72,73 or varying stiffness 74 with AM technology is necessary. In summary, a clear need remains for extensive clinical validation studies comparing the durability and effectiveness of 3D-printed versus milled splints to better inform their adoption in clinical practice.
Conclusion
In conclusion, the use of 3D printing in dentistry has provided a significant improvement in the production of occlusal splints, replacing laborious and time-consuming traditional methods. When combined with intraoral scanning, 3D printing allows for the creation of highly accurate, customizable, and cost-effective splints with reduced clinical time and easy replacement. However, challenges remain, particularly in the mechanical properties and long-term performance of certain 3D-printed materials, necessitating additional research into non-acrylic and flexible resins to improve durability and biocompatibility.
Footnotes
Acknowledgements
The authors would like to thank Formlabs for providing the 3D-printed occlusal splint used in the photograph.
Authors’ Contribution
Celine van Lingen - conceptualization, methodology, writing—original draft
João Paulo Mendes Tribst
Conceptualization, resources, writing—review and editing, supervision
Data Availability Statement
All data supporting the findings of this study are included within the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
Ethical permission was not applicable for this article, as this is a review article drafted from various research articles and not from patients directly.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Consent was not applicable, as this is a review article compiled from various research articles and guidelines and not from patients directly.