
Abstract
Aim:
Endodontically treated teeth display altered tooth structure pertaining to various chemical irrigants and intracanal medicaments. To prevent the compromised adhesive bond, dentin biomodification is indicated. This study was designed to evaluate the influence of dentin biomodification on the fracture resistance of root canal-treated teeth following Delayed Endodontic Sealing (DES).
Materials and Methods:
In 50 maxillary central incisors, Class III cavities along with access cavities were prepared. The samples were randomly divided into five groups. Group 1: Intact teeth (N = 10), Group 2: Immediate Endodontic Sealing (IES) (N = 10); Group 3: DES after irrigation with 3% NaOCl (N = 10); Group 4: DES with 2% chlorhexidine (CHX) as a biomodifier (N = 10) and Group 5: DES with 5% grape seed extract (GSE) as a biomodifier (N = 10). In Group 2 samples, composite restorations were done prior to irrigation with 3% sodium hypochlorite (NaOCl). Group 3 samples received root canal irrigation with 3% NaOCl for 1 min, etch and rinse procedure and composite restorations. In Groups 4 and 5, dentin biomodification was done prior to composite restorations. Teeth were subjected to fracture resistance tests. Statistical analysis was carried out employing analysis of variance (ANOVA) and Tukey’s post hoc tests (p < .05).
Results:
IES group demonstrated the highest fracture resistance, with a significant difference statistically (p < .05) when compared with the DES groups. DES modified with GSE resulted in significantly superior fracture resistance compared to DES only, but no statistical difference was present between the CHX and grape seed-treated DES groups.
Conclusion:
DES with the use of dentin biomodifiers such as 5% GSE and 2% CHX increased the fracture resistance of root canal-treated teeth compared to DES only.
Keywords
Abbreviations
Delayed endodontic sealing
Immediate endodontic sealing
Chlorhexidine
Grape seed extract
Matrix metalloproteinases
Proanthocyanidins
Introduction
Fracture resistance of root canal-treated teeth is related to the amount of remaining tooth structure as well as the quality of the post-endodontic restoration. Most endodontically treated teeth end up in extraction not because of reinfection but because of restorative failure. 1 Endodontically treated teeth require special considerations for the final restoration due to decreased or altered tooth structure pertaining to various chemical irrigants and intracanal medicaments.
Crowns are indicated on endodontically treated posterior teeth. In anterior teeth with minimal loss of tooth structure, only access restoration will be sufficient without the requirement of a full veneer crown. 2 In such a situation, coronal sealing may be affected due to an alteration in the composition of the dentin surface caused by the action of irrigants used in root canal procedures.
In conventional endodontic procedures, sodium hypochlorite (NaOCl) is used as the primary irrigating solution in clinical practice because of its bactericidal activity and its ability to dissolve pulpal tissue. 3 After irrigation, pre-endodontic access sealing will be done with composite resin restoration, which is referred to as delayed endodontic sealing (DES). DES exposes the dentin to NaOCl solution, which damages the collagen component due to its deproteinizing effect, leading to decreased resin-dentin bond quality.4,5
Immediate endodontic sealing (IES) refers to a recent restorative technique of access cavity sealing prior to endodontic irrigation. Literature has reported improved internal adaptation of composite resin to dentin with IES than with DES.
6
IES can be done in conditions of non-vital teeth where irrigation with NaOCl for dissolution of pulpal tissue may not be required in the initial stages. Whereas in the case of vital teeth, there will be a need for the dissolution of pulpal tissue, which makes the use of NaOCl a must because of its tissue dissolving capacity. If not, the blood can compromise the adhesive bond’s strength. In such conditions, the negative effect of NaOCl can be reduced by dentin biomodification using the following methods:
strengthening collagen using collagen crosslinkers and reducing matrix metalloproteinases (MMP) activity using MMP inhibitors.
Dentin biomodification can be used to regain the lost bond strength due to NaOCl. 4 Literature report has shown that NaOCl makes dentin less tough and more brittle, making it vulnerable to fracture. 7
Several strategies have been reported in the literature to improve longevity and decrease the degradation of the hybrid layer by using protease inhibitors, enzyme inhibitors, and collagen crosslinkers as primary agents. 8
Natural crosslinkers such as 5% proanthocyanidins (PA), which are present in grape seed extract (GSE), can increase the number of intermolecular and intramolecular collagen crosslinks. This in turn leads to collagen strengthening, providing fibrillar resistance against the degradation of collagen. 4 Whereas 2% chlorhexidine (CHX) is shown to inhibit MMPs, which are involved in the degeneration of unprotected collagen fibrils and decelerate the loss of resin–dentin bonds. 9 Use of CHX and GSE as irrigating solutions before the application of bonding agents can improve the lost bond strength after the use of NaOCl by preserving the hybrid layer.4,9
So, the present research was aimed at analyzing the effect of DES with CHX and GSE as biomodifiers after irrigation with NaOCl on the fracture strength of endodontically treated maxillary anteriors.
