
Abstract
Aim:
Patients with Beckwith-Wiedemann syndrome (BWS) often present with macroglossia and aberrant dentoskeletal features, which may increase the prevalence of malocclusion and complicate conventional orthodontic management (OM). The aim was to comprehensively review the available literature regarding the OM of patients with BWS.
Materials and Methods:
Indexed databases were searched until February 2023. Clinical studies that addressed the dentoskeletal manifestations and OM of patients with BWS were included. A literature search was performed in accordance with the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Results:
Notably, 8 out of 2,664 initially-identified studies were included. Six of the studies were case reports/case series and two were retrospective clinical studies. A total of 35 patients with BWS who received orthodontic treatment (OT) were included. Common dentoskeletal and soft tissue traits included the presence of macroglossia, obtuse gonial angle, and anterior open bite. Some form of maxillary transverse discrepancy was found in nine patients. The OT modalities that were utilized included extraoral appliances, functional appliances, removable appliances, interarch elastics, and fixed appliances. The outcome of the OT was reported as successful in five studies. The follow-up, as reported by three studies, ranged from 8 months to 6 years, and the results of the OT were maintained. Adjunct interdisciplinary therapeutic procedures included glossectomy, oral physiotherapy, and orthognathic surgery.
Conclusion:
Based upon limited available evidence, OT in conjunction with tongue reduction surgery and/or myofunctional therapy can be successfully performed in children with BWS to manage various dentoskeletal discrepancies.
Keywords
List of Abbreviations
BWS: Beckwith-Wiedemann syndrome
EMG: Exomphalos, macroglossia, gigantism
BWSp: Beckwith-Wiedemann spectrum
OT: Orthodontic treatment
OM: Orthodontic management.
Introduction
Beckwith-Wiedemann syndrome (BWS) is the most common congenital overgrowth disorder.1,2 It presents with an estimated incidence of 1 out of every 13,700 births; 2 however, this is likely to be an underestimation, as mild phenotypes may go unrecognized. 2 BWS seems to affect both sexes almost equally, it has a worldwide distribution, 3 and it is associated with epigenetic–genetic alterations on chromosome 11p15.5. BWS more commonly occurs as a sporadic case; however, the role of a family history cannot be disregarded.2,4 Exomphalos, macroglossia, and gigantism are the most prevalent findings of the syndrome, which is why it used to also be referred to as the EMG syndrome. 4 Recently, BWS has been redefined as the Beckwith-Wiedemann spectrum (BWSp), as it consists of a large variety of phenotypes. 5 Patients with BWS may present with a variety of clinical findings, including macroglossia, macrosomia, abnormal earlobe creases/pits, hemihypertrophy, congenital heart defects, cleft palate, and others.2,4 Mental development is usually normal, but mental retardation may occur in a small amount of patients with BWS. 4 Children with BWS are at increased risk of developing tumors, which are usually malignant.2,4
The growth of the maxillofacial complex is connected to the growth and function of the soft tissues that surround it, also known as the functional matrix theory.6,7 For example, the resting position of the tongue and tongue size seem to have an effect both on tooth and jaw relationships.6,8 It has been suggested that tissue overgrowth manifestations (such as macroglossia) in patients with BWS may lead to a higher rate of dentoskeletal deformities and malocclusion, as well as respiratory problems, sleep apnea, and problems with speech.9,10 The concurrence of macroglossia with skeletal open bite malocclusion and mandibular protrusion has been documented in several patients with BWS.11–14 The presence of malocclusion in patients with BWS may negatively affect patients’ masticatory function, facial esthetics, and overall quality of life. 15 Patients with BWS often require an interdisciplinary treatment approach to manage the various cardiac, neurological, cognitive, and psychological features of the syndrome, as well as the orodental and craniofacial manifestations and alterations in oral function. In this regard, orthodontic treatment (OT) in conjunction with other dental and/or surgical treatment approaches can be an integral part of the overall interdisciplinary care of patients with BWS. It is speculated that syndrome and patient-related characteristics in patients with BWS may entail challenges in orthodontic management (OM), compromise the outcomes and long-term stability of OT, and warrant interdisciplinary therapeutic approaches. To the best of the authors’ knowledge, there are no studies in indexed literature that have reviewed the OM of patients with BWS. The aim of this study was to comprehensively review the available literature regarding the OM of patients with BWS.
Materials and Methods
Focused Question
In this review, the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines 16 were followed to assess the following focused question: “Is OT useful in the interdisciplinary management of patients with BWS?” The pattern of this review was customized to summarize the pertinent information.
Eligibility Criteria
The inclusion criteria were as follows: (a) clinical studies; (b) patients with BWS; and (c) patients undergoing OT. Commentaries, Letters to the Editor, Reviews, and Experimental Studies were excluded.
