
Abstract
Aim:
Children with sickle cell disease (SCD) are prone to many complications. However, little is known about oral infectious. This study aimed to assess the oral health status of pediatric patients with SCD and explore the associations between oral health conditions and clinical complications of SCD.
Materials and Methods:
A cross-sectional study was conducted in children with SCD admitted to the pediatric wards of two government hospitals in Jeddah city. The children were examined for dental caries, gingival diseases, oral lesions, and dental infections. Oral findings were compared between children who were hospitalized for vaso-occlusive crisis (VOC) or had a history of VOC in the last 6 or 12 months and those who were admitted for other reasons such as blood transfusion or other complications or had no history of VOC in the last 6 or 12 months.
Results:
A total of 107 children with SCD were included, with a mean age of 9.82 ± 3.82 years, of which 51 (47.7%) were females. Of the total, 58 (54.2%) were admitted because of VOC. There was a significant relationship between VOC and dental attrition (P = 0.038), osteomyelitis, and dental abscesses (P = 0.004). A significant association was found between the presence of dental abscesses and a history of osteomyelitis or avascular necrosis of long bones in the previous 12 months (P = 0.001 and P = 0.041, respectively).
Conclusion:
Dental abscesses and non-carious lesions are likely to be associated with VOC; however, further prospective cohort studies are warranted to confirm this association and establish a causal relationship.
Keywords
Introduction
Sickle cell disease (SCD) is an inherited blood disorder that affects the hemoglobin in red blood cells, which deliver oxygen to cells throughout the body. 1 Children with this disorder have a variant of hemoglobin, hemoglobin S, which distorts the red blood cells into a sickle shape, making them delicate and prone to rupture. 2
The symptoms of SCD include anemia, as sickle cells are fragile and can easily break apart and die, leaving the patient without sufficient red blood cells. 3 SCD has a significant association with morbidity and mortality, with a common clinical manifestation of vaso-occlusive crisis (VOC), in which the patient experiences episodes of pain when sickle cells clog the small vessels. 4
SCD is prevalent in the Middle East and Africa. In Saudi Arabia, SCD constitutes a significant health and economic burden, among other autosomal recessive genetic disorders; and the epidemiological figures vary across the region and are highly related to consanguine marriage.5–7 A cross-sectional population study in Saudi Arabia which screened a total of 488,315 individuals found that 4.20% had sickle cell traits and 0.26% had SCD. 8 Additionally, another cross-sectional community-based survey was conducted to screen SCD in 45,682 children and adolescents, and it concluded a prevalence of 24 per 10,000 children. 9 This community study recruited participants from each of the 13 regions of the Kingdom of Saudi Arabia.
Little attention has been paid to the oral manifestations of SCD, such as enamel hypo-mineralization and pulpal necrosis, which can greatly increase the risk of dental infection .10–12 Dental caries is a common manifestation in patients with SCD, particularly in those with low socioeconomic status.13,14
Very little evidence suggests that dental infections in SCD may increase the likelihood of a sickle cell crisis event. 15 A cross-sectional study from the United States indicated that dental infections in patients with SCD increased the likelihood of hospital admissions. 16
Few studies have assessed the association between dental infections and VOC in children with SCD. Therefore, this study aimed to assess the oral health status of patients with SCD and to explore the associations between oral health conditions and clinical complications of SCD. We hypothesized that oral health conditions are associated with clinical complications of SCD.
Material and Methods
Study Design and Data Collection Procedure
This cross-sectional study was carried out in the pediatric hematology wards of two Saudi Arabian government hospitals, King Abdulaziz University Hospital (KAUH) and King Fahad Armed Forces Hospital (KFAFH) in Jeddah, between September 2019 and September 2020.
A non-purposive sample of all children with SCD (0–18 years old) was admitted to the KAUH and KFAFH. The inclusion criteria were children with SCD admitted at two governmental hospitals whose parents agreed to participate and signed the consent forms. Children of parents who refused to participate in the study were excluded. Dental examinations were performed on all children with SCD, and the parents completed a questionnaire. The medical histories of the children were obtained from the institutions’ electronic file systems. Chief complaints, medical history, general examination, review of systems, cause of admission and history of complications in the previous 12 months (e.g., VOC, acute splenic sequestration, leg ulcers, avascular necrosis of long bones, osteomyelitis, pulmonary infection, stroke, cerebral infarction, vascular complication, organ failure, psychological dysfunction and splenomegaly) were among the medical history questions.