The null hypothesis states that DES with CHX and GSE as biomodifiers after irrigation with NaOCl will not increase the fracture strength of endodontically treated maxillary anteriors.
Materials and Methods
Ethical approval was obtained from the Institutional Ethical Committee (IEC/VDC/MDS15 ENDO 06).
The samples were collected with consent from the pool of extracted teeth from the Department of Oral and Maxillofacial Surgery.
Sample Size Estimation
The calculation of required samples was done taking into account the results of the pilot study using G Power software at 80% confidence and a p-value set at less than .05, which resulted in 50 samples.
Sample Preparation
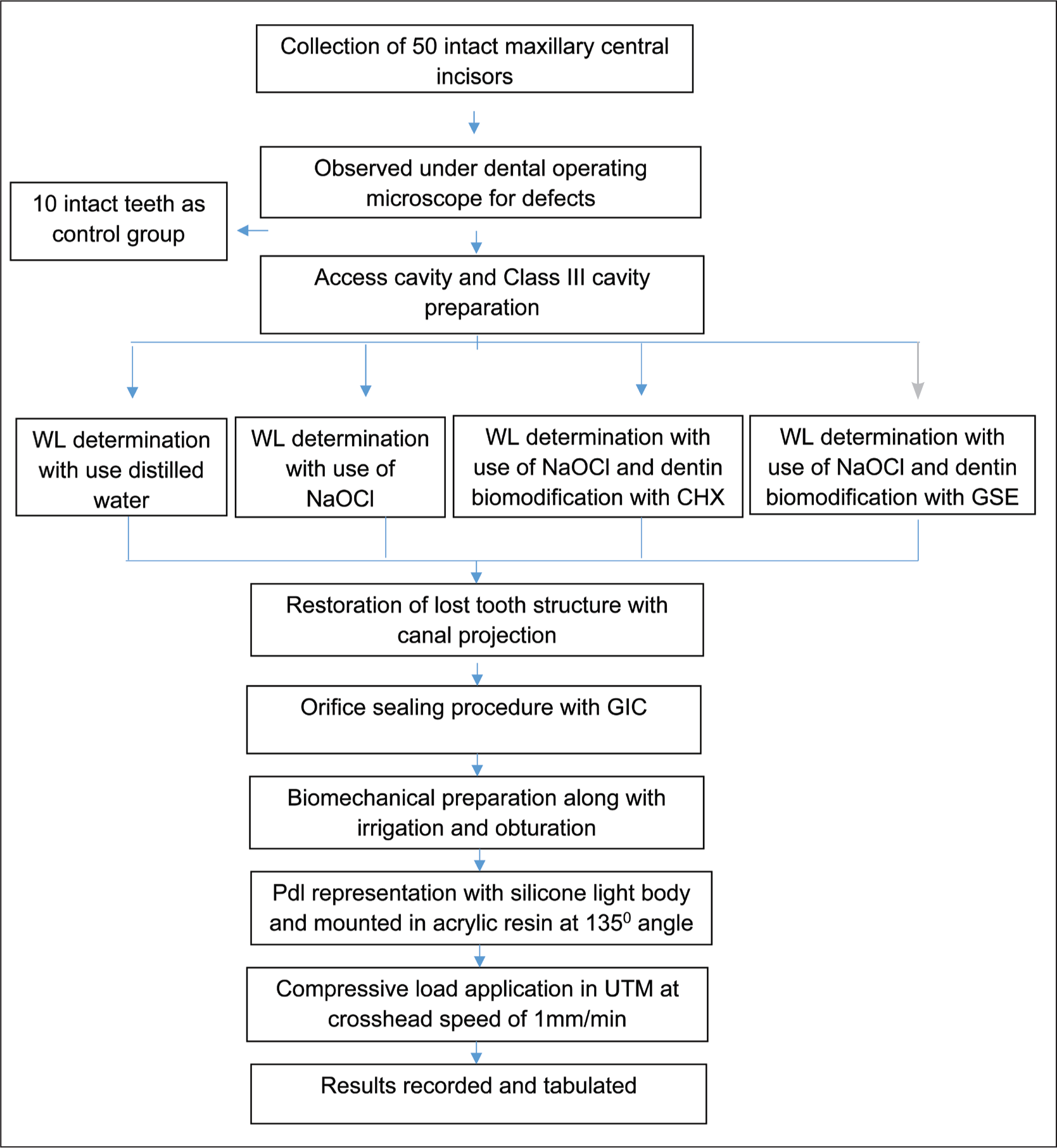
Maxillary central incisors of similar dimensions, that is, crown length 10 ± 1 mm and root length 13 ± 1 mm, were collected soon after extraction. Teeth indicated for extraction due to periodontal reasons were included. Teeth with caries, developmental defects, and cracks were excluded. Ten teeth were left uninstrumented (the control group). Endodontic cavity preparation was done with an endoaccess bur (Dentsply-Maillefer, Tulsa, OK, USA). Many patients report having profound Class III caries involving the pulp of their central incisor teeth, necessitating root canal therapy. Hence, a Class III cavity was prepared using a No. 2 round carbide bur (Mani Inc., Japan), extending 3 mm inciso-cervically and involving both buccal and palatal aspects of the tooth with an axial wall of 0.2 mm inside the DEJ to simulate the clinical scenario. (Figure 1a). Samples were randomly distributed by a simple randomization method using random numbers into four experimental groups.