Information Sources, Search Strategy, and Study Selection
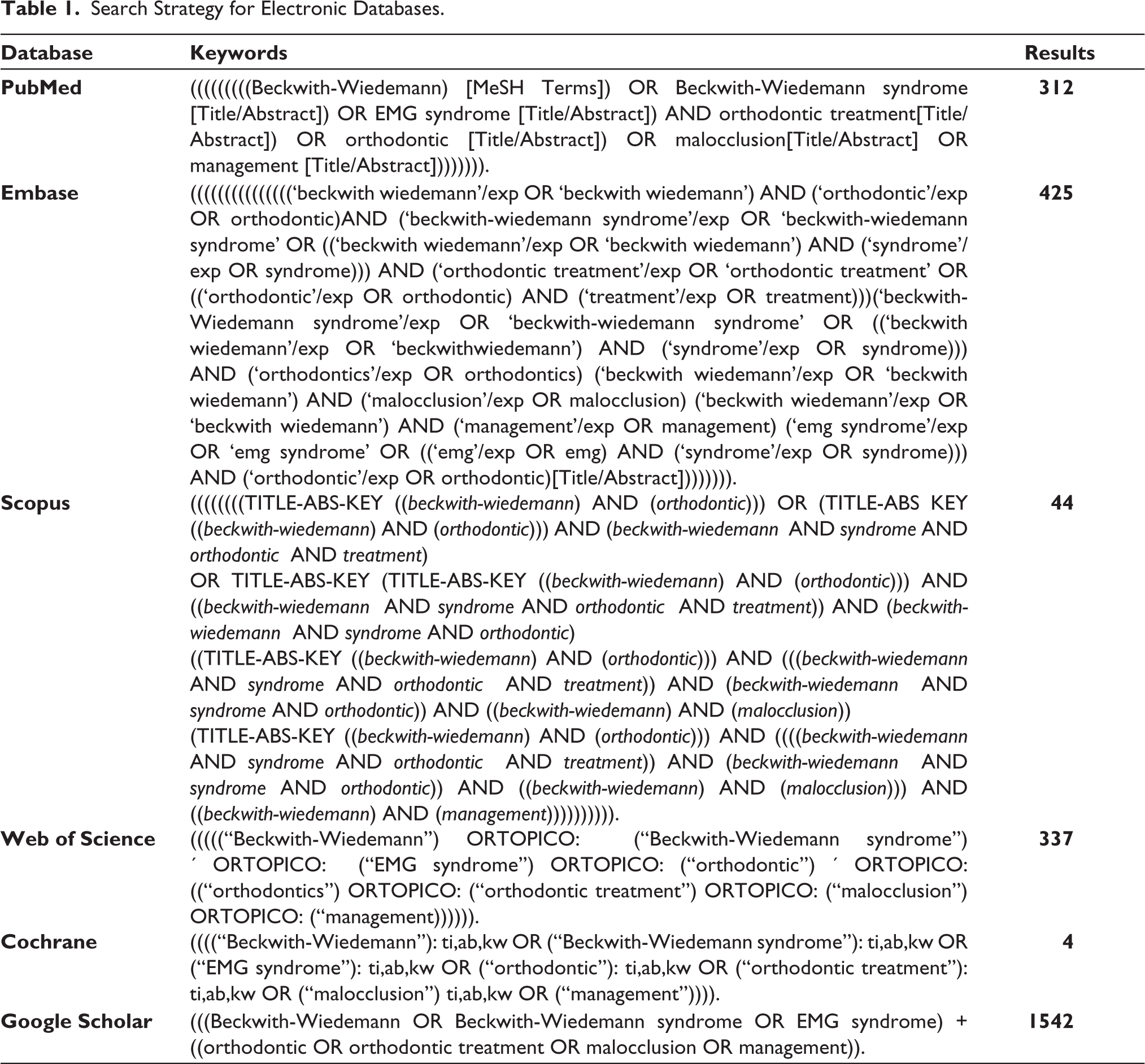
A search in the following electronic databases [EMBASE, PubMed (National Library of Medicine), Google Scholar, Web of Science, Cochrane, and Scopus] was conducted without time restrictions up to and including February 2023. The following MeSH terms were used: “Beckwith-Wiedemann,” “Beckwith-Wiedemann syndrome,” “orthodontic,” and “malocclusion,” and a customized search strategy was implemented by two authors (MK and LJ) (Table 1). The titles and abstracts of relevant articles were screened by two authors (MK and DM), and the full texts of relevant articles were independently read. Hand-search of the reference lists of relevant articles was also performed to collect possible articles that may have been missed in the previous steps. Disagreements were resolved via discussion between all authors.
Search Strategy for Electronic Databases.
Data Collection and Data Items
Data extraction from the included studies was performed independently by two authors (MK and LJ), and pertinent information was collected as follows: (1) reference; (2) study design; (3) number of patients; (4) demographic information; (5) oral manifestations of the syndrome and their treatment; (6) type of malocclusion and maxillofacial characteristics; (7) information regarding OT (such as age at initiation and end of OT, one- or two-phase OT, appliances, and retention); (8) outcome and follow-up of OT; and (9) additional adjunctive interdisciplinary treatment modalities. Disagreements related to data extraction were resolved through consensus discussion among all authors.
Risk of Bias of Individual Studies and Additional Analyses
Risk of bias of individual studies, meta-analysis, and additional analyses such as assessment of publication bias and sensitivity analysis were planned to be performed should an adequate number of original clinical studies be identified.
Results
Study Selection
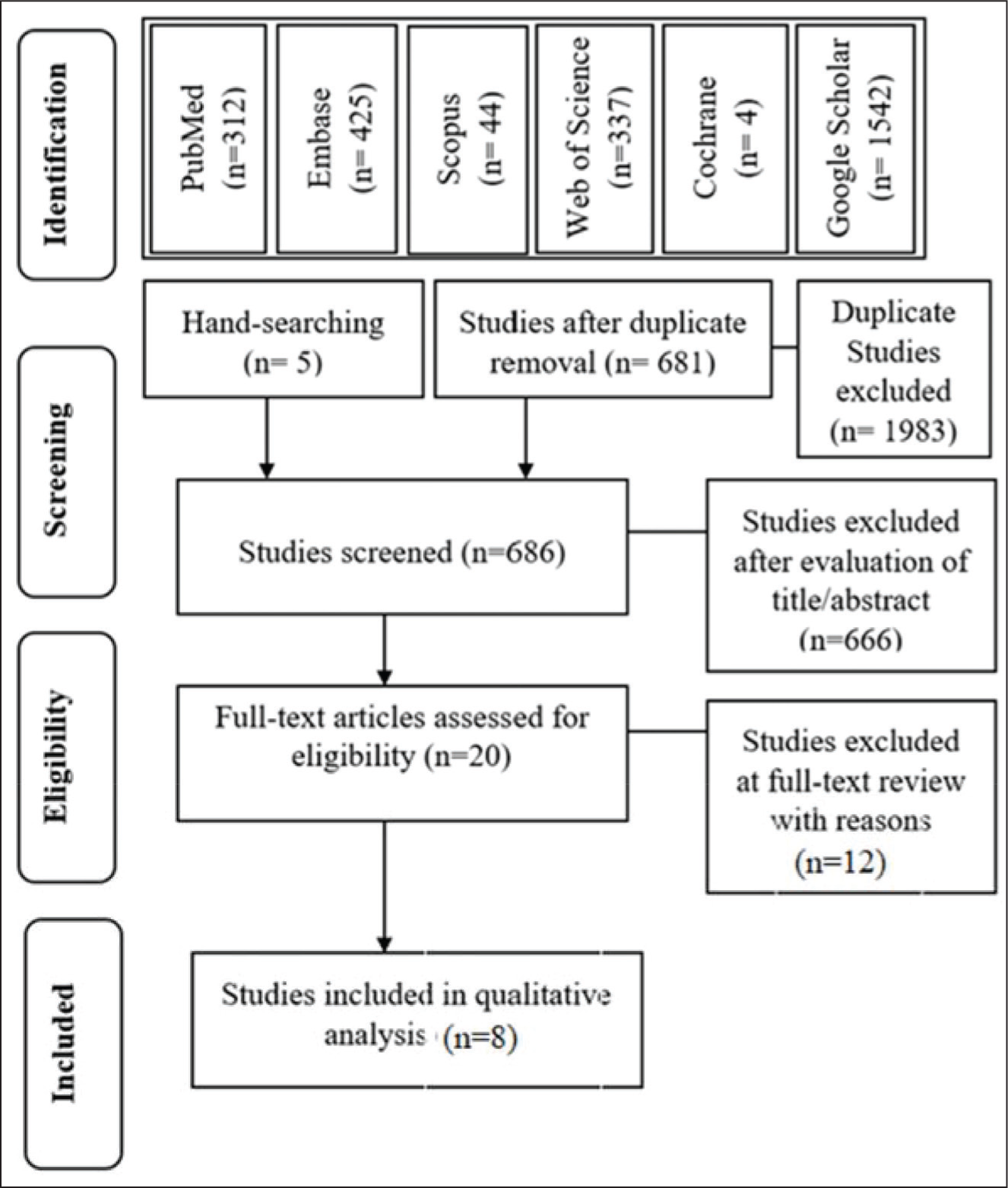
Initially, 2,664 studies were identified, and 1983 studies were excluded due to duplicate removal. A total of 681 studies remained. Five articles were added for screening after a hand search of the references of relevant articles. After title and abstract screening, the full texts of 20 articles were evaluated, and 12 were excluded based on the eligibility criteria (Appendix A). Eight studies9,11–14,17–19 were included in this review; and analyzed for data extraction (Figure 1).