Ethical Approval
The study was approved by the Research Ethics Committees of King Abdulaziz University Faculty of Dentistry (Approval No-154-12-18) and KFAFH (REC-318-2020). Written informed consent was obtained from parents prior to the study.
Sample Size Calculation
G. Power software was used to calculate the sample size 17 (3.1.9.4) based on a previous study conducted on children with SCD in Jeddah 18 using the outcome variable hospitalization of SCD. Based on this study, the effect size was 0.2 and the power was 80%. The calculation was based on a significance level of 0.05, and the sample size required was found to be at least 100 children diagnosed with SCD.
Dental Examination and Study Instrument
Dental examination was performed by a single trained calibrated dental examiner using a probe, mirror, and flashlight in the hematology ward. The examiner examined children twice with one-week difference between both examinations. Caries experience was classified as either the presence or absence of caries, based on the definition of caries (d-decayed) according to the World Health Organization criteria. 19 Caries risk was categorized based on the American Academy of Pediatric Dentistry guidelines as high, moderate, or low. 20 Oral consequences that result from advanced stages of untreated caries were evaluated, such as presence of oral abscess, oral fistula, and oral ulcerations. The oral hygiene status of children was assessed using the Simplified Oral Hygiene Index and debris index component. 21
In addition, parents were given a data collection sheet comprising two parts. The first part included information on the child’s sociodemographic data, medical history, medications, and specific questions concerning the diagnosis and symptoms of SCD. Children were divided into three groups according to monthly family income based on the data from the central statistics and information website of Saudi Arabia 22 : high, moderate, and low with a monthly family income > 12,000 Saudi Riyal (SAR), 6,000–12,000 SAR, and < 6,000 SAR, respectively. The second part of the data collection sheet included information related to the child’s dental history, dietary and brushing habits, and specific questions related to frequency of sugar consumption.
Statistical Analysis
The parents answered the questionnaire, and dental examination and medical information data were entered on an Excel (Microsoft) sheet. All data were anonymized and saved securely using a password on a desktop computer. Statistical Package for the Social Sciences (SPSS) (version 22.0; SPSS Inc., Chicago, II, USA) was used to analyze the data. Descriptive statistics, frequency, and percentages were used to present the outcomes and independent variables. Associations between causes of hospital admission and SCD complications in the past 12 months were assessed using the chi-square test and Fisher’s exact test. SPSS version 20.0 was used to conduct the data analysis.
Results
Demographic Characteristics
The kappa values for intra-examiner reliability in the assessment of the presence of dental caries were 0.81, and oral consequence of caries was 0.82. A total of 107 participants were included in this study; 34 from KAUH and 73 from KFAFH. Table 1 shows the demographic characteristics of the participants, as well as their oral health status and behaviors, and their dietary patterns. The participants’ ages ranged from 1 to 18 years, with a mean age of 9.82 ± 3.82 years. About half of the participants (52.3%) were male, and nearly three quarters (74.8%) had a monthly income of 6,000–12,000 SAR.
Demographic Characteristics, Oral Health Status, Oral Health Habits, and Frequency of Sugar Consumption of the Study Subjects.
