
Abstract
Aim:
One of the problems that orthodontists commonly face is the prolonged duration of the treatment. Therefore, it is important to find an effective method to increase the rate of orthodontic tooth movement (OTM). This study aimed to evaluate the effectiveness of oral administration of vitamin D3 on OTM rates in humans.
Materials and Methods:
In this randomized clinical trial study, we selected 29 healthy women aged 18–25 years who sought orthodontic treatment and required bilateral maxillary first premolar extraction. Participants were tested to measure the blood levels of vitamin D3 and, based on the outcomes, were divided into three groups: control (without vitamin D3 deficiency; N = 10), placebo (N = 9), and experiment (N = 10), both with vitamin D3 deficiency. Subjects of the last two groups, who were randomly assigned, received 50,000 IU (International Unit) vitamin D3 pearls (Dana Pharmaceutical Company, Tabriz, Iran) or a placebo every 2 weeks for 2 months. Inclusion criteria were patients requiring bilateral extraction of the first premolar in the maxilla. The canines were retracted by nickel-titanium (NiTi) coil springs into the extraction sites. At the beginning, after 1 and 2 months, the distance between canine and lateral teeth on both sides was measured to calculate OTM.
Results:
In the first month (t (1–2)), the mean values of OTM in the placebo group were higher than the other groups. However, during the second month (t (2–3)) and overall (t (1–3)), the experiment group showed a higher OTM. The experiment and control groups were statistically different in all three time periods (P-value < .05). The difference between the experiment and placebo groups was only significant in t (2–3) (P-value < .05). Whereas the placebo and control groups showed a significant difference in t (1–2) (P-value < .05).
Conclusion:
Vitamin D3 deficiency seems to increase OTM. Receiving oral supplements of vitamin D3 may not have much effect on increasing the level of vitamin D3. The lowest OTM rate was observed in the control group.
Abbreviations
1,25-Dihydroxyvitamin D3
Bone alkaline phosphatase
High mobility group box 1
International unit
Nickel-titanium
Non-steroidal anti-inflammatory drugs
Orthodontic tooth movement
Prostaglandin E2
Parathyroid hormone
Receptor activator of nuclear factor kappa-Β ligand
Vascular endothelial growth factor
Introduction
Orthodontic treatment relies on the clinician’s ability to produce controlled tooth movement. Since the introduction of orthodontics, various techniques and devices have been developed to achieve this. Applying force to a tooth causes certain mechanical, chemical, and cellular events in the adjacent tissues that result in structural changes and ultimately the movement of the tooth. Even with different devices with different mechanisms, one must achieve the same result at the cellular level, that is, alveolar bone remodeling in the expected direction.1–3
In recent decades, more people have become candidates for orthodontic treatment. As a result, it is now a new challenge to shorten the treatment time, which is a real concern for patients, especially adults. An acceleration of the orthodontic tooth movement (OTM) has long been desired because of its various advantages, such as a shorter duration of treatment and fewer side effects such as problems related to oral hygiene, root resorption, and open gingival embrasure spaces. Therefore, various methods have been introduced in recent years to shorten the duration of treatment,4–6 some of which include piezosurgery,7–9 low-level laser therapy,10,11 fiberotomy,12,13 electromagnetic fields,14,15 corticotomy, 16 drugs, 17 and mechanical stimulation. 18
A non-invasive technique involves the use of certain drugs that can affect the rate of OTM as well as bone metabolism.19,20 Several studies have looked into the mechanisms and effects of commonly used drugs and systemic factors such as NSAIDs,21–24 corticosteroids,25,26 thyroid hormones, 27 parathyroid hormone (PTH),28,29 and vitamin D30–32 on tissue changes and OTM.
Vitamin D and its active metabolite 1,25-dihydroxyvitamin D3 (1,25,2(OH)D3), together with PTH and calcitonin, regulate the amount of calcium and phosphorus in the body.2,33 Vitamin D deficiency can lead to skeletal disorders such as osteomalacia as well as non-skeletal effects such as secondary hyperparathyroidism34,35
A study in 2011 showed that local injection of 1,25,2(OH)D3 was clinically effective in increasing the rate of OTM in humans, and it was demonstrated to be dose-dependent. 30 However, Shetty et al. 36 reported in 2015 that local injections of vitamin D3 significantly reduced the rate and amount of tooth movement in humans. According to a study, 1,25,2(OH)D3 stimulates osteoclastic bone resorption through a primary hormonal response in osteoblasts. 37 In another study, local injection of 1,25,2(OH)D3 was shown to result in an acceleration of OTM after 21 days in adult cats. 1 Kale et al. found that 1,25,2(OH)D3 promoted bone turnover more effectively than PGE2 (prostaglandin E2) and supported the balance between formation and absorption in alveolar bone remodeling during OTM. 38
Overall, there are only a few studies, most of which were carried out on animals, evaluating the effect of vitamin D3 on tooth movement. In addition, they all focus on the local effects of vitamin D3 rather than oral intake. Therefore, the aim of this study was to evaluate the effect of oral vitamin D3 supplements on OTM in humans.