Study Flowchart Based on the PRISMA Guidelines.
General Characteristics of the Included Studies
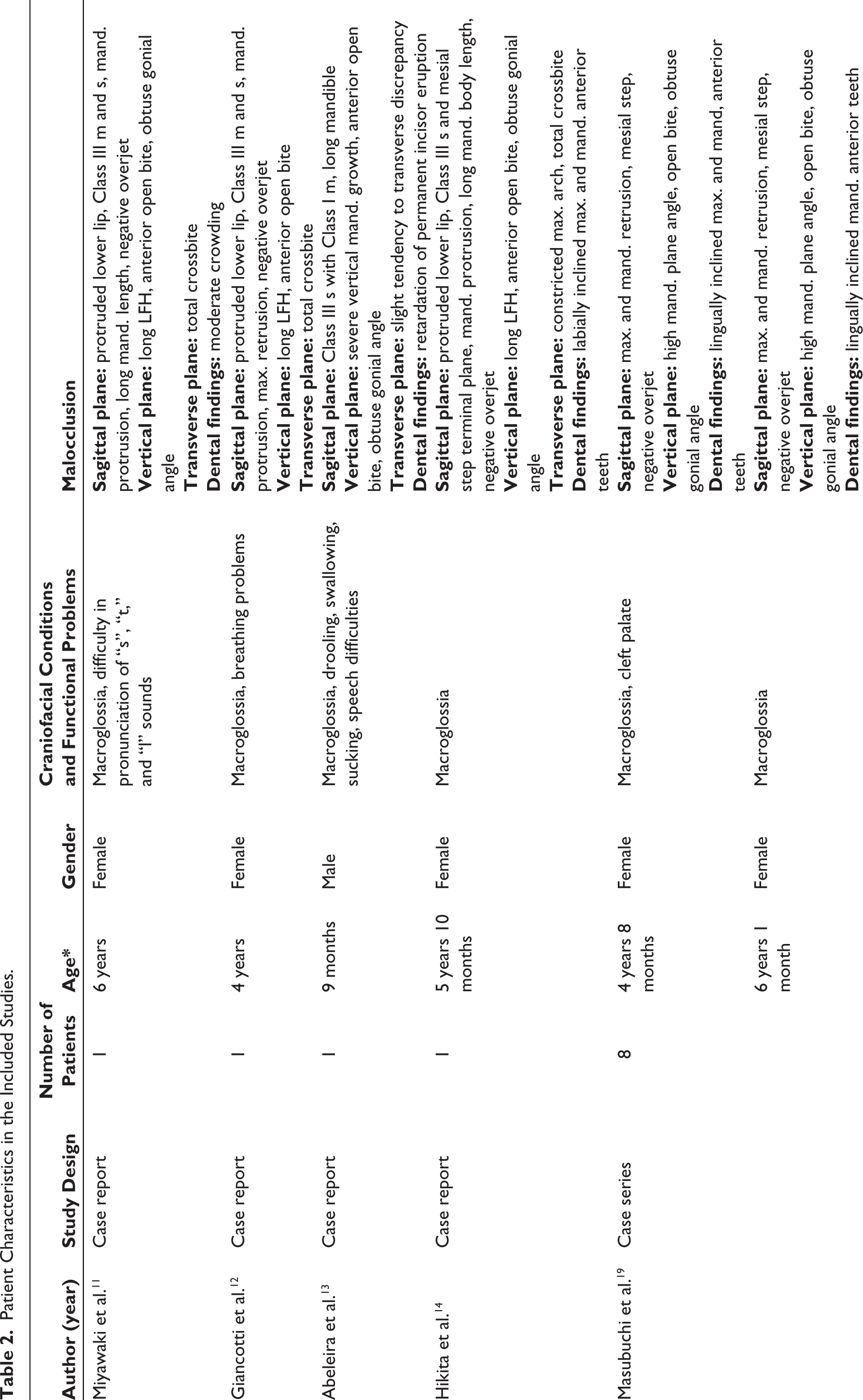
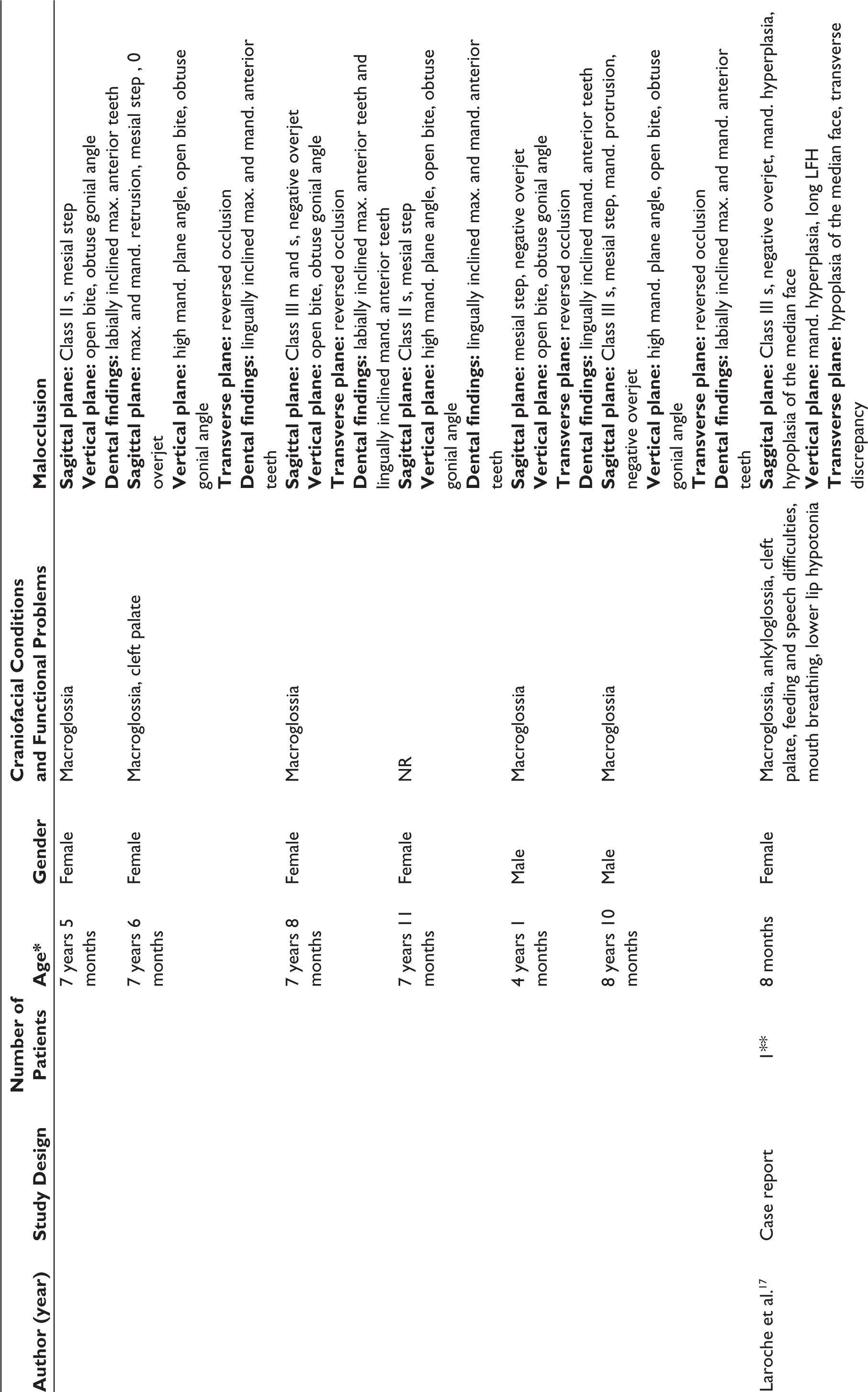
Five of the studies11–14,17 included in this review were case reports, one was a case series, 19 and two9,18 were retrospective clinical studies. A total of 35 patients with BWS were included in this review.9,11–14,17–19 The age of the patients at the initial oral evaluation ranged from 8 months to 8 years 10 months,11–14,17,19 and it was not reported in the two clinical studies.9,18 Both female and male patients were described9,11–14,17–19 (Table 2).
Orofacial Characteristics of Patients with BWS in the Included Studies
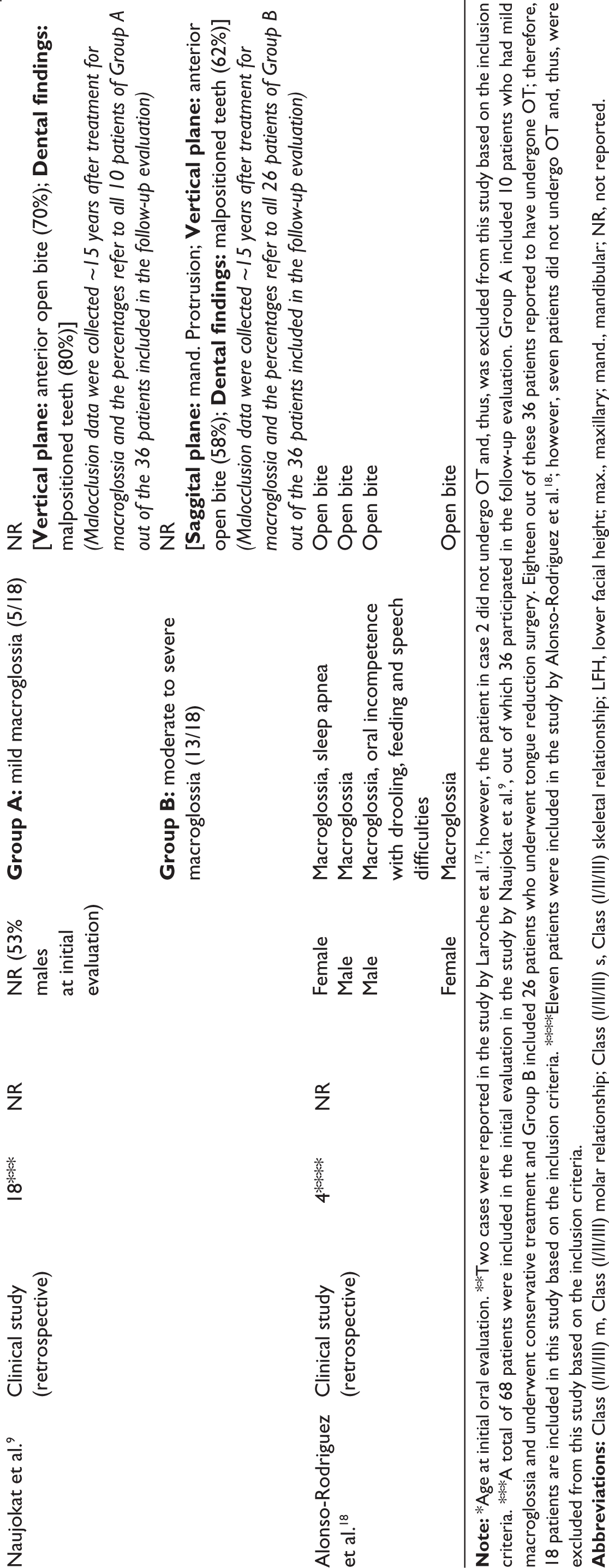
Macroglossia was present in all patients9,11–14,17–19 except for one, where the presence or absence of macroglossia was not reported; 19 and one patient also presented with ankyloglossia. 17 Speech difficulties were reported in four patients,11,13,17,18 breathing problems were reported in three patients,12,17,18 and oral incompetence was found in three patients.13,17,18 Oral function difficulties were not reported in two studies.14,19 Three patients had a cleft palate.17,19 Regarding the malocclusion characteristics of the patients, in the sagittal plane, three patients had a protrusive lower lip,11,12,14 six patients had a Class III skeletal and dental relationship,11,12,14,17,19 one patient had a Class III skeletal with Class I molar relationship, 13 four patients had a mesial step 19 and two patients had a Class II skeletal relationship with a mesial step. 19 Mandibular protrusion was reported in five patients,11,12,14,17,19 mandibular and maxillary retrusion was reported in three other patients, 19 and solely maxillary retrusion in one patient. 12 A long mandible was reported in four cases.11,13,14,17 Eight patients had a negative overjet,11,12,14,19 and one had zero overjet. 19 In the vertical plane, long lower face height was reported in four cases,11,12,14,17 and severe vertical mandibular growth was reported in the case by Abeleira et al. 13 Masubuchi et al. 19 reported high mandibular plane angle in five of their patients. Laroche et al. 17 reported mandibular hyperplasia in combination with hypoplasia of the median face in their patient. Sixteen patients had an anterior open bite and 11 patients had an obtuse gonial angle.11–14,19 In the transverse plane, some form of transverse abnormality was found in a total of nine patients.11–14,17,19 As for the dental issues of the patients, moderate crowding was reported in one case 11 and retardation of permanent incisor eruption in another. 13 The inclination of anterior teeth was reported as labial in four patients14,19 and lingual in six patients 19 (Table 2).