Groups were divided as follows:
Group 1: Intact teeth (control group) (N = 10) Group 2: Immediate endodontic sealing (IES) (N = 10) Group 3: DES after irrigation of 3% NaOCl (N = 10) Group 4: DES with CHX (2%) as biomodifier (N = 10) Group 5: DES with GSE (5%) as biomodifier (N = 10).

Procedure for IES (Group 2)
The access cavity was irrigated with a sterile saline solution. The working length was determined using a 15k file. The Class III cavity was subjected to an etch and rinse protocol and blot dried, leaving optimally moist dentin.
Protaper gutta percha (GP) (Dentsply-Mallifer, USA) point inserted into the canal orifice to act as a canal projection blocking the canal orifice. The adhesive agent (Tetric N-Bond, Ivoclarvivadent, Austria) was coated on cavity walls and polymerized as per the manufacturer’s instructions. Class III cavity was restored with nanohybrid composite resin (Tetric N-ceram, Ivoclarvivadent, Austria) by layering technique with increments of 2 mm thickness, and the GP used for canal projection was removed.
Procedure for DES
Root canals were irrigated with 3% NaOCl (Prime Dental Pvt. Ltd., India) solution for 1 min and flushed with sterile saline solution. The canal projection protocol was carried out as in the IES group.
Procedure for DES with Biomodification
After root canal irrigation with 3% NaOCl for 1 min, the etch and rinse procedure was done. In Group 4, dentin was dried, and 2% CHX (V-concept, Vishal Dentocare, Pvt. Ltd., India) was applied as a dentin biomodifier using an applicator tip for 60 s, gently blot dried and continued with canal projection (Figure 1b).
Five grams of GSE in the form of powder (Puritans Pride Inc., Oakdale, NY, USA) were collected from the capsules and dissolved in 100 ml of sterile distilled water to make a 5% GSE solution. In Group 5, dentin was dried and 5% GSE was applied as dentin biomodifier with a syringe for 10 min, rinsed with saline, blot dried, and continued with canal projection by following the bonding protocol for composite buildup (Figure 1c).
Canal Preparation, Obturation, and Postendodontic Restoration Protocol
Samples were prepared with the Protaper Universal File System (Protaper Universal, Dentsply-Maillefer) to an apical size of F5 using ethylenediaminetetraacetic acid (EDTA; Prime Dental Pvt. Ltd., India) as a lubricant. Obturation was done using GP master cone (F5, Dentsply-maillefer) and AH plus (Dentsply-maillefer) sealers with cold lateral compaction technique. Orifice sealing was done using glass ionomer cement (GC, USA). Etch-and-rinse and bonding protocols were carried out. The access cavity was restored with nanohybrid composite (Tetric N Ceram, Ivoclar Vivadent) in layers of 2 mm using a suitable instrument and polymerized each layer for 10-15 sec according to the instructions given by the manufacturer; finishing and polishing were done. The prepared specimens were then stored in saline solution for 2 days to complete the setting of the sealer. Teeth were subjected to 500 cycles of artificial thermal aging according to the ISO 11405 standard recommendations.
Fracture Testing
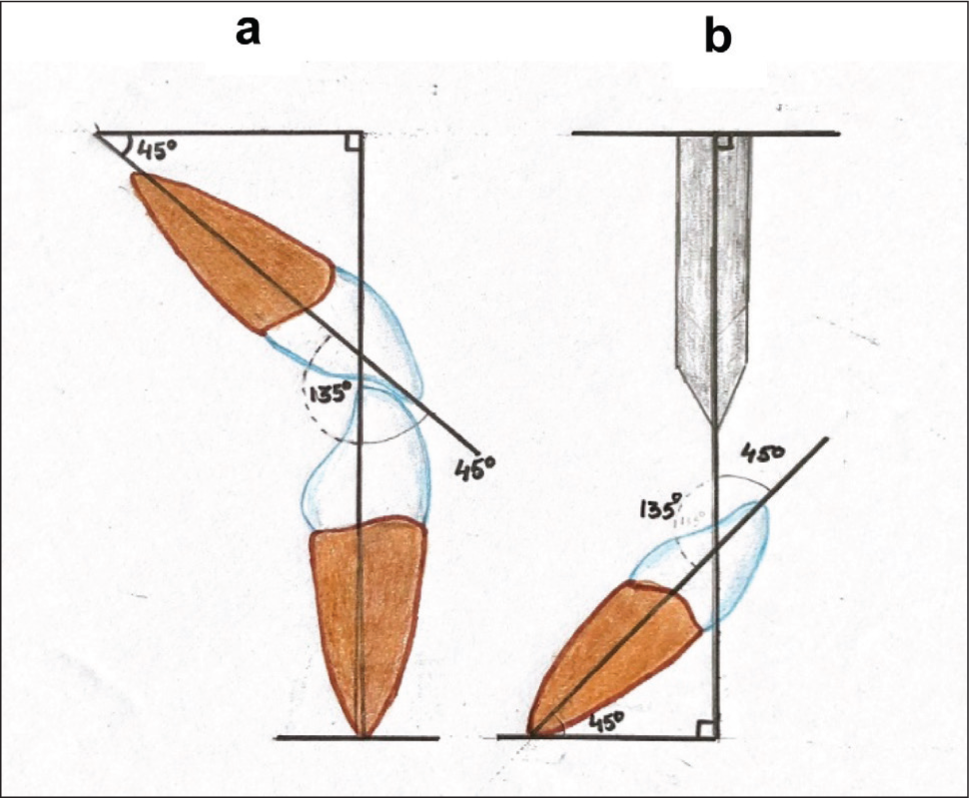
Following the endodontic procedure, a nick was placed in the middle of the mesiodistal width, 3 mm apical to the incisal edge. The periodontium around the tooth was simulated with silicone impression material of 0.1 mm thickness. Specimens were mounted in polymethyl methacrylate (PMMA) resin such that the long axis of the tooth was oriented at an angle of 135° to the applied force (Figure 2).
Methodology Flowchart
Schematic Representation of Applied Load. (a) Anterior Occlusion and (b) Angle of Load Applied in the Present Study.
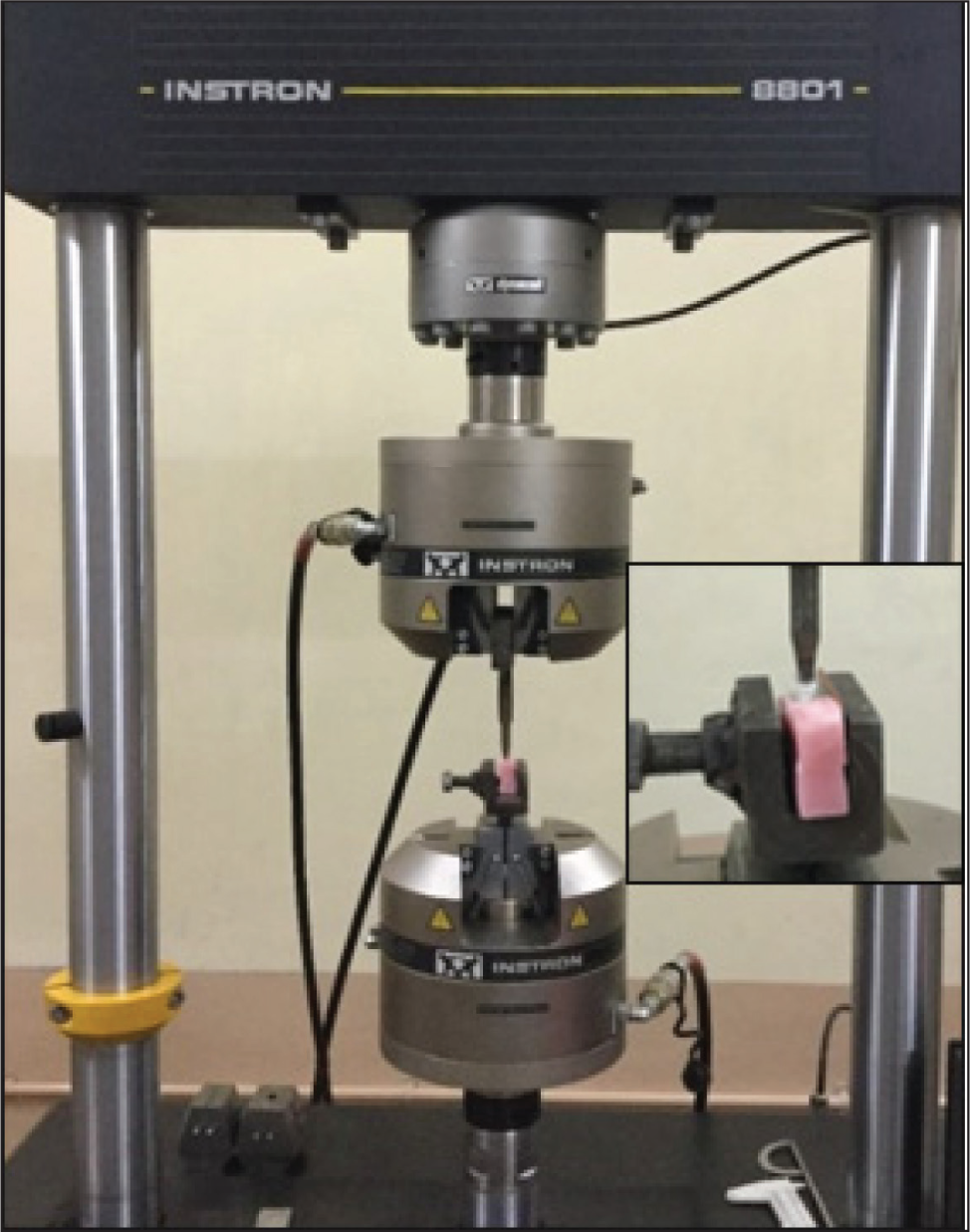
Teeth were mounted on a universal testing machine (Instron), and compressive force was applied at a crosshead speed of 1 mm/min until fracture occurred (Figure 3). The fracture loads were recorded in Newtons. 10 Fractured specimens were evaluated for the nature of fractures under a dental operating microscope at 1× magnification (Labomed, Los Angeles, CA, U.S.A). Fracture modes were categorized as restorable and unrestorable. Restorable fracture: fracture above the CEJ or within 1 mm apical to the CEJ. Unrestorable fracture: fracture more than 1 mm apical to the CEJ. 11
Results
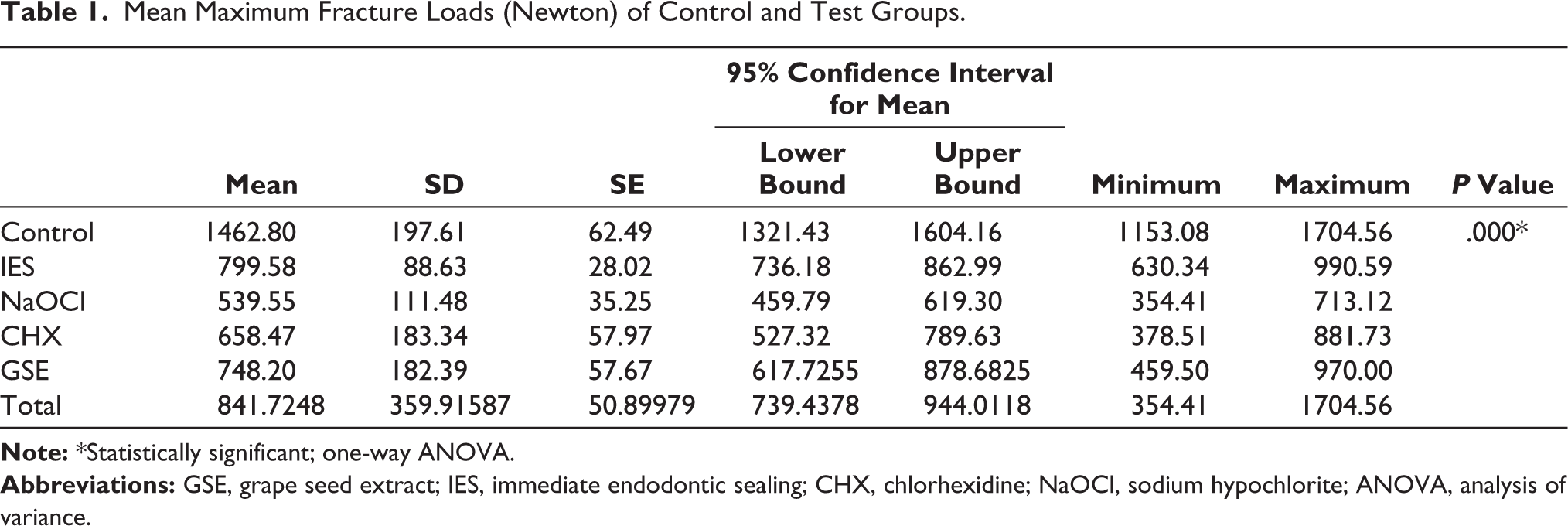
Statistical analysis was done using SPSS 22.0 (IBM, USA). Intergroup comparisons of the control group and experimental groups reported statistically significant differences with the analysis of variance (ANOVA) test. The mean and SD values of different groups are presented in Table 1. Among experimental groups, the mean fracture resistance value was highest for the IES group (799.58 N), followed by the GSE (748.20 N), CHX (658.47 N), and NaOCl (539.55 N) groups.
Mean Maximum Fracture Loads (Newton) of Control and Test Groups.
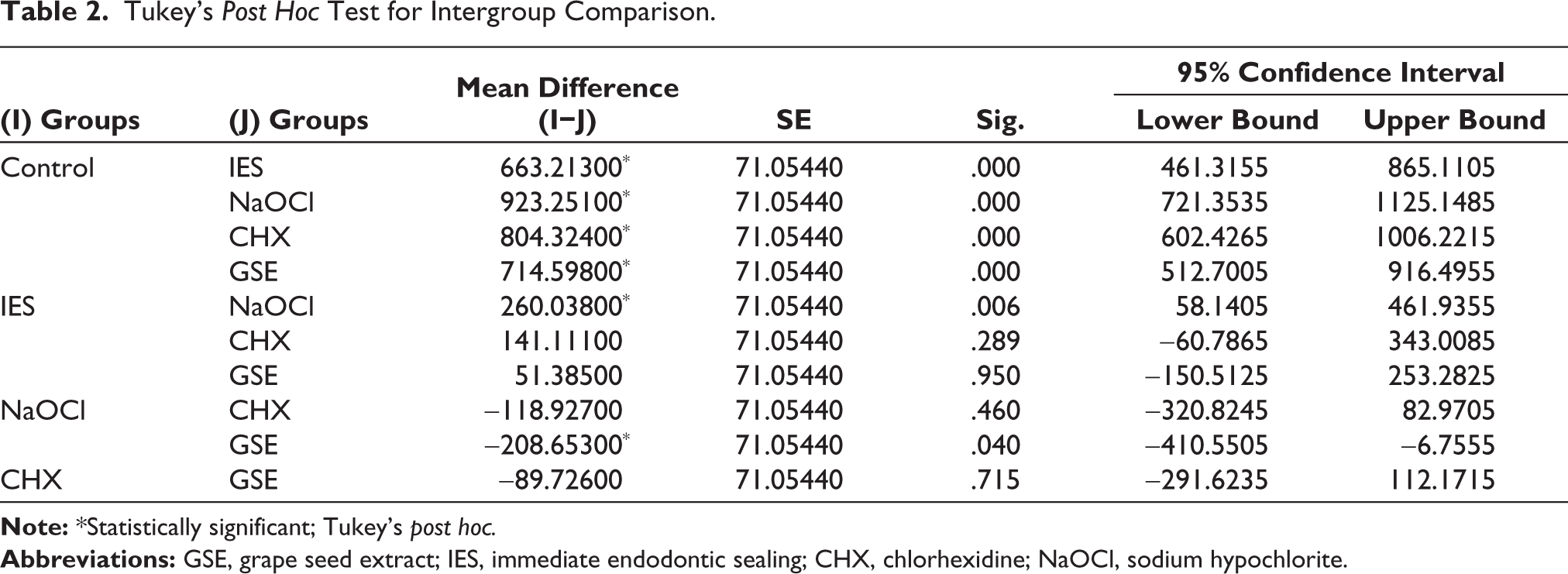
To determine specific and significant differences between groups, a Tukey’s post hoc test (Table 2) was performed, which revealed statistically significant differences among various groups. The IES group showed a statistically significant difference (p < .05) when compared with the DES groups. Grape seed-treated DES groups showed significantly increased fracture resistance compared to DES-only groups. In the dentin biomodification groups, no statistically significant difference was observed.
Examination of the failure pattern disclosed the fractures as oblique, extending from the palatal surface of the tooth to the buccal surface apical to the CEJ.
Post hoc power analysis was calculated using G* Power 3.1.9.4 software, considering an alpha level of 0.05, an effect size of 1.61, and 50 subjects in five groups. The power of the study was found to be high (100%).
Tukey’s Post Hoc Test for Intergroup Comparison.
Discussion
The coronal seal is equally important to the apical seal for the long-term success of root canal treatment. 12 Due to the micromechanical adhesion developed through bonding mechanisms, composite resin restorations are capable of reinforcing the available tooth structure. 13 Despite improvements in the adhesive systems, the resin dentin interface still remains the weakest area and begins to deteriorate in a matter of months both in vitro and in vivo. 14
In the present study, intact maxillary central incisors with similar dimensions were selected. In the anterior tooth, the most probable reason for endodontic treatment could be a carious lesion involving the proximal surfaces. 15 To represent the clinical scenario, the proximal carious lesion was represented by a standard Class III cavity extending into the access cavity, such that dentin in the Class III cavity was exposed to irrigants while performing an endodontic procedure. The effect of DES with biomodification on the fracture resistance of teeth was evaluated.
This research revealed the best performance for the control group (1462.802 N) and was statistically significant (p < .05) when compared to all the experimental groups for fracture resistance. Similar fracture strength for the intact teeth was observed in the study conducted by Chun et al. 16
The IES group showed a mean maximum load of 799.5 N. The fracture strength of the IES group was not as high as the control group. The inferior results of the IES group in comparison with the control group could be the result of loss of enamel and dentin in access and Class III cavities. 16 In the IES group, after sealing of Class III cavities and access buildup, the teeth were subjected to root canal irrigation.
The IES group exhibited higher fracture resistance than the DES group (p < .05). In the experimental groups, the lowest fracture resistance was shown by the NaOCl-treated DES group, with a mean fracture resistance of 539.55 N. The lowest fracture resistance of the NaOCl group was statistically significant compared to the IES (p < .05) group and the control group (p < .05). NaOCl acts on the organic structure, whereas EDTA chelates calcium from root canal dentin, resulting in erosion of the dentin. Chelators mainly deplete calcium through complex formation and also affect noncollagenous proteins, leading to dentin erosion and surface softening. 17
IES prevents dentin from being exposed to NaOCl irrigation used for endodontic purposes, which prevents damage to organic components of dentin and other effects on dentin structure. As a result, a consistent hybrid layer could be formed, leading to a strong resin–dentin interface. An experimental study concluded that the IES showed significantly greater internal adaptation than the DES. 6 This improved bonding interface might have increased the mechanical properties and improved fracture resistance in the IES group.
The decreased fracture resistance of the NaOCl group might be due to NaOCl, which removes exposed organic matrix from dentin by reacting with amino acids in dentin and proteins, breaking down peptide chains, and leaving a mineralized surface. This is due to the hypochlorite ion, which has a powerful oxidative effect that promotes higher collagen denaturation.7,18,19 This action of NaOCl on dentin leaves unbound hydroxyapatite apatite-rich collagen sparse dentin subsurface leading to a non-uniform effect. This destruction is responsible for the substrate, which is less tough and more brittle, predisposing it to crown or root fracture. 7
Furthermore, NaOCl has been shown to change the permeability and solubility characteristics of dentin by removing carbonate ions from the inorganic portion, compromising the quality of the hybrid layer. 5 Degree of conversion could be affected by the competing protein-derived radicals formed by NaOCl with propagating free radicals during polymerization. 9 Dentin samples, when irrigated with NaOCl, revealed changes in organic and mineral contents under electron-dispersive spectroscopy. 20
All these factors explain the lowest fracture resistance in the NaOCl-treated DES group. Therefore, in a clinical scenario, IES is recommended whenever it is possible. However, IES may not be possible in all clinical situations, especially in the case of vital pulpal tissue, which requires the use of NaOCl irrigation for pulpal tissue dissolution. In such conditions, DES can be followed, but exposure of dentin to NaOCl will have a negative effect.
The recent concept of dentin biomodification has been used to modify the mechanical properties of compromised collagen, preventing the biodegradation of extracellular matrix components and leading to a stable and durable adhesive interface. Various collagen crosslinkers and MMP inhibitors have been used as dentin biomodifiers.21,22
In the present study, GSE was used experimentally as a dentin biomodifier to reverse lost fracture strength after using NaOCl. Clinical trials of 14 months have reported minimal bond strength degradation from MMPs with the treatment of etched dentin with 2% CHX for a minute. 23 A similar protocol was followed in the present study.
The CHX-treated DES group showed increased fracture resistance of the tooth with a mean maximum load of 658.4 N when compared with the NaOCl-treated DES group. This improved fracture resistance of the CHX group compared to the NaOCl group was statistically insignificant (p-value of .460). This improved fracture resistance over the NaOCl group might be due to the diffusion of CHX into the 65% water-filled spaces exposed by the collagen fibrils of demineralized dentin. CHX inhibits the MMPs through its Zn2+ cation-chelating reaction, which removes zinc from the cysteine switch and preserves the hybrid layer. 24 Santos et al., in their respective studies, showed that the use of CHX preserved the bond strength that was lost due to the application of NaOCl.12,25 In the present study, improved fracture resistance of the CHX group over the NaOCl group might be due to improved mechanical properties because of improved bonding between resin–dentin interfaces in the proximal cavity.
In experimental groups, the GSE-treated DES group showed improved fracture resistance of teeth with a mean maximum load of 748.2 N when compared with the NaOCl-treated DES group. This improved fracture resistance was statistically significant (p = .040).
Hydroxyl sites in PAs of GSE have multiple electron donor sites that form stable hydrogen bonds and produce non-biodegradable collagen matrices. Formed hydrogen bonds between the protein amide carbonyl and the phenolic hydroxyl increase the intermolecular and intramolecular crosslinks in the collagen. This increases the mechanical properties of dentin collagen, thus enhancing biodegradable resistance and bond durability.26,27 They also remove the remnants of NaOCl by oxidation–reduction reactions. 28
PAs of GSE also inhibit collagen breakdown by reducing MMPs’ destructive potential. 24 This reduced MMP activity was confirmed by using zymography and confocal laser scanning microscopy, which showed the elimination of MMP activity at the hybrid layer.29,30 All these factors could contribute to the improved fracture resistance and strong reversal action of PA on the negative action of NaOCl. Studies have also shown that in vitro application of GSE to dentin significantly enhanced the immediate dentin bond strength. 3 The application time of GSE in those studies ranged from 5–10 min to 1 h. Therefore, in the present study, 5% GSE was used for 10 min after exposure to NaOCl. Recent literature has reported that the combination of PA + carboxymethyl chitosan/amorphous calcium phosphate nanocomplexes has improved the structural durability of endodontically treated teeth. 31 Similar to the flavonoid present in the GSE, quercetin, an irrigating solution exhibited a collagen-stabilizing effect when used as a dentin biomodifier. 32
All specimens were subjected to thermocycling according to ISO 1994 for 500 cycles, which corresponds to less than 2 months of aging in the oral cavity. Literature reports are available in research studies that have used 100–10,000 cycles. Unfortunately, the choice of parameters for thermocycling is not standardized and seems to be made according to convenience. 33
The periodontal ligament and surrounding anatomical structures were represented by a thin coat of polyvinyl siloxane, and the roots were immersed in PMMA. 34 The load was applied as in normal Class I occlusion at an angle of 135o to the long axis of the tooth. 35 In the present study, fracture patterns were mostly oblique, extending from palatal to labial, with subgingival extension in the labial aspect. This represents a clinical condition where occlusal overload causes oblique fractures extending from palatal to labial with subgingival extension in the labial aspect. 35
The null hypothesis was partially rejected, as DES modified with GSE resulted in significantly superior fracture resistance compared to CHX.
The strengths of the study include clinical simulation of carious lesions, thermocycling, and periodontal simulation.
Limitations
In a clinical scenario, endodontically treated teeth fracture due to fatigue; therefore, static loading is not the only concern. Various contact positions and angles were not considered. Future research includes dynamic loading and prospective human clinical trials.
Conclusion
Exposure of dentin to NaOCl during root canal procedures led to reduced fracture resistance of root canal-treated teeth.
IES increased the fracture resistance of root canal-treated teeth.
DES with dentin biomodifiers, such as 5% GSE and 2% CHX, increased fracture resistance of root canal-treated teeth.
Footnotes
Author Contributions
All authors contributed in study designing, data analysis and preparation of manuscript and editing.
Data Availability Statement
Available.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Institutional Ethical Committee (IEC/VDC/MDS15 ENDO 06).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.