
Abstract
Aim:
The aim of this study was to quantify the association between the incidence and mortality of salivary gland cancer (SGC) with the consumption of tobacco and with the Human Development Index (HDI).
Materials and Methods:
An ecological study was designed using SGC incidence and mortality data in 172 countries in 2020, reported per 100,000 population with an age range of 10–85 years. Such dependent variables were obtained from the Global Cancer Observatory (GLOBOCAN). The prevalences of smoked and chewed tobacco were obtained from reports made in 2019, sourced from Global Burden of Diseases Study, while the HDI was obtained from the Human Development Report (2019) presented by the United Nations Development Program, and were considered independent variables. Statistical analysis was performed in Stata using Spearman’s correlation test.
Results:
In 2020, there were 53,583 new cases of SGC worldwide, and countries with very high HDI exhibited a higher incidence. In terms of mortality, there were 22,778 cases worldwide, and countries with a moderate HDI showed a higher number of deaths. SGC mortality was associated with chewing tobacco use overall and in women. Surprising negative associations were found with the incidence of SGC and tobacco smoking in men, as well as with mortality of SGC and smoking overall and in women. CGS mortality was negatively associated with the HDI and all its components.
Conclusion:
In this international overview, SGC mortality is associated with chewing tobacco in women, as well as with the HDI and its components.
Introduction
Tobacco use is considered one of the main risk factors for oral health, which affects the immune system and salivary flow, promoting problems such as dental caries and periodontal disease.1, 2 Tobacco use is now widely accepted as the cause of many types of cancer, including those that arise in the head and neck region. 3 Tobacco is responsible for approximately 15% of deaths worldwide, often from cancer, heart, or respiratory diseases. 4 There are two main modalities of tobacco use, smoked and smokeless. In the smoked modality, substances reach the lungs and disseminate systemically, while in the smokeless modality, substances come into direct contact mainly with the mucosa.5, 6 The way this product is consumed varies by region of the world: in Western countries, the most common modality is smoked, while in Asian countries (especially in South Asia), the most common modality is chewed. 7 It is a risk factor for salivary gland cancer (SGC); other SGC factors include human immunodeficiency virus (HIV) infection, exposure to radiation (therapeutic or military), as well as excessive consumption of high-cholesterol foods.8, 9
Cancer is one of the diseases with the highest rates of morbidity and mortality globally, with an incidence of 19,292,789 cases reported in 2020. Notably, 9,958,133 cases died from this disease,10, 11 making it a global public health problem. SGC is a rare disease, with an incidence of 0.4–2.6 cases per 100,000 population per year. There are 22 subtypes of this cancer. 12 The International Agency for Research on Cancer (IARC) reported an incidence of 53,583 cases and a mortality of 22,778 cases in 2020, affecting males more than females in both cases. 10 It mainly affects the major salivary glands (primarily the parotid gland), with only 23% affecting minor salivary glands. 13 The most common type of SGC is mucoepidermoid carcinoma; however, in countries such as Turkey, Croatia, or Brazil, adenoid cystic carcinoma has been found to be more common. There are variations in incidence and mortality rates among different countries, and it is unclear whether these variations are due to intrinsic factors associated with the level of development among countries or if they are idiosyncratic. These carcinomas are usually identified only in advanced stages due to the limited number of known risk factors, the wide diversity in the sophistication of healthcare services for diagnosis, and even the tumor location.14, 15
In the present study, we ascertained the role of smoking and chewing tobacco use in the incidence and mortality rates of SGC in the context of the Human Development Index (HDI) for 172 countries. This index was selected to determine whether differences in the development of different countries were associated with SGC or if SGC manifested similarly across all countries.
Materials and Methods
Design and Ethical Considerations
This ecological study was conducted using preestablished and publicly accessible databases. The study was registered with the Research and Advanced Studies Secretariat of the Autonomous University of the State of Mexico (DOCCSA-0321). Informed consent was not required because the data were available in public databases and the patients were not directly examined (face-to-face) for the present study.
Variables
The Global Cancer Observatory (GLOBOCAN) is responsible for updating estimates of the incidence and mortality of different types of cancer using data from the IARC.
16
These data provided by GLOBOCAN are used to evaluate the effectiveness of prevention and treatment strategies implemented in each country.