Patient Characteristics in the Included Studies.
Orthodontic Treatment-related Characteristics
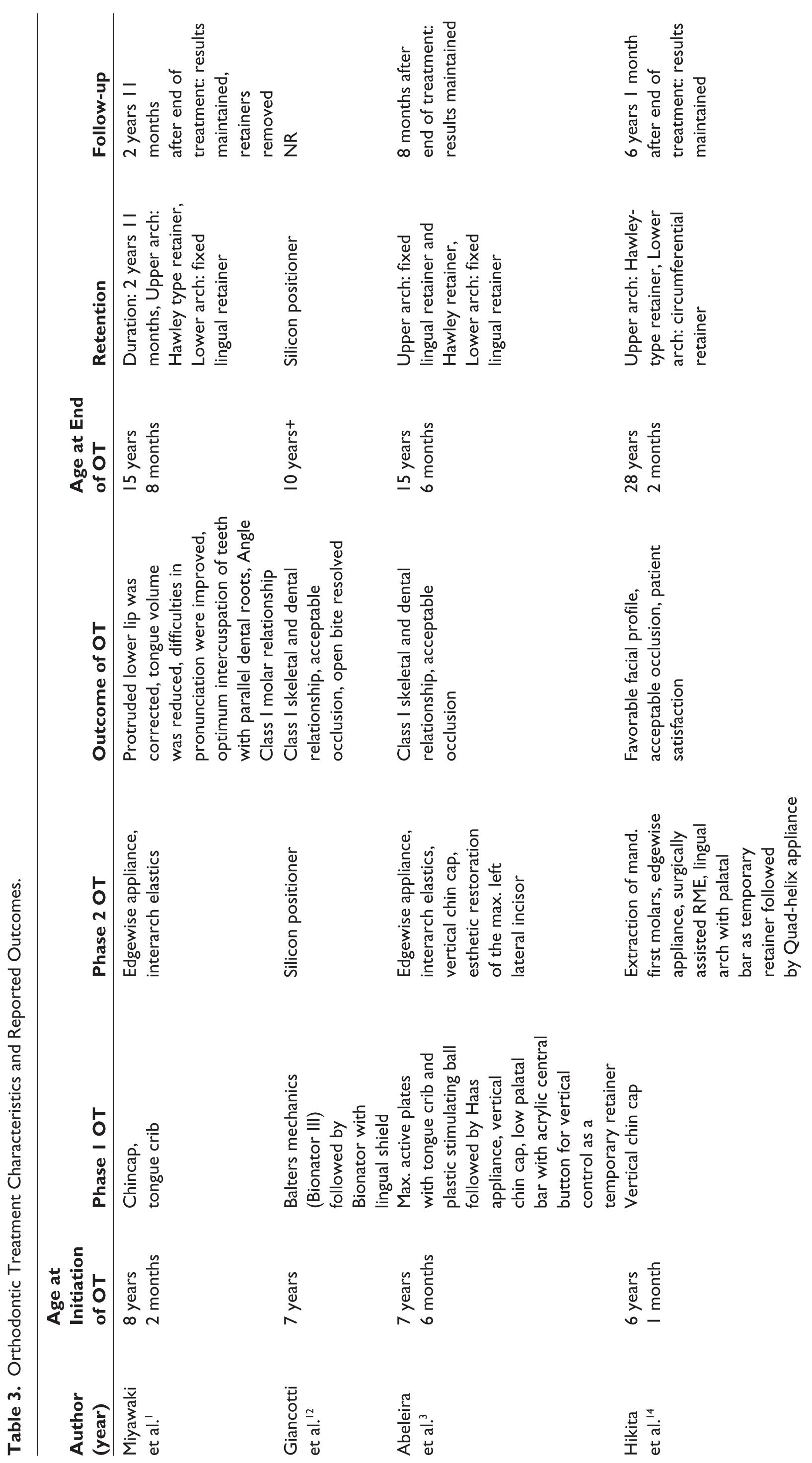
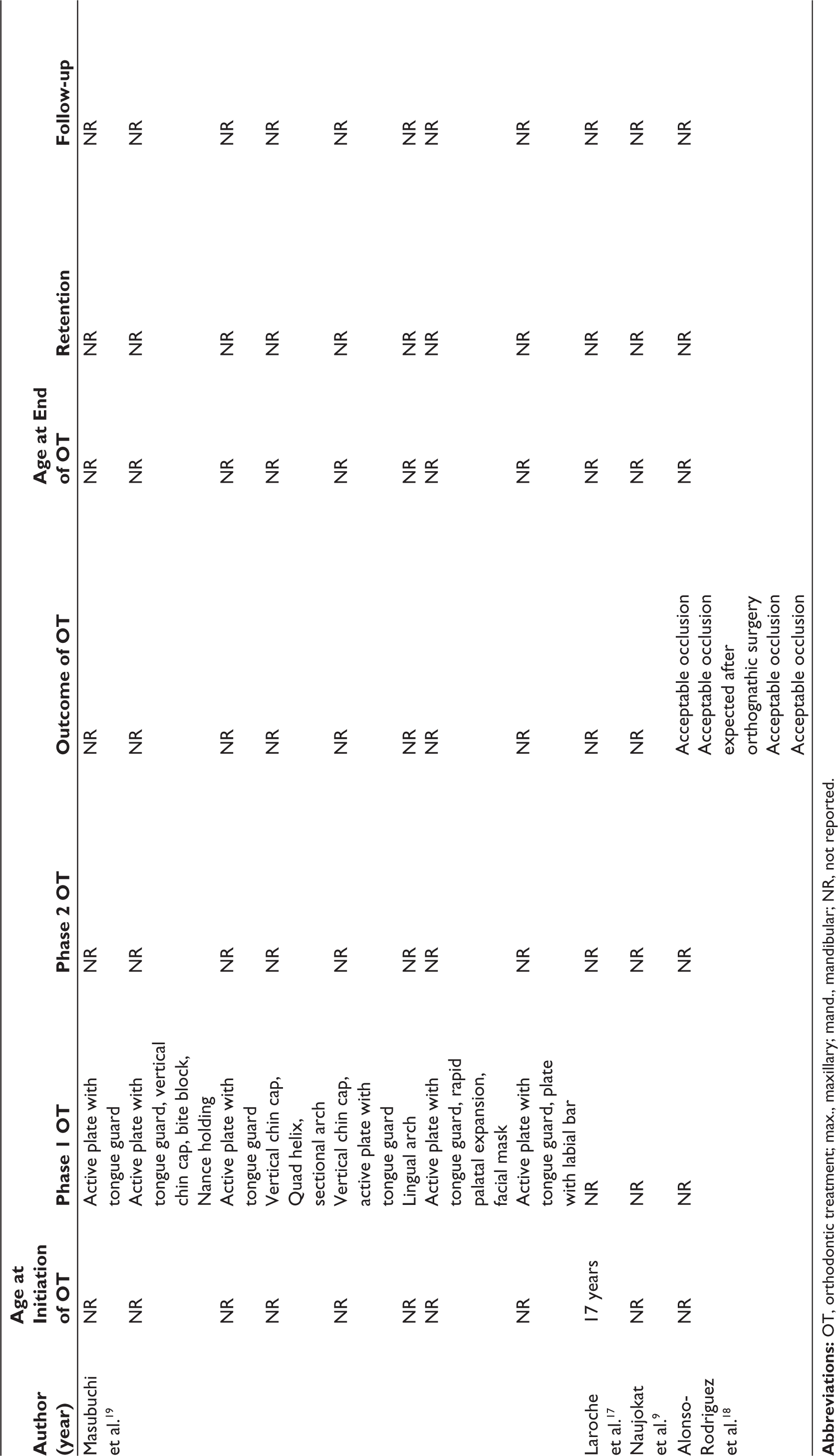
The age of the patients at the initiation of the OT ranged from 6 years 1 month to 17 years,11–14,17 and was not reported in three studies.9,18,19 The chin cap was used by six patients;11,13,14,19 a tongue guard was used by eight patients11,13,19 incorporated in an active plate in seven of them.13,19 Giancotti et al. 12 reported the use of two forms of the Bionator. The use of the Haas appliance, 13 a bite block, 19 the Nance holding appliance, 19 the Quad helix,14,19 a sectional arch, 19 a lingual arch, 19 rapid palatal expansion, 19 and a facial mask 19 were also reported. A low palatal bar with an acrylic central button for vertical control 13 and a lingual arch with a palatal bar 14 were worn by two patients as temporary retainers. Two-phase OT was performed in four studies and included Edgewise appliances,11,13,14 interarch elastics,11,13 and a silicon positioner. 12 Esthetic restoration of the maxillary left lateral incisor 13 and extraction of the mandibular first molars 14 were needed in two cases. Three studies9,17,18 did not report the particular features of the OT (Table 3).
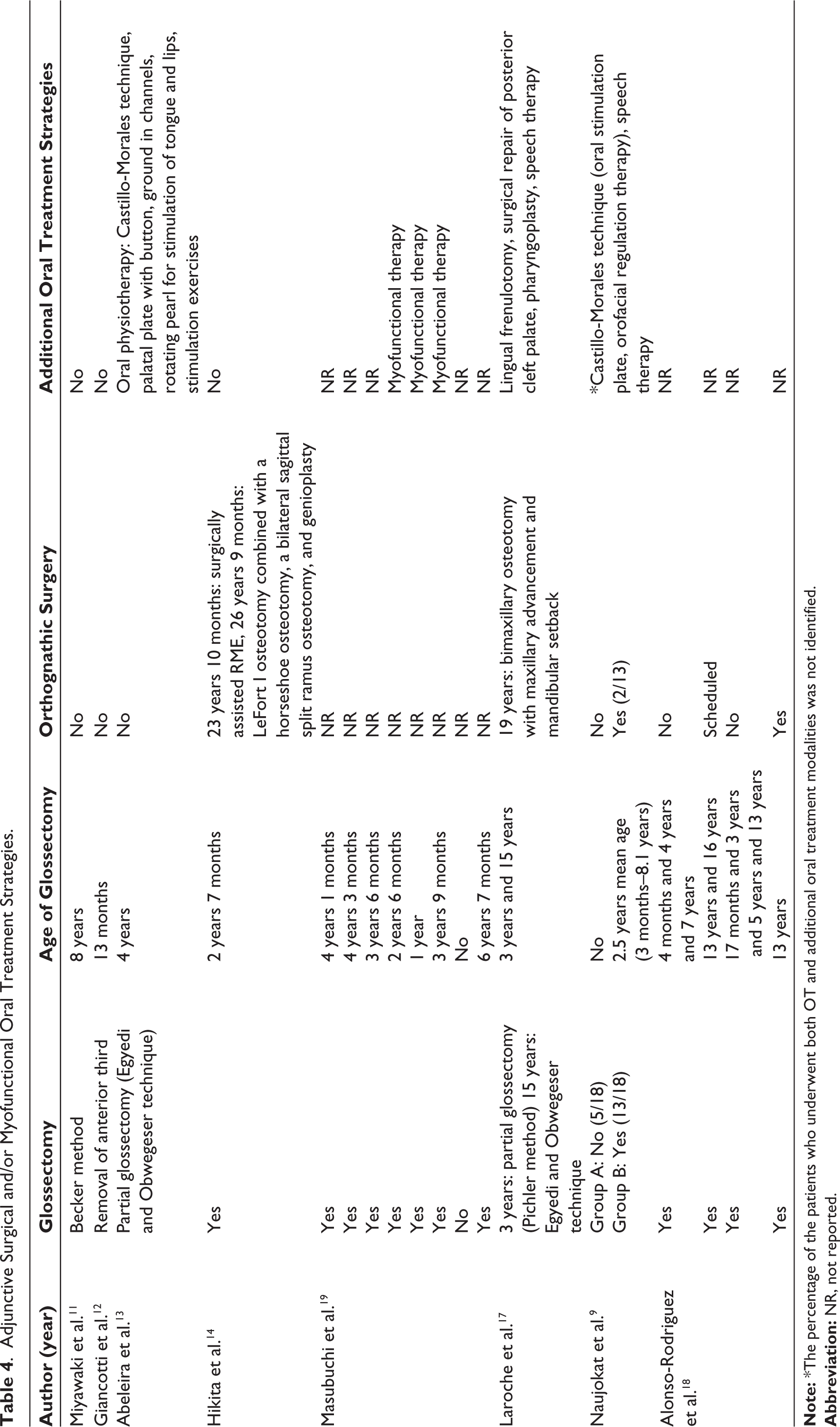
Adjunctive Oral Myofunctional and Surgical Treatment Strategies
Glossectomy was performed in 29 patients,9,11–14,17–19 at a large variety of ages, starting from 3 months and reaching up to 13 years for the primary surgery. Four patients had to undergo a second17,18 or third 18 glossectomy. The patient in the study by Laroche et al. 17 , who also presented with ankyloglossia and cleft palate, received surgical treatments for these conditions as well. Myofunctional therapy and oral physiotherapy were reported in 3 and 14 patients, respectively.9,13,19 Speech therapy was also performed in the majority of patients in the study by Naujokat et al., 9 and in the case by Laroche et al., 17 orthognathic surgery was performed in five patients with BWS9,14,17,18 (Table 4).
Orthodontic Treatment-related Outcomes
The age of the patients at the end of the OT ranged between 10 and 28 years,11–14 and was not reported in four studies.9,17–19 The outcome of the OT was reported as successful in five studies.12–14,18 Two studies reported improvement in oral function and patient satisfaction after OT.11,14 A Hawley-type retainer was used for retention in the upper arch in three studies,11,13,14 in combination with a fixed lingual retainer in one study. 13 In the lower arch, two studies reported the use of a fixed lingual retainer,11,13 and one study indicated the use of a circumferential retainer. 14 Giancotti et al. 12 used a silicon positioner for retention. The follow-up, as reported by three studies, ranged from 8 months to 6 years, and the results of the OT were maintained.11,13,14 Three studies9,17,19 did not report the outcome of OT nor the retention method. Follow-up after the end of treatment was not reported in four studies9,17–19 (Table 3).
Orthodontic Treatment Characteristics and Reported Outcomes.
Adjunctive Surgical and/or Myofunctional Oral Treatment Strategies.
Risk of Bias of Individual Studies and Additional Analyses
Publication bias and selective reporting of outcomes within the studies, such as selective reporting of patients with extreme manifestations of BWS or underreporting of moderate aspects of the malocclusion or OT, could introduce bias or distort the representation of the true clinical picture. In light of the available evidence, which encompassed a total of six case reports/case series and two retrospective clinical studies, which did not report the specific features of the OT protocol, the risk of bias of included studies is considered high. Moreover, owing to the unavailability of comprehensive data and the absence of key information necessary for meaningful quantitative synthesis, a meta-analysis, sensitivity analysis, and evaluation of publication bias were deemed unfeasible and, as such, were not conducted.
Discussion
An exhaustive search of the literature was conducted to identify studies that reported the OM of patients with BWS. We aimed to summarize and critically appraise information regarding common malocclusion traits, dentoskeletal and functional discrepancies in patients with BWS, OT strategies, and related outcomes, as well as identify adjunctive interdisciplinary surgical and/or myofunctional treatment protocols. A total of 35 patients with BWS were included in this review and 34 of them presented with macroglossia, whereas, for one patient, the presence or absence of macroglossia was not clearly stated.9,11–14,17–19 The most common malocclusion traits identified were Class III relationship, either dental or skeletal, decreased overjet, increased vertical growth, and transverse discrepancies.9,11–14,17,19 An anterior open bite was reported in 16 patients.11–14,18,19 However, the actual number of patients who presented with anterior open bite is greater, since Naujokat et al. 9 reported anterior open bite (along with other malocclusion features) in a large percentage of their patients, but it was not specified which of them the ones that received OT were. Similarly, an obtuse gonial angle was reported in 11 out of the 35 included patients,11,13,14,19 but this is also likely to be an underestimation, as the study by Alonso-Rodriguez et al. 18 focused mainly on the presence of open bite and other aspects of malocclusion were not reported. Other studies have also reported a high rate of proclination of the incisors, interdental spacing, and wide dental arches in patients with BWS;10,20–22 as well as the presence of anterior open bite.10,21 However, despite the common aforementioned malocclusion traits, patients with BWS do not present with a consistent maxillofacial pattern. Patients with BWS may present with a variety of dentoskeletal findings, including retrusive jaws, Class I or Class II relationship, dental crowding, and retroclination of incisors11,19,23 indicating the need for individualized treatment strategies.
The etiology behind the malocclusion in patients with BWS has been a subject of debate in the literature. Naujokat et al. 9 reported mandibular prognathism solely in the group of patients who presented with moderate to severe macroglossia and were in need of glossectomy. 9 Macroglossia is highly associated with the presence of open bite, Class III malocclusion, mandibular prognathism, obtuse gonial angle, spacing, increased dental arch width, and protrusion of incisors.8,24 These dentoskeletal features can be attributed to macroglossia according to the functional matrix theory.7,8 However, when it comes to BWS, this might not necessarily be the full story. Some authors have suggested the possibility that mandibular overgrowth may be an intrinsic characteristic of the syndrome.9,22 Defabianis et al., 23 in a study of 25 Caucasian patients with BWS, found several possible correlations between malocclusion and genetic subtype, and although these results did not reach statistical significance, they reported that the IC2-LoM subtype seems to be related to a worse skeletal growth tendency with greater risk for progressive deterioration of the malocclusion. Regardless of the etiology, patients with BWS present with maxillofacial discrepancies and are highly in need of OT.10,23 All eight of the included studies in this review reported masticatory and/or speech difficulties in patients with BWS difficulties.9,11–14,17–19 This highlights the importance of OM in conjunction with adjunctive therapeutic procedures such as glossectomy and myofunctional therapy to improve oral function in patients with BWS. Naujokat et al. 9 reported high percentages of patient satisfaction regarding tongue shape and pronunciation, following either surgical or conservative treatment for macroglossia; nevertheless, phonation and lip closure difficulties, as well as malocclusion, persisted in a large portion of the patients. 9 Defabianis et al. 25 studied the oral health-related quality of life (OHRQoL) in patients with BWS and found that the oral function, orofacial appearance, and psychosocial impact indexes were significantly worse in patients with BWS compared with the control group (patients without BWS). Additionally, a significant percentage of patients with BWS who had been treated with glossectomy still had speech difficulties and open bite after treatment. 25
Even though there is a high need for OT in patients with BWS, there is poor-quality evidence regarding the recommended OT protocols and related outcomes. The chin cap and a maxillary active plate with a tongue guard were the most common OT options in the included studies, and four of them reported two-phase OT.11–14,19 However, a variety of appliances and methods were reported.11–14,19 Some form of retention was employed in four of the included studies.11–14 Hikita et al. 14 expressed a concern regarding the efficiency of phase 1 treatment, and the interval between initiation of OT and achieving final results ranged from 3 to 22 years in the four studies that it was reported.11–14,19 Reports regarding long-term follow-up and stability of the OT in patients with BWS are scarce. Yet, the concurrence of macroglossia and open bite puts patients with BWS at high risk of instability of OT results. 8 Five of the included studies that reported the outcome of OT found it successful, and improvement in patient satisfaction and oral function after OT was reported in three studies.11–14,18 However, there are limitations in the interpretation of these results as no specific indices were used for the measurement of the success of OT. Based on these findings, it is challenging to identify the optimal OT and retention protocols in patients with BWS. Nonetheless, OT appears to be a useful option for growing patients with BWS to improve dentoskeletal discrepancies and OHRQoL. Concomitantly, children with syndromes and/or developmental disorders often have insufficient access to dental and orthodontic care due to various reasons such as increased chairside time, lack of referrals, problems in cooperation, and lack of additional treatment strategies. 26 In this regard, development and implementation of educational initiatives especially at the dental school, pediatric dentistry, and orthodontic residency levels are needed to properly train practitioners in the management of children with syndromes such as BWS.
Interdisciplinary monitoring is imperative for patients with BWS. Adjunctive treatments such as speech therapy, oral physiotherapy, and orthognathic surgery have been reported in the literature with possible beneficial effects.9,11–14,17–19 The combination of OT and myofunctional therapy has demonstrated beneficial outcomes in the development of orofacial characteristics in previous studies.27,28 Regarding orthognathic surgery, it has been successfully used to improve severe skeletal discrepancies; nevertheless, the potential advantages should always be weighed against possible complications and patient discomfort.29,30 The efficacy of tongue reduction surgery in improving maxillofacial morphology and quality of life in patients with BWS is a subject of controversy. Many authors advocate for glossectomy at a young age to prevent the adverse effects of macroglossia.9,18,24,31 Alonso-Rodriguez et al. 18 reported improvement of the open bite in five patients who received glossectomy at an early age. On the contrary, macroglossia in this syndrome is due to muscle hyperplasia which, in contrast to other types, might continue to progress, rendering early glossectomy insufficient. 20 A total of nine patients in three of the included studies needed additional tongue reduction surgeries growing up.9,17,18 Defabianis et al. 25 reported that, for a significant percentage of patients with BWS, glossectomy did not lead to a better quality of life. Additionally, Meazzini et al., 22 in a retrospective observational study, found no statistically significant difference in mandibular growth between patients with BWS treated and not treated with glossectomy. It seems that it would be valuable if it could be determined which patients with BWS would benefit from tongue reduction surgery and at what age. The right coordination of additional treatments may affect the success of OT, along with factors such as treatment duration and exhaustion of the patients’ and parents’ cooperation with the healthcare system.
To date, there are no studies in indexed literature that provide the optimal protocol for the OM of patients with BWS, including ideal treatment time, orthodontic mechanotherapy and appliances, and adjunctive procedures such as myofunctional therapy and glossectomy, with or without combined orthognathic surgery. This review is limited by the fact that the available evidence is either in the form of case reports11–14,17,19 or retrospective clinical studies that focused primarily on the treatments for macroglossia and did not thoroughly report the OT protocol. In this regard, it was difficult to adopt the traditional protocols followed in systematic reviews and meta-analysis. Therefore, the pattern of this review was customized to primarily summarize the available information. Future research is needed in the form of clinical studies to address the best treatment options for children with BWS, and a genetically targeted approach could prove advantageous.
Conclusion
Based on the limited available evidence, OT in conjunction with tongue reduction surgery and/or myofunctional therapy can be successfully performed in children with BWS to manage various dentoskeletal discrepancies and improve occlusion, oral function, and patient satisfaction. Clinical studies are needed to identify the optimal interdisciplinary OT protocols.
Footnotes
Authors Contributions
MK and DM conceived the ideas and led the writing. MK and LJ performed the literature search, study screening, selection, and data extraction. MK, FJ, and DM helped in the interpretation of the results. All authors revised the draft and approved it prior to submission.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Since this study is a review of the literature, ethical approval by an Institutional Review Board was not required.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed Consent
Not applicable.
Appendix
List of Excluded Studies at Full-text Review With Reasons for Exclusion.
| References | Reasons for the Exclusion |
| Giancotti et al. 12 PMID:12924739 | Duplicate study |
| Meazzini et al. 22 PMID: 33087311 | Focused question not addressed |
| Evans et al. 32 (2014) PMID: 24009317 | Editorial |
| Thomson et al. 33 (1986) PMID: 2941072 | Focused question not addressed |
| Kveim et al. 20 PMID: 3994256 | Focused question not addressed |
| Kawafuji et al. 10 PMID: 21457863 | Focused question not addressed |
| Wang et al. 34 (2003) PMID: 12627095 | Focused question not addressed |
| Wolford et al. 35 (1996) PMID: 8760843 | Focused question not addressed |
| Menard et al. 21 PMID: 7604127 | Focused question not addressed |
| Filippi et al. 36 (1970) PMID: 5426745 | Focused question not addressed |
| Manor et al. 37 (2020) PMID: 33194904 | Focused question not addressed |
| Komogashira et al. 38 (1984) PMID: 6597842 | Focused question not addressed |