Materials and Methods
Trial Design
This study used a 1:1 allocation ratio in a randomized clinical trial. The randomization was done for the participants included in the study.
Participants, Eligibility, and Setting
This single-center clinical study (Mashhad University of Medical Sciences, Dental School, Orthodontic Department) was conducted on 29 healthy women aged between 18 and 25 years seeking orthodontic treatment. Inclusion criteria were patients requiring bilateral extraction of the first premolar in the maxilla. Exclusion criteria were the presence of any systemic disease, syndrome, or bone malformation, any systemic or metabolic disease that affects bone metabolism, intake of vitamin D or another drug that can influence bone metabolism, any existing periodontitis or bone loss, and smoking.
Sample Size Calculation
According to the Al-Attar et al. study, 39 the sample size for this study was estimated and based on the ability to distinguish a clinically relevant difference in the orthodontic tooth (primary outcome) in the three groups of the trial, with a significance level of .05 and 80% power. Based on the calculation, at least 23 patients had to be assigned to each group. This was rounded up to 25 to compensate for the losses during follow-up. However, the number of patients in each group was reduced to ten due to the need for a preliminary blood test and patient reluctance. To compensate for this, measurements were taken on both sides.
Blinding
In this triple-blind study, the patient, operator (the second author), and statistician were blinded to the study so that they did not know who was receiving placebo or vitamin D3 (the pills looked the same). The placebo group was treated after the study by an internal medicine specialist for vitamin D3 deficiency.
Randomization
Each participant was assigned a random four-digit number, and the randomization was completed using the
Intervention
All patients were treated with stainless steel brackets with Roth prescriptions (0.018 Discovery, Dentaurum, Germany). The initial leveling and alignment were carried out with a 0.014 nickel-titanium (NiTi) wire, followed by a 0.016 NiTi.
After the initial leveling and alignment, the blood level of vitamin D3 was determined by radioimmunoassay (Biosource, Europe, Nivelles, Belgium). Subjects whose blood level of vitamin D3 was between 20 and 30 ng/mL (vitamin D3 insufficiency) or below 20 ng/mL (vitamin D3 deficiency) were allocated at random to either the placebo (N = 9) or the intervention group (N = 10, normal range: 30–100 ng/mL). Patients with normal vitamin D3 levels were assigned to the control group (N = 10).
Patients in the intervention group received gelatin capsules containing 50,000 IU (international unit) vitamin D3 pearls (Dana Pharmaceutical Company, Tabriz, Iran) (based on Demetriou et al. 40 ) every 2 weeks, while the placebo group received empty gelatin capsules for blinding. The control group, which had no vitamin D3 deficiency, was considered a parallel to the other two groups in order to carry out the required measurements at predetermined times.
Finally, the placebo group was treated for vitamin D3 deficiency.
Canine Retraction
Space closure was performed by retracting the canine using a 0.016-inch stainless steel wire (Remanium, Dentaurum, Germany) and a NiTi coil spring (100 g) (American Ortodontics, USA). The distance between the lateral incisor and the canine on either side of the maxilla was measured once a month for 2 months in order to determine the movement rate of the canine. For this purpose, a computerized calliper was used to measure the distance between the canine and the lateral incisor’s prominent point with an accuracy of 0.01 mm. The mean movement on either side was taken as the amount of movement for each patient. The retraction rate of the canine was defined as the amount of tooth movement per unit of time.
Statistical Analysis
The Shapiro-Wilk test revealed that the data had a normal distribution. Using SPSS software version 18 (SPSS, Inc., Chicago, IL, USA), the one-way ANOVA and Tukey tests were used to analyze the data. The statistical significance level was set to .05.
Results
Participant Flow
A total of 29 subjects aged between 18 and 25 years participated in this study: 10 subjects with vitamin D3 deficiency received dietary vitamin D3 capsules (intervention group), nine subjects with vitamin D3 deficiency received placebo capsules (placebo group), and ten subjects with normal vitamin D3 levels were considered baseline (control group). No subject left the trial during follow-up. The distance between the canine and the lateral incisor was measured at the beginning as well as 1 and 2 months after initiating the treatment to calculate the amount of tooth movement. According to the Shapiro-Wilk test, all of the data were normally distributed (P > .05).