17
The data obtained from the database are publicly accessible (
The independent variables were the prevalence of smoked and chewed tobacco, and the HDI. The prevalence of smoking tobacco by sex was obtained from Reitsma et al., 18 reported per 100,000 population, while the prevalence of chewing tobacco by sex was obtained from Kendrick et al. 19 described in percentages. The average prevalence of both smoking and chewing tobacco was also obtained to provide an overall picture of tobacco use (all reported data are obtained in 2020).
The HDI is based on three dimensions: education, quality of life, and health, aiming to provide a real scale of personal growth for each country.20, 21 Based on these dimensions, countries can be classified into very high, high, moderate, and low HDI categories.
7
Although this index reflects that a country with a high HDI is in better conditions than those with a moderate or low index, it does not exhaustively quantify the inequality, poverty, and human safety in each country. Additional evaluations should be conducted for these factors.22, 23 The HDI data were obtained from the United Nations Development Program, Human Development Report (
Statistical Analysis
The association between the incidence and mortality of SGC with the prevalence of smoking and chewing tobacco and the HDI was determined using Spearman’s correlation, with p-values < 0.05 considered statistically significant. The statistical analysis was performed using Stata 14 (StataCorp LLC, Texas, USA).
Results
Epidemiology of SGC
In 2020, there were 53,583 new cases of SGC worldwide, with countries having a very high HDI showing a higher incidence. Males were more affected, accounting for a total of 29,694 cases. In terms of mortality, there were 22,778 cases worldwide, with moderate HDI countries showing a higher number of deaths. Once again, males were more affected, with 13,353 cases.
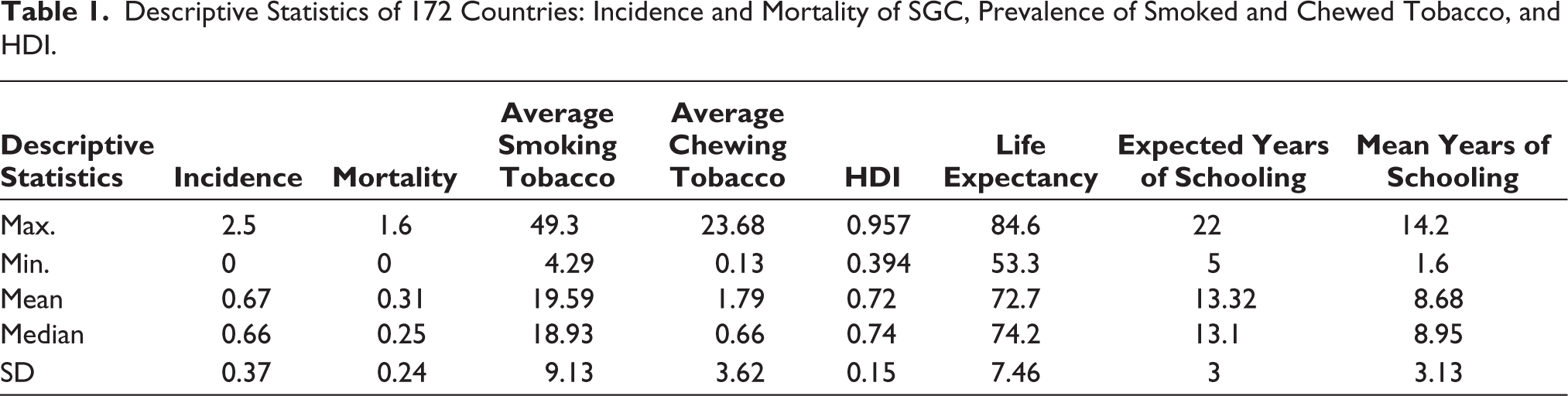
Table 1 shows the results of the descriptive analysis of the study variables. The incidence rates of SGC in 172 countries are shown in Table 2 (complete data in Supplementary Table S2). The results indicate that Cape Verde (2.5), Togo (2.1), and Haiti (2.0) had the highest incidence rates of this condition, while Suriname, Timor-Leste, and Djibouti had the lowest incidence rates, with zero reported cases. In terms of incidence by sex, Haiti, Togo, and Cameroon had the highest incidence rates in men, while Cape Verde, Togo, and Benin had the highest incidence rates in women.
