
Abstract
Introduction:
Index for Orthodontic Treatment Need is a widely used index to assess the orthodontic treatment need among various populations.
Aim:
The aim of this study is to evaluate and compare orthodontic treatment needs of Nepali among gender and ethnicity.
Materials and Methods:
A total of 800 children (400 males and 400 females) above 14 years of age were selected from different schools of Kathmandu using multistage sampling technique. The study sample was grouped into 2 ethnic groups: Indo-Aryan and Janajati. Two trained and calibrated examiners examined school-going children using Index for Orthodontic Treatment Need tool. Statistical comparison of the study variables by gender and ethnicity was done.
Results:
Dental Health Component showed 36.75% male and 34.5% female, and 39% Indo-Aryan and 29.76% Janajati had great treatment need. The Aesthetic Component (AC) showed 13.75% male and 12.25% female, and 12.5% Indo-Aryan 14.58% Janajati had great/severe need.
Conclusions:
Males had great/severe need of treatment for both Dental Health Component and Aesthetic Component (AC). Indo-Aryan showed higher degree of great/severe need for Dental Health Component and lesser degree of great/severe need for Aesthetic Component (AC) than Janajati.
Introduction
A deviation from normal or ideal occlusion can cause various functional, aesthetics, and psychosocial problems. Malocclusion can tax an individual’s confidence in society. This problem therefore needs to be assessed and addressed. Accurate data is required for assessing the needs of orthodontic treatment among various populations. The principal goal of orthodontic treatment is to improve oral health, function, and aesthetics. Dominant motives for orthodontic treatment have evolved into improving dental-facial appearance and other psychosocial factors.1–3
In the past, various indices have been developed to assess the need of orthodontic treatment like Handicapping Labio-lingual Deviation Index, Swedish Medical Board Index, Dental Aesthetic Index, Index of Orthodontic Treatment Need, Index of Complexity, Outcome & Need, and so on.
Brook and Shaw 4 developed and tested the validity and reliability of the Index for Orthodontic Treatment Need as an index of treatment needs. The Index for Orthodontic Treatment Need attempts to rank malocclusion in terms of the significance of various occlusal traits for an individual’s dental health and perceived aesthetic impairment. 5 Index for Orthodontic Treatment Need comprises of 2 components—Dental Health Component and Aesthetic Component (AC). This index allows prioritization of treatment and appropriate direction of resources which helps in maximizing cost-benefit ratios to the advantage of both the patient and the service provider. Although the use of indexes has been limited in countries where publicly funded dental health services are not generally available. However, treatment need indexes are also important tools for recording the prevalence and severity of malocclusions in epidemiological studies. 6
Drive on determination of orthodontic treatment needs were carried out on the basis of Index for Orthodontic Treatment Need by different authors: Brook and Shaw, 4 Burden and Holmes, 7 Mandall et al, 8 Kok et al, 9 Holmes and Willmot, 10 and in different countries: England (Brook & Shaw 4 and Richmond et al 11 ), Norway (Birkeland et al 12 ), Switzerland (Firestone et al 13 ),Turkey (Uncuncu and Ertugay 14 ), Iran (Hedayati et al 15 ), and Pakistan (Zahid et al 16 ).
Physical beauty is subjective in nature. It depends on various factors like age, gender, ethnicity, socioeconomic background, and so on. Factors other than the severity of malocclusion, such as aesthetics, and the impact of the malocclusion on the subject’s quality of life must also be considered when assessing treatment need. Such factors are more subjective and less readily measured than the presence and severity of malocclusions and may be influenced by the subject’s cultural background and social status. 17 Several studies have investigated the relationship between normative orthodontic treatment need, measured by a clinician, and the more subjective patient perception of malocclusion and found that perceived orthodontic treatment need also varies among ethnic groups and gender.8, 18 Index for Orthodontic Treatment Need is one of the most essential areas of study in orthodontics in different countries. No studies on Index for Orthodontic Treatment Need based on gender and ethnicity have been done in Nepal so far. Hence, this study was proposed. The primary aim of this study is to evaluate the orthodontic treatment needs of Nepali. The secondary aim is to compare the orthodontic treatment needs of Nepali function of gender and ethnicity using Index for Orthodontic Treatment Need.
Materials and Methods
It is a cross-sectional descriptive study. The study population included adolescents of high school of Kathmandu Valley. Study sample was obtained using multistage sampling technique. The sample size for the study at 35% prevalence and 10% of allowable error was 715. The sample included in the study was 800 with equal number of male and female in each group of 400. In the first stage, all the schools with more than 100 students in the specified age group were selected; in the second stage, the samples were divided based on gender into male and female; and in the third stage, equal number of boys and girls were selected using random sampling technique. Sample size of 800 (400 males and 400 females) who met the inclusive criteria of the study was derived out of total screened population sample of 927.
Data Collection Method and Tools
Two trained and calibrated examiners performed oral examination. Before the survey, 10% of total students were examined by each of the 2 investigators to assess interexaminer reliability and Kappa values for both the examiners were found to be 0.87 and 0.88, respectively. Clinical examination was carried by examining each student with each examination lasting 10 min. The assessment of dental occlusion was carried out using latex gloves, dental mouth mirrors, and millimetric rulers. Sufficient numbers of autoclaved instruments were made available to avoid the interruption during the study. Data was coded and entered into Excel sheet. Rechecking and cross-checking was done during data entry phase to maintain the data quality followed by necessary data cleaning. Data was transformed into SPSS version 16.0. Primarily, univariate and bivariate analysis was done to measure the need for orthodontic treatment.
Exclusion Criteria
Subjects with craniofacial anomalies (clefts and syndromes), ongoing or previous history of orthodontic treatment, and non-Nepali citizens were excluded from the study.
Dental Health Component can be examined either clinically or on the study model. In the present study, dental stone study model was used to determine the Dental Health Component. Study models were examined and graded by the specialist to determine the Dental Health Component of the Index for Orthodontic Treatment Need. The grades of Dental Health Component are based on occlusal characteristics: overjet, overbite, crossbite, contact point displacement, missing teeth, and other occlusal abnormalities. Dental Health Component comprises of 5 grades: grade 1—no treatment need, grade 2—slight/little treatment need, grade 3—moderate/borderline treatment need, grade 4—great treatment need, and grade 5—very great treatment need.
AC consists of 10-grade standard reference color photographs representing different grades of dental attractiveness. Grade 1 represents the most attractive and grade 10 the least attractive dentitions. Intraoral frontal view color photographs of orthodontic patients were used in order to determine the AC of the index. The examiner assessed the patient’s photograph and compared it with the 10-grade reference photos and gave a score to each patient, which was considered as the subjective need of the patient.
Statistical Analysis
Data were coded and entered into Microsoft Excel sheet. To maintain the data quality (validity), rechecking and cross-checking were done during data entry phase. After the entry of the data into the Excel sheet, necessary data cleaning was done. Second, data were transformed into SPSS 16.0 version where further cleaning, coding, recoding, cross-checking, processing, and analysis were done. Descriptive statistical analysis was performed for both gender and ethnicity.
Results
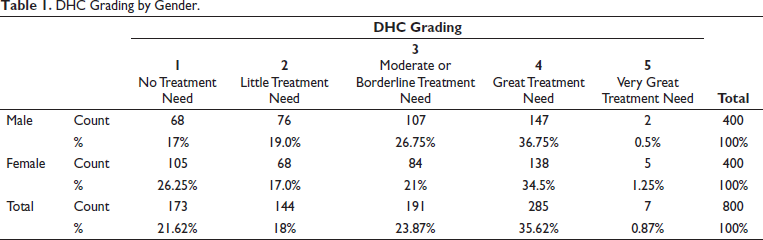
DHC Grading by Gender.
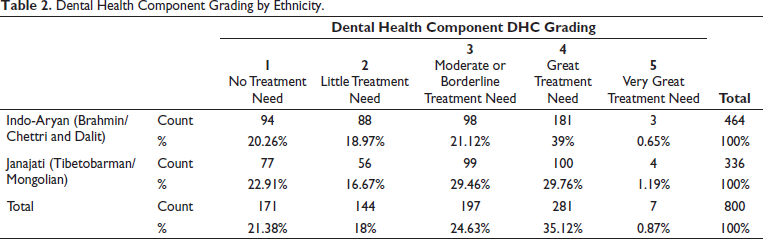
Dental Health Component Grading by Ethnicity.
Aesthetic Component by Gender.

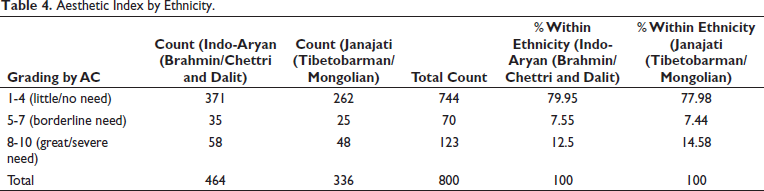
Aesthetic Index by Ethnicity.
Discussion
Dental Health Component of Index for Orthodontic Treatment Need is a valuable tool in determining the treatment need priority for effective resource use in orthodontic care. It is based on the view that the more a deviation differs from a given norm (the ideal occlusion), the greater are the risks of future objective functional deficits or oral health problems. In the Index for Orthodontic Treatment Need-Dental Health Component, only the most severe occlusal trait is considered for categorization, despite the fact that other severe symptoms may be present. Aesthetic Component of Index for Orthodontic Treatment Need, whether it is examiner or patient-based, assesses malocclusion on the grounds of aesthetic impairment, and by inference reflects the psycho-social need for orthodontic treatment. However, it has shortcomings like the other aesthetic orthodontic treatment need indices; the subjective nature of the aesthetic indices and the variable perception of attractiveness between clinicians and patients, and among various cultures or countries. The Index for Orthodontic Treatment Need has been shown to be reliable and have predictive validity, which is of particular importance when considering the young age groups studied here. 5 Taking into account the occlusal changes that occur with age, it has been shown that an Index for Orthodontic Treatment Need grade assigned at age 11 is unlikely to change by the age of 19. 19
A total of 23.87% (26.75% males and 21% females) people have borderline need of treatment and 35.62% (36.75% males and 34.5% females) have great/severe need of treatment for Aesthetic Component of Index for Orthodontic Treatment Need. Similar findings were found in the study by Puertes-Fernández et al 20 and Corneaga et al 21 In contrast, Miguel et al 22 found lower need for treatment in their sample. The males have higher need for orthodontic treatment than female for all grades except for little or no need (grade 1-4 AC) similar to other studies by Hedayati et al, 15 Moghadam et al, 23 Jeshi et al, 24 and Reshitaj et al 25 whereas Miguel et al 22 and Kolawole et al 26 found no gender difference.
This study reveals that majority of 79.5% (77.25% males and 81.75% females) people have (little/no need) (grade 1-4 AC). A total of 7.5% (9% males and 6% females) people have borderline need of treatment (grade 5-7) and 13% (13.78% males and 12.22% females) have great/severe need of treatment (grade 8-10). The males have higher need for orthodontic treatment than female for all grades except for little or no need (grade 1-4 AC) similar to other studies by Hedayati et al, 15 Moghadam et al, 23 and Jeshi et al 24 whereas Miguel et al 22 found no gender difference.
In this study, Dental Health Component grading by ethnicity reveals that 34.38% (39% Indo-Aryan and 29.76% Janajati) people had great treatment need (grade IV Dental Health Component). Those with no need of treatment were 21.58% (20.26% Indo-Aryan and 22.91% Janajati) (grade I Dental Health Component). Grade II (little treatment need) and grade III (Moderate or Borderline treatment need) constituted 17.82% and 23.06% (18.97% and 21.12% Indo-Aryan; 16.67 and 29.46% Janajati), respectively. Grade V (very great treatment need) comprised 0.92% (0.65% Indo-Aryan and 1.19% Janajati). In this study, AC grading by ethnicity reveals 78.97% (79.95% Indo-Aryan and 77.98% Janajati) have little/no need of treatment (grade 1-4 AC). A total of 7.49% (7.55% Indo-Aryan and 7.44% Janajati) of them have borderline treatment need (grade 5-7 AC) and 13.38% (12.5% Indo-Aryan and 14.58% Janajati) have great/severe need (grade 8-10). The finding of the study shows that the need for orthodontic treatment showed ethnic difference similar to studies by Soh et al, 27 Reichmuth et al, 28 Proffit et al, 29 Christopherson et al, 30 and Ahmed et al. 31 The studies by Alkhatib et al, 32 Kolawole et al, 26 Otuyemi et al, 33 Mandall et al, 8 Woon et al, 34 and Zamzuri et al 35 found no significant variation in the need for orthodontic treatment between different ethnic backgrounds.
The reported differences in normative orthodontic treatment need may be due to the different methods used and differences among the age groups studied. In addition, some studies included samples with a history of orthodontic treatment and referred for orthodontic treatment.
The present study has also found high discrepancy in treatment needs between the Dental Health Component and Aesthetic Component of Index for Orthodontic Treatment Need. The discrepancy may be attributed to the fact that malocclusion traits (like missing teeth, crossbites, deep traumatic overbites, nonerupted, or impacted teeth has definite need for orthodontic treatment) have dental health implications, but do not attract a high AC score. In addition, as AC is subjective in its nature and assesses the aesthetic aspects of the malocclusion only in frontal view, it brings difficulties in assessing some parameters, such as degrees of Overjet and Overbite. 35 Hence, these indices show different aspects of orthodontic treatment need, both of which can be used to complement each other in epidemiologic surveys, diagnostic, and treatment procedures.
Conclusion
The Index for Orthodontic Treatment Need based on the Dental Health Component scores showed that approximately 60% were in need for orthodontic treatment when the subjects with the borderline or great need for treatment were summed up. Great and very great treatment need for orthodontic treatment need according to Dental Health Component was observed in 36.24% of the total sample. Dental Health Component grading by ethnicity reveals that 39% Indo-Aryan and 29.76% Janajati had great treatment need. Females have great/severe need of treatment for both Dental Health Component and AC components of Index for Orthodontic Treatment Need than males. Indo-Aryan showed lesser degree of great/severe need than Janajati.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance was obtained from the Ethical Review Board of Institute of Medicine (Reference: 288/[6-11]E2 078/079).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Each study participant was informed about the objective and benefit of the study. The informed consent form was signed to ensure consent from each participant.