Tooth Movement
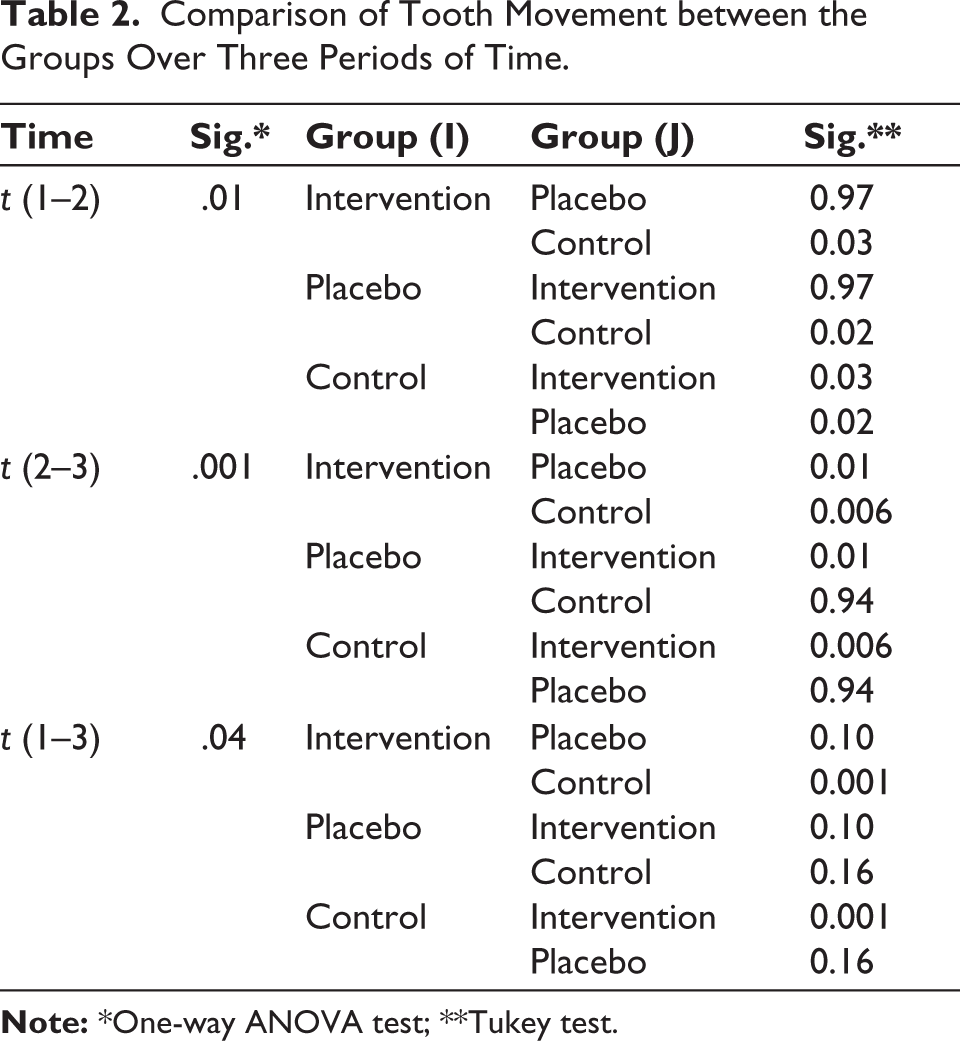
Table 1 shows the descriptive statistics of the tooth movement of the groups at three time periods. Based on the results of the one-way ANOVA test, there was a significant difference in terms of tooth movement between the groups in all three time periods (Table 2).
The Tooth Movement of the Groups at Three Time Periods.
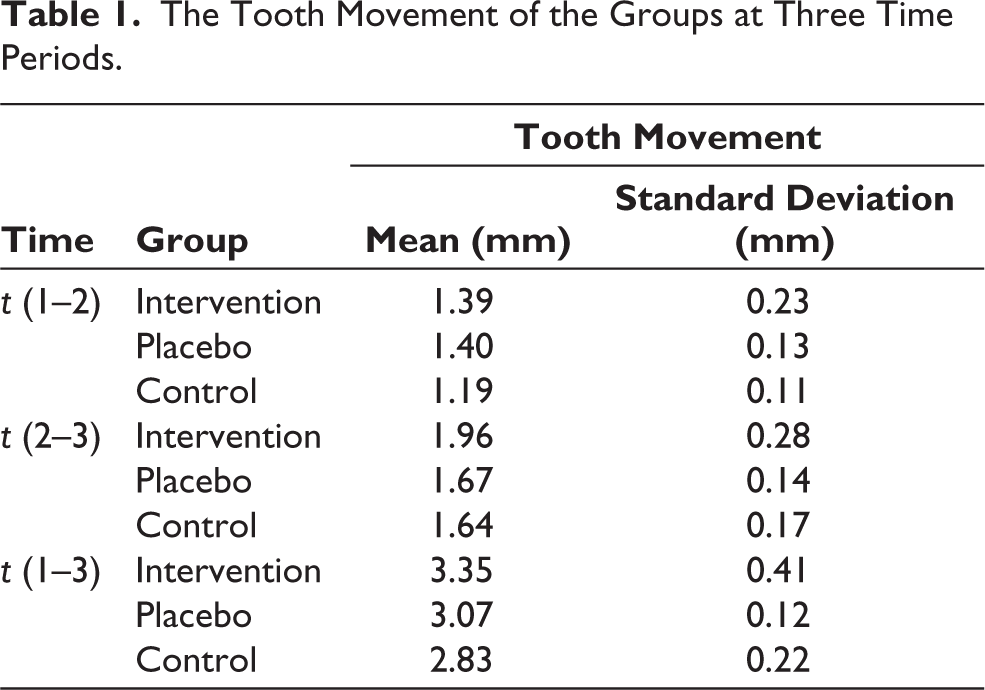
The Tukey test (Table 2) indicated that during the first period (t (1–2)), there was a significant difference between the control and intervention groups as well as between the control and placebo groups (P < .05). However, there was no noticible difference between the control and placebo groups during this period.
There was also a significant difference between the intervention and placebo groups as well as between the intervention and control groups during the second period (t (2–3)) (P ≤ .01). Overall, only the difference between the control and intervention groups was significant in both periods (t (1–3)) (P = .001).
Comparison of Tooth Movement between the Groups Over Three Periods of Time.
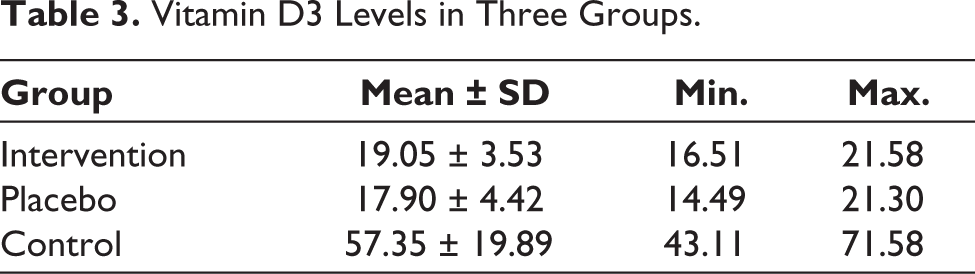
Vitamin D3 Levels in Three Groups.
Vitamin D3 Level
The preferred range for vitamin D3 is 30–60 ng/mL. 41 According to our results, 19 out of the 29 patients (65.5%) had vitamin D3 deficiency. Table 3 gives the levels of vitamin D3 in the three groups. No serious harm or side effects were observed during the entire treatment.
Discussion
Vitamin D is a potent inducer of bone resorption and formation and is one of the factors that can affect the rate of OTM.19,42 However, it has only been examined and administered locally, which is not only painful but also cannot explain the systemic effects of vitamin D3. In our research, we studied for the first time the effect of dietary vitamin D3 on OTM in humans. The results suggested that higher amounts of vitamin D3 can systemically reduce OTM.
According to Al-Hasani et al., a 25 pg dose of vitamin D3 accelerated the experimental canine movement by nearly 51% compared to the control group, while each of the 15 and 40 pg doses resulted in an approximately 10% acceleration of OTM. They therefore concluded that local injection of vitamin D3, in a dose-dependent pattern, is a cost-effective way to increase OTM in humans. 30
In their investigation on cats, Collins et al. 1 found that individuals who got weekly intraligamentous injections of a solution of 1,25,2(OH)D3 in dimethyl sulfoxide saw a 60% faster movement of their teeth than the matching control teeth. In addition, an increased number of mononuclear osteoclasts was reported in histological evaluations, which can lead to an increase on the pressure side of the periodontal ligament in alveolar bone resorption. 1
In 2019, Narmada et al. 32 found that intramuscular administration of vitamin D could increase the number of osteoclasts and receptor activator of nuclear factor kappa-β ligand (RANKL) in pregnant rats while going through OTM. However, according to Nareswari et al., 31 there was no significant increase in angiogenesis or vascular endothelial growth factor