Descriptive Statistics of 172 Countries: Incidence and Mortality of SGC, Prevalence of Smoked and Chewed Tobacco, and HDI.
Incidence of SGC, for Example, in the Top 10 countries With the Highest and 10 With the Lowest Incidence Rate.
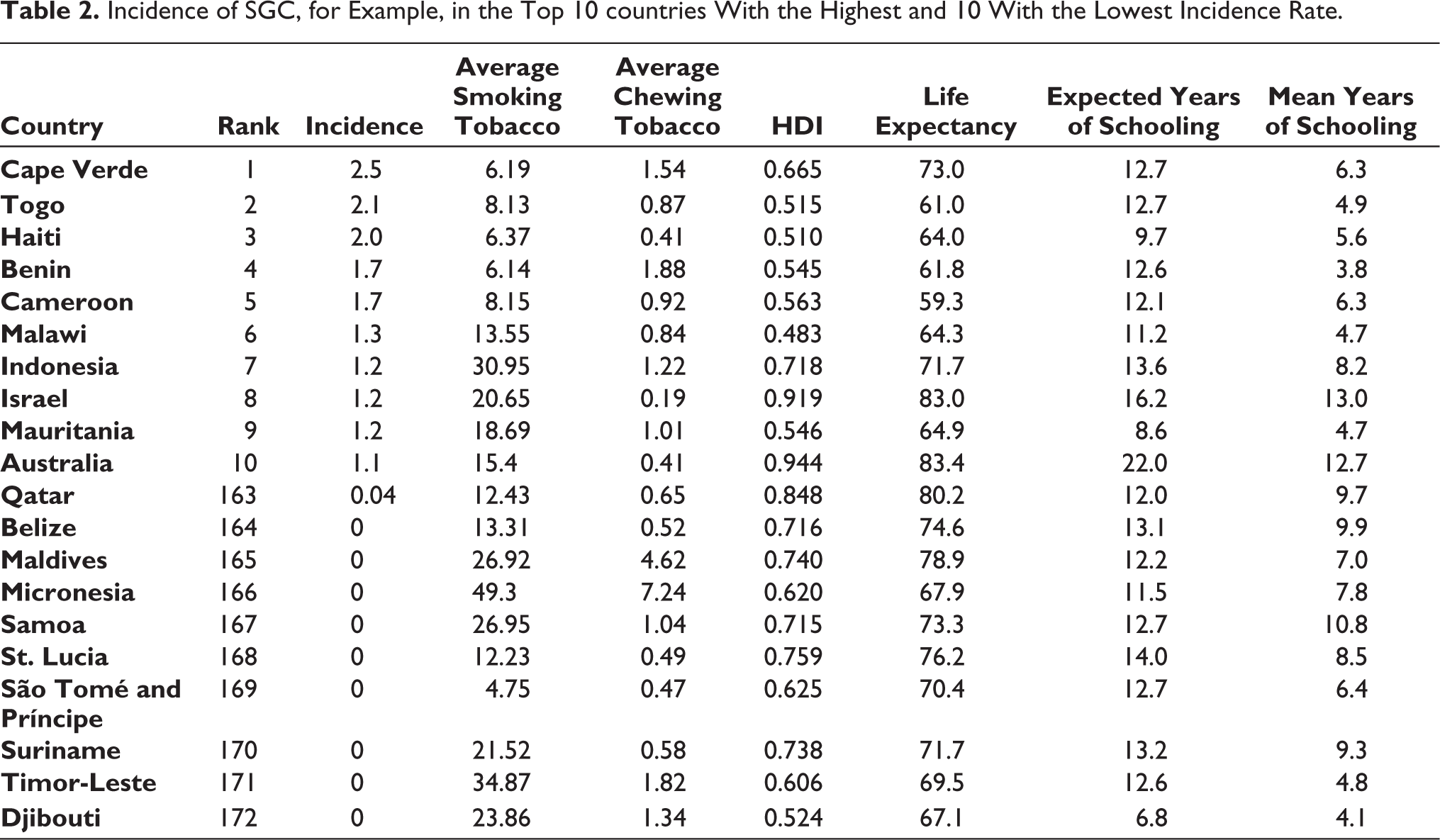
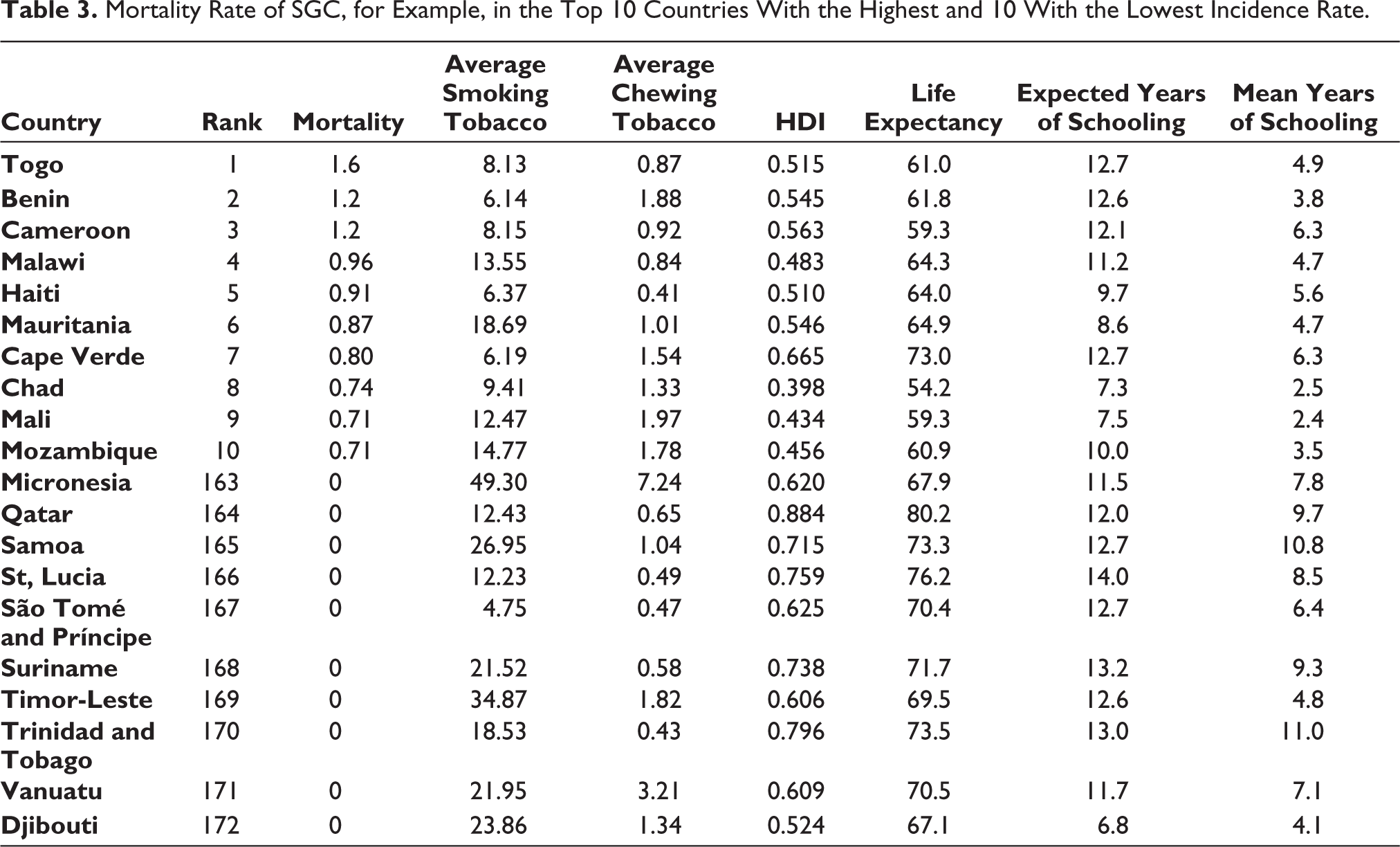
Table 3 shows the mortality rates (complete data in Supplementary Table S3). The countries with the highest mortality rates were Togo (1.6), Benin (1.2), and Cameroon (1.2), while the countries with the lowest mortality rates were Trinidad and Tobago, Vanuatu, and Djibouti, all with zero cases. As for mortality by sex, Togo, Haiti, and Benin had the highest mortality rates in men, and Cabo Verde, Togo, and Benin had the highest mortality rates in women.