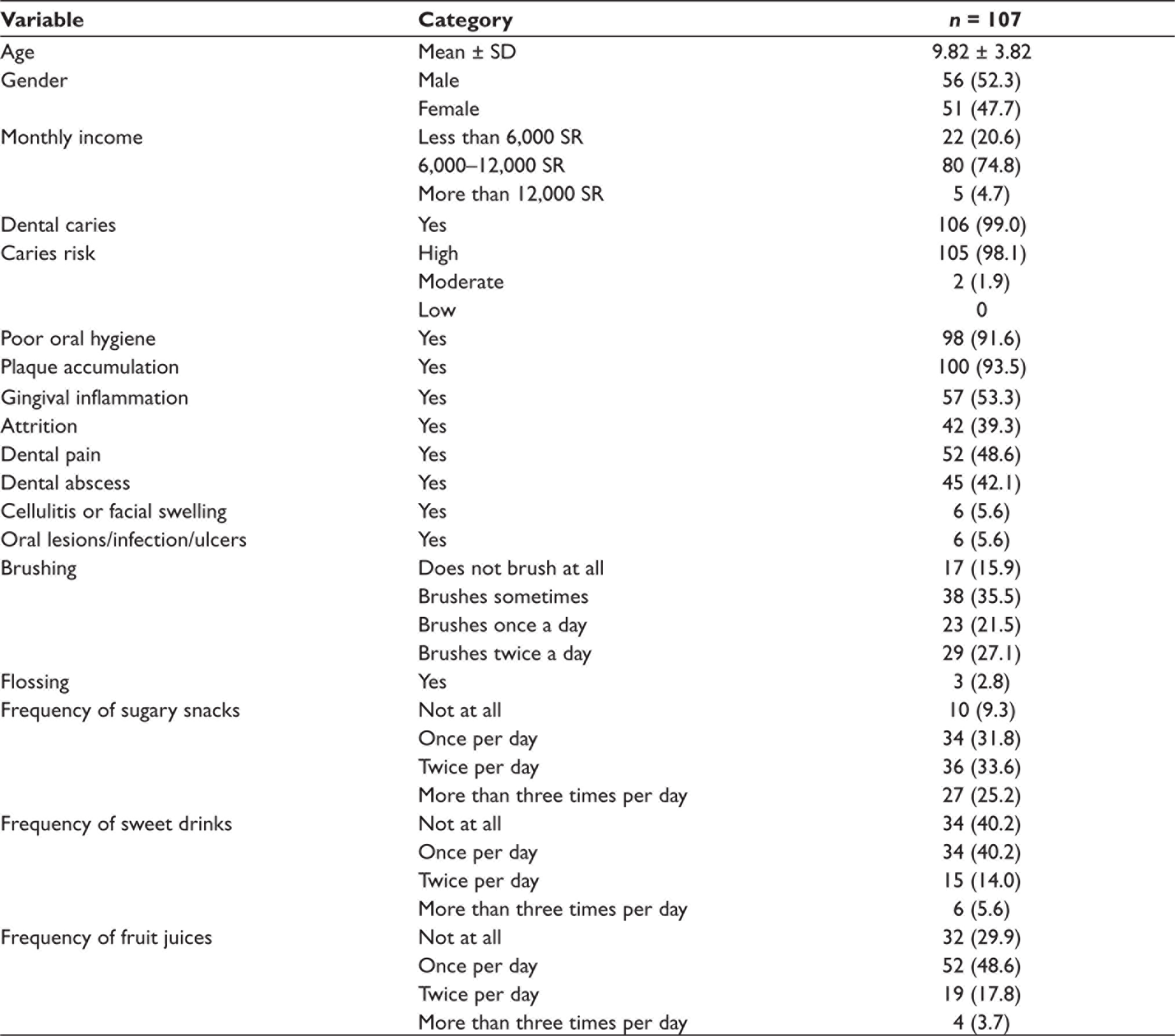
Almost all patients with SCD had dental caries (99.0%), were at high risk for caries (98.1%), had poor oral hygiene (93.6%), or had plaque accumulation (93.5%). Gingival inflammation and/or tooth pain was present in approximately half of the participants (53.3% and 48.6%, respectively). Attrition was observed in 39.3%, and tooth abscess was detected in 42.1% of the participants.
Relationships Between Oral Health Conditions and Causes of Admission
Table 2 shows the relationship between the oral health conditions and causes of admission. There was a significant relationship between VOC and dental attrition (P = 0.038), osteomyelitis, and dental abscesses (P = 0.004). Dental attrition affected 48.3% of the 58 patients admitted for VOC. Furthermore, 88.9% of patients admitted for osteomyelitis had a dental abscess. Other reasons for hospitalization were acute splenic sequestration, acute chest syndrome, stroke, splenomegaly, upper respiratory tract infection, pulmonary infection, cerebrovascular complications, asthma, septic arthritis, growth hormone deficiency, otitis media, type I diabetes mellitus, seizure episodes, cerebral infarction, hospital-acquired pneumonia, and diabetic ketoacidosis.
Association Between Oral Health Conditions and Admission Causes of the Children.
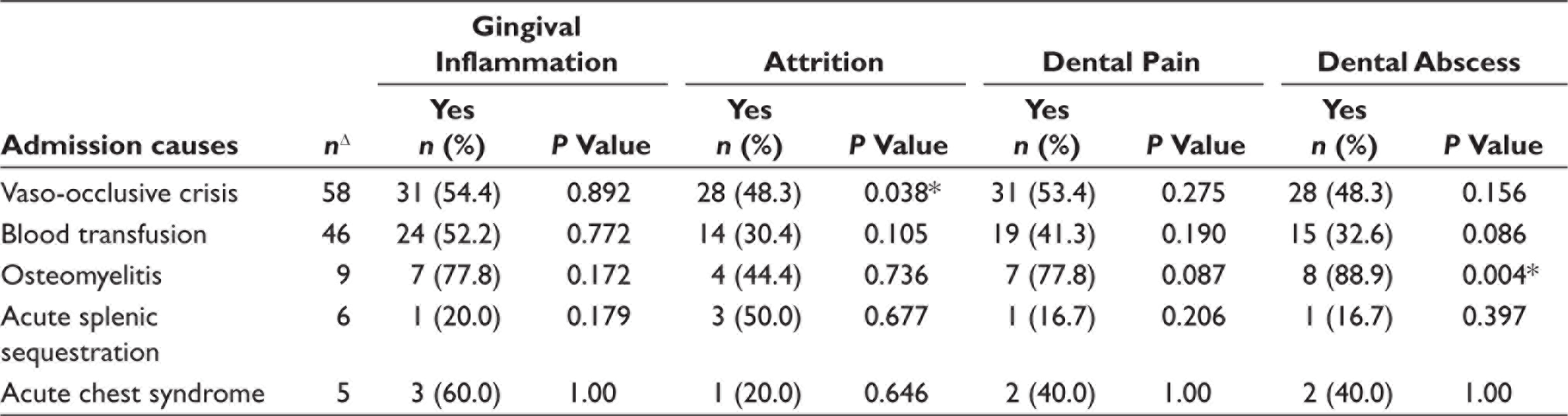
Chi-square test/Fisher Exact test.
ΔSome subjects were admitted for multiple causes.
Relationships Between Oral Health and SCD Complications in the Last 12 Months
Table 3 shows the relationship between oral health conditions and SCD complications in the children in the past 12 months. The presence of a dental abscess was associated with a history of osteomyelitis or avascular necrosis of the long bones in the previous 12 months (P = 0.001 and P = 0.041, respectively). More than three-quarters of the children (77.8%) with a history of osteomyelitis in the previous 12 months had a dental abscess. In addition, on dental examination, 69.2% of patients with a history of avascular necrosis in long bones in the previous 12 months had a dental abscess. Leg ulcers (2.8%), osteoporosis (1.9%), cerebral infarction (0.9%), hospital-acquired pneumonia (0.9%), urinary tract infection (0.9%), pulmonary embolism (0.9%), and abdominal infection (0.9%) were among the SCD complications recorded during the previous 12 months (Table 3).
Association Between History of Oral Health Conditions and SCD Complications of the Children.
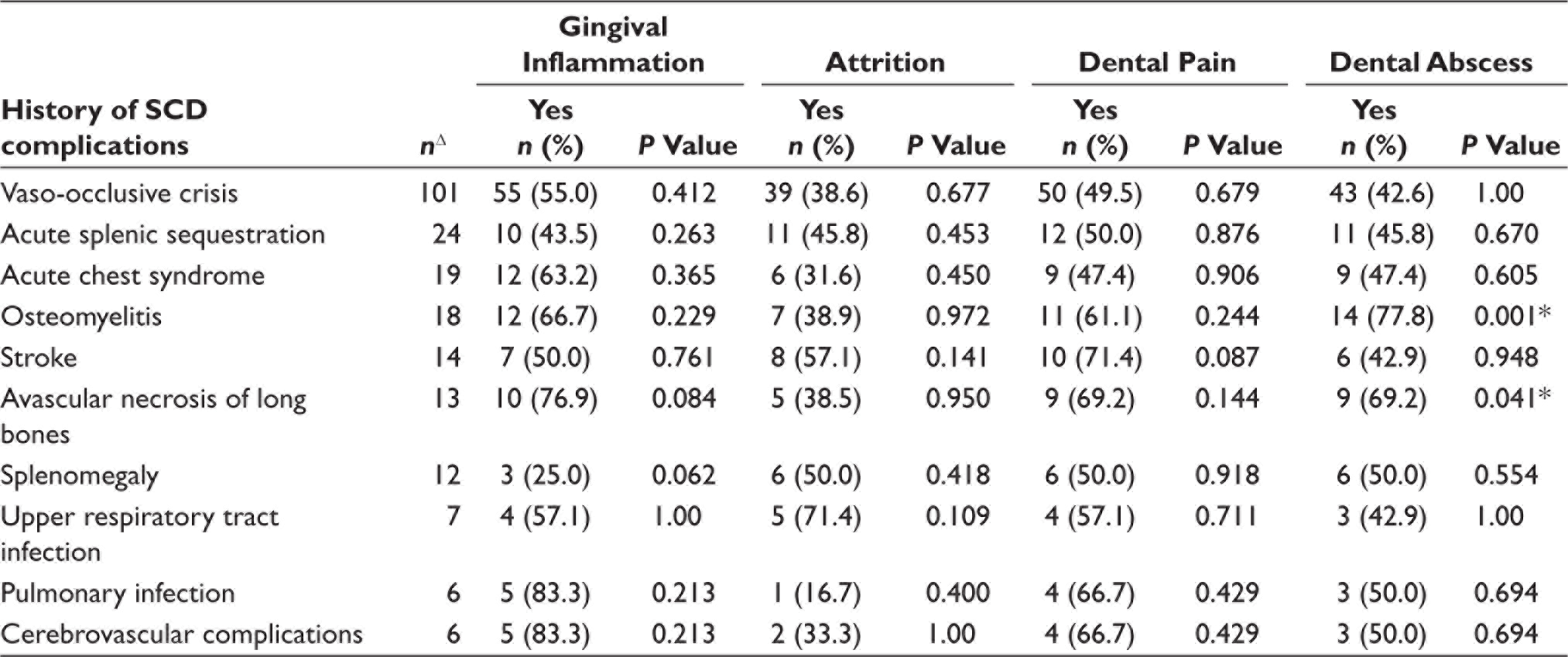
Chi-square test / Fisher Exact test.
ΔSome subjects had more than one SCD complication in the past 12 months.
Discussion
This study investigated the association between oral health conditions and the cause of admission in children diagnosed with SCD in two hospitals in Jeddah city. The findings of this study showed that SCD children were at high risk for caries and had poor oral hygiene. Additionally, an association was found between VOC and both osteomyelitis and dental abscesses in children diagnosed with SCD. This study found that the presence of a dental abscess in the last 12 months was associated with a history of osteomyelitis or avascular necrosis in children diagnosed with SCD.
Oral health issues are among the most debated clinical and pathological features of SCD. 23 The first published data go back to 1986, when Okafor et al. studied oral and dental conditions among Nigerian patients with homozygous SCD compared to age- and sex-matched controls. 24 Their findings were conflicting in that patients with SCD had a higher prevalence of intrinsic opacity (67.5% vs. 29%) and malocclusion of the teeth (35% vs. 17%). In contrast to our results, they reported that patients with SCD had a lower prevalence of dental caries (35% vs. 54%) compared to controls. 24
SCD is the most common type of hereditary hemoglobin disorder, affecting approximately 20–25 million people worldwide, with approximately 300,000 people being diagnosed each year. 25 Literature has demonstrated the association between SCD and parental consanguinity and concluded that a significantly higher incidence of inherited blood disorders was found among populations with high consanguinity marriage rates. 26 In 2003, the government of Saudi Arabia implemented a premarital screening program to reduce the incidence of SCD. 7 Therefore, these governmental efforts included premarital genetic counseling that was cost-effective in improving the awareness of parents and increasing the quality of life of children.
Recently, a study investigated the causes of hospitalization among children with sickle cell anemia in a group of private hospitals in Jeddah, Saudi Arabia. 18 In agreement with our results, they found that VOC (64.9%) was the most common cause of hospital admission, followed by infection (24.5%). Moreover, a case report suggested findings similar to our study that dental infections in patients with SCD increase the likelihood of developing a VOC event. 15 Similar to our findings, a study showed that dental infections among adult patients with SCD increased the susceptibility to hospitalization by 72%. 16
The pathogenesis of VOC is related to the damage of erythrocytes and transformation of normal blood cells into abnormal, rigid, sickle-shaped cells upon deoxygenation. 27 This injury leads to hemolytic anemia and the likelihood of blocked small blood vessels, causing a distinctive painful syndrome called VOC.28,29 These mechanisms lead to ischemia due to impaired organ perfusion, resulting in a wide range of clinical complications depending on the SCD phenotype. In our research, osteomyelitis and avascular necrosis of long bones were connected with dental abscesses and deteriorating oral health problems. Osteomyelitis is an inflammatory bone disorder that begins in the medullar cavity and spreads to the periosteum of the damaged bone.11,23 Because of the sickled cells, sludging develops in the microvasculature, blocking blood supply to the tissues and allowing osteomyelitis to set in. Bone necrosis and subsequent infection may result from persistent ischemia. 30 Due to VOC, pain in the jaws may happen and lead to acute and chronic ischemia and infarction followed by osteonecrosis. 31
SCD patients have a higher risk of general and dental infection than non-SCD patients. Conversely, inflammatory mediators from a dental infection could cause or worsen an existing medical emergency, necessitating a trip to the emergency room and possibly a hospital stay. 16 Therefore, it stands to reason that including dental care into medical management models for patients with SCD with a focus on prevention of oral diseases could result in long-term improvements in the overall quality of care for individuals with the condition.
In our study, almost all children with SCD had dental caries (99.0%). This finding provides implications for the prevention of dental disease among children diagnosed with SCD, which may decrease the cost of SCD management and its complications. Additionally, the prevention of oral infection will also protect the pediatric patients with SCD from developing serious complications, such as VOC, and improve their quality of life. Due to the limited number of investigations, a greater number of studies are required to properly evaluate this association.
To our knowledge, this study is the first to evaluate the association between oral health conditions and causes of admission among children diagnosed with SCD in Saudi Arabia. This study highlights the benefit of early oral preventive programs targeting newly diagnosed cases with SCD. There is no study without limitations. Further, since this is a cross-sectional study, its nature only allows for associations and cannot infer causality. 32 Moreover, the limitations of this study that the sample comprised patients attending only two government hospitals in Jeddah City, which makes generalization of the sample to community populations possible with caution. Additionally, in this study, the severity of dental caries was not assessed during dental examination.
Conclusion
Dental abscesses and non-carious lesions are likely to be associated with VOC; however, further prospective cohort studies are warranted to confirm this association and establish a causal relationship. Implementing oral preventive programs among newly diagnosed children with SCD can reduce the development of serious complications such as VOC and improve their quality of life.
Footnotes
Acknowledgements
The authors acknowledge Dr. Manal Almalik for her efforts in facilitating the research at King Fahad armed forces hospital. The authors also acknowledge all children who contributed to this study.
Author Contributions
All authors contributed either in writing the paper, recruiting data, examining and analyzing the data. All Authors had read, approved, and agreed to the submission of the manuscript.
Ethical Approval
The study and questionnaire were approved by the Research Ethics Committee of King Abdulaziz University Faculty of Dentistry (Approval No-154-12-18) and KFAFH (REC-318-2020).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study documents were approved by the Research Ethics Committee. The participant has consented to the submission of the article to the journal.