Mortality Rate of SGC, for Example, in the Top 10 Countries With the Highest and 10 With the Lowest Incidence Rate.
Prevalence of Smoking and Chewing Tobacco Worldwide
The highest prevalence of smoking tobacco among women was observed in Bosnia Herzegovina, followed by Serbia and Micronesia. In men, East Timor, Micronesia, and Indonesia showed the highest prevalence rates of smoking tobacco.
As for chewing tobacco in women, Bangladesh showed the highest prevalence, even higher than in men. Bhutan and Cambodia also had a significant prevalence of chewing tobacco use. Among men, Nepal, Bhutan, and India had the highest prevalence of chewing tobacco use.
Human Development Index
The countries with the highest HDI were Norway (0.957), Ireland (0.955), and Switzerland (0.955), while those with the lowest HDI were Chad (0.398), Central African Republic (0.397), and Niger (0.394).
The country with the highest life expectancy was Japan (84.6 years), while the lowest was the Central African Republic (53.3 years). Australia had the highest expected years of schooling (22 years), while Eritrea had the lowest (5 years). In terms of mean years of schooling, Germany ranked the highest (14.2 years), while Burkina Faso was the lowest (1.6 years).
Correlation between the Incidence and Mortality of SGC and the Prevalence of Smoking and Chewing Tobacco
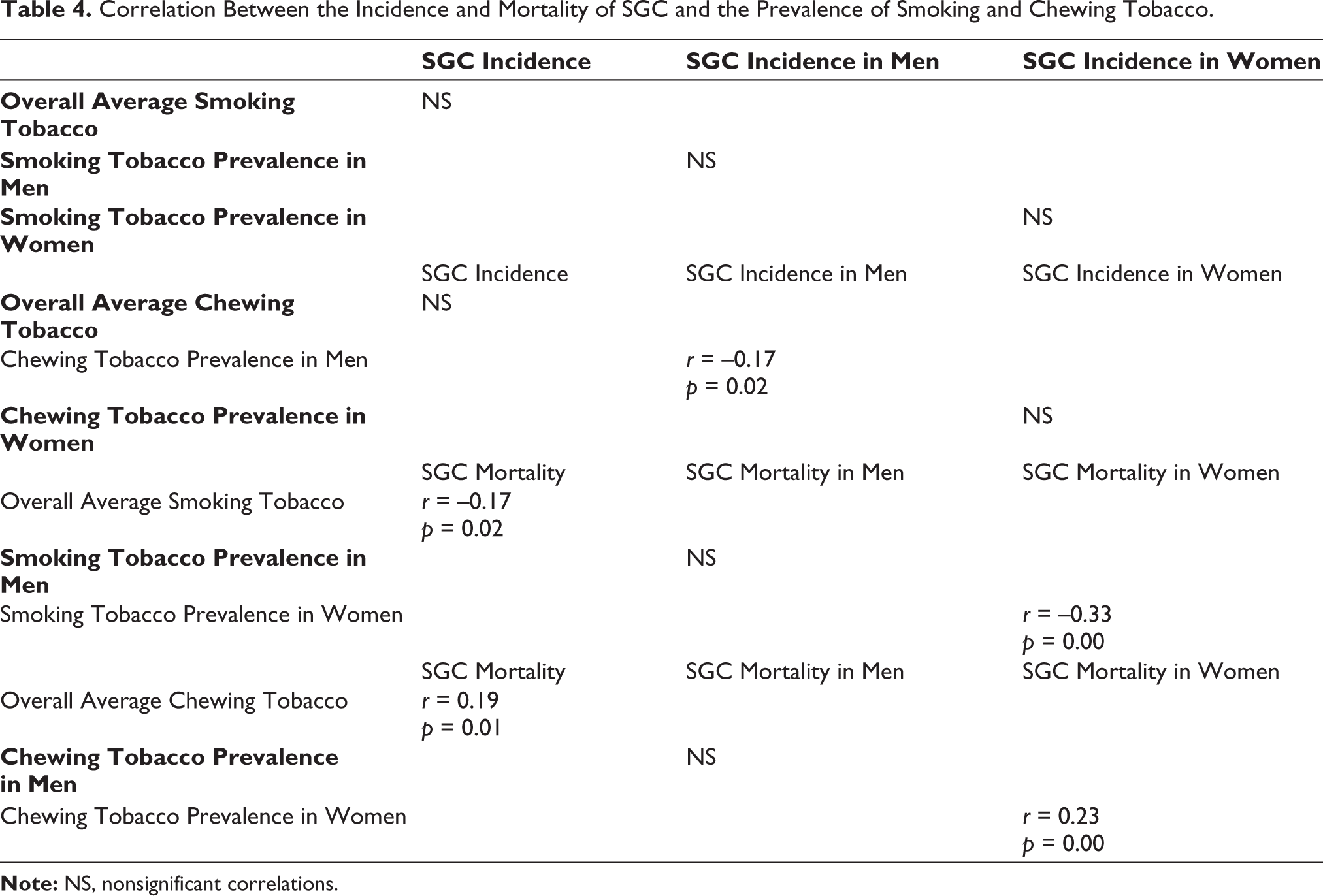
No statistically significant differences were found between the incidence of SGC (overall and by sex) and the prevalence of smoking tobacco. In the case of chewing tobacco, only a negative correlation was found between the prevalence of chewing tobacco in men and the incidence of SGC in men (p = 0.023, r = –0.173) (Table 4).
In the analysis of SGC mortality and the prevalence of smoking and chewing tobacco, a surprising negative correlation was found between the average smoking tobacco and overall SGC mortality (p = 0.022, r = –0.174), as well as a negative correlation between the prevalence of smoking tobacco in women and SGC mortality (p < 0.001, r = –0.334). As for chewing tobacco, a positive correlation was found between the average chewing tobacco and overall SGC mortality (p = 0.012, r = 0.192). The same trend was observed between the prevalence of chewing tobacco in women and SGC mortality (p = 0.002, r = 0.233) (Table 4).
Correlation Between the Incidence and Mortality of SGC and the Prevalence of Smoking and Chewing Tobacco.
Correlation between the Incidence and Mortality of SGC and the Human Development Index
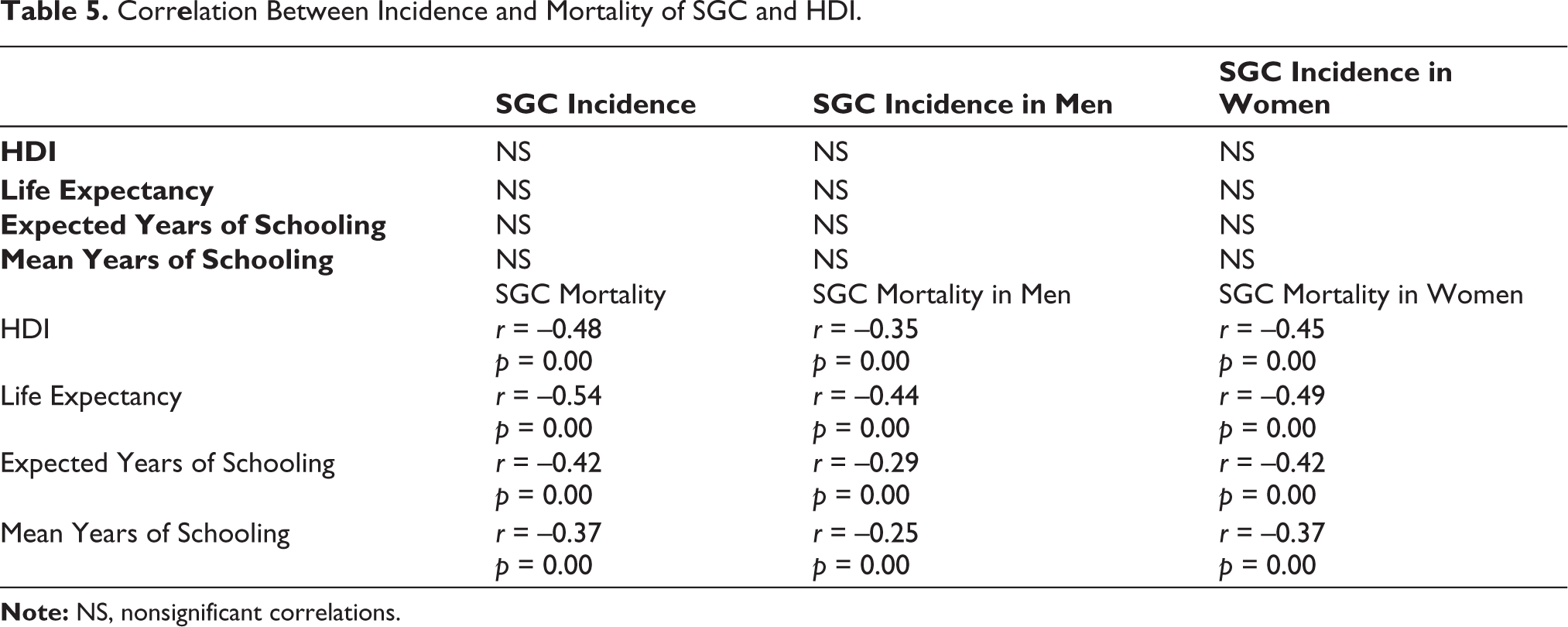
No statistically significant differences were observed between SGC incidence (overall and by sex) and HDI and its components. However, overall SGC mortality showed a negative correlation with HDI (p < 0.001, r = –0.480), life expectancy (p < 0.001, r = –0.545), expected years of schooling (p < 0.001, r = –0.423), and mean years of schooling (p < 0.001, r = –0.375). SGC mortality in men had negative correlations with HDI (p < 0.001, r = –0.359), life expectancy (p < 0.001, r = –0.445), expected years of schooling (p < 0.001, r = –0.290), and mean years of schooling (p = 0.001, r = –0.252). Finally, SGC mortality in women had negative correlations with HDI (p < 0.001, r = –0.458), life expectancy (p < 0.001, r = –0.496), expected years of schooling (p < 0.001, r = –0.423), and mean years of schooling (p < 0.001, r = –0.370) (Table 5).
Corr
Discussion
In the present study, we analyzed the incidence and mortality rates of SGC in 172 countries and their relationship with smoking and chewing tobacco use, as well as with the HDI. SGC is an entity with a low incidence rate; however, countries such as Japan and the United States have shown an increasing trend in the past 40 years. 24 We observed that males were more affected, which contradicts the findings of Alsanie et al., who found a slight preference for females. 25 Our study showed that the difference between sexes was not significant. The countries with the highest incidence rates were African countries, which also differs from Donaldson et al., who found low rates in African men despite not finding significant differences in incidence rates among ethnicities. 26
The mortality rates were higher in men than in women, with a significant difference than the incidence. In a study conducted in Germany, it was demonstrated that mortality rates by sex were very similar, especially in patients older than 79 years. 27 Likewise, higher mortality and incidence rates were found in African countries. This finding is comparable to that reported by Chiruvella et al., whose finding showed that the worst mortality rates were observed in African American/Black patients, as well as a significant difference when comparing Caucasian/White patients with African American/Black patients. 28
Due to SGC being uncommon, there are poorly documented aspects about it. One aspect is the risk factors, although radiation, smoking, and obesity have also been suggested. 29 In the present study, we quantified the correlation between smoking and chewing tobacco use with the incidence and mortality of SGC, and the results showed that there were no statistically significant differences between the incidence of SGC (overall and by sex) and smoking tobacco. In the case of chewing tobacco, only a negative correlation was found in men. These results are consistent with those obtained by Radoï et al., who did not find an association between SGC and smoking tobacco use, and they found elevated, but not significant, risks for smokers with more than 25 years of tobacco use and more than 16.5 pack-years. 30 It could be important in future research to focus on specific types of SGC to determine if any particular type is more closely associated with smoking tobacco use. Leopard et al., for instance, found high levels of smoking in cases of myoepithelial carcinoma. 29
Regarding the relationship between mortality and the prevalence of smoking and chewing tobacco use, a negative correlation was found with smoking tobacco, suggesting that smoking tobacco may not play a critical role in the evolution of this condition. In the case of chewing tobacco, however, a positive correlation was found between overall mortality and chewing tobacco, as well as between mortality in women and the prevalence of chewing tobacco in women. Such findings suggested that higher consumption of this product leads to increased mortality in women. This finding needs to be scrutinized in future studies to determine which substances contribute to this situation or if it affects a specific type of SGC.
No correlation was found in the relationship between SGC incidence and HDI, despite reports from the IARC in 2020 stating that countries with very high HDI (19,391 cases) and high HDI (18,634 cases) had a higher incidence of this cancer. 10 However, these trends did not appear to be significant. It is generally known that the incidence disproportionately affects highly developed countries, possibly due to having more advanced healthcare systems capable of diagnosing cases more effectively. However, it is believed that between 2008 and 2030, countries with low HDI will experience a 100% increase in incidence, and countries with moderate HDI will experience an 81% increase. 31 Regarding mortality, negative correlations were found with HDI and all its components. This can be interpreted as countries with lower HDI having high mortality rates, as reported by the IARC, and countries with moderate HDI having a higher mortality rate, with 7,376 cases. Again, this may be due to these countries lacking access to effective healthcare services, resulting in late diagnosis and possibly inadequate treatment. A similar pattern was reported by Fidler et al., mentioning that mortality rates seemed to be comparable overall across the four levels of HDI. However, a deeper analysis revealed that the highest burden of cancer occurred in countries with moderate and low HDI, suggesting a poorer survival prognosis. 31 A previous study on lip and oral cavity cancer (LOCC) 32 followed the same methodology. It found correlations between various socioeconomic indicators and tobacco use, with LOCC incidence and mortality. Some correlations were surprisingly counterintuitive from what was expected.
Using aggregated or summarized population-based data in research (such as GLOBOCAN and Global Burden of Disease Study) can offer valuable insights into various aspects of health, behavior, and social dynamics. However, there are also potential risks and challenges associated with the use of such data. Some key considerations regarding the use of this aggregated data can be summarized; for example, data may not be truly representative of the entire population, leading to bias. This can affect the generalizability of research findings; the quality of data (collection and capture) can vary, and inaccuracies may be present, leading to erroneous conclusions; handling large datasets requires robust data management practices to organize, store, and analyze the information effectively; correlation does not imply causation and misinterpretation of population-based data can lead to erroneous conclusions about causal relationships; extrapolating findings from population-based studies to specific individuals may not always be accurate; and researchers must be cautious about making broad generalizations.
The present study provides international comparisons relevant to various regions of the world; however, the study has limitations that should be highlighted to objectively interpret the findings. The first limitation is that since it is an ecological study, the ecological fallacy cannot be avoided, and our results cannot be extrapolated to individual cases. Second, SGC is an entity with 22 subtypes; ideally, each of them should be studied individually to determine the main risk factors relevant to each subtype. Finally, in the present analysis, no data were available on risk factors for SGC; for example, having received therapeutic radiation in patients who suffered from some type of head and neck cancer; viral infections such as human immunodeficiency virus or Epstein-Barr virus; or nutritional deficiencies, such as consuming high levels of cholesterol, that considerably increase the risk of suffering from GCS. Likewise, the correlation analysis used is susceptible to errors since it only refers to the variables studied and does not provide information beyond the correlated data.
Conclusions
The incidence of SGC was negatively associated with smoking tobacco in men, while the mortality of SGC was negatively associated with the prevalence of smoking tobacco overall and in women. The mortality of SGC was only associated with chewing tobacco overall and in women, as well as with HDI and its components. These findings emphasize the need to improve policies for access to healthcare services in order to facilitate timely diagnosis and treatment to reduce the gap in SGC mortality between developed and less developed countries.
Supplemental Material
The supplemental material for this article is available online.
Footnotes
Acknowledgements
This study was supported by a scholarship awarded by the National Council of Humanities, Science, and Technology of Mexico (CONAHCYT) to Antonio Hernández-Morales.
Abbreviations
SGC, salivary gland cancer; HIV, human immunodeficiency virus; HDI, Human Development Index, GLOBOCAN, The Global Cancer Observatory; IARC, International Agency for Research on Cancer; LOCC, lip and oral cavity cancer.
Authors’ Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was registered with the Research and Advanced Studies Secretariat of the Autonomous University of the State of Mexico (DOCCSA-0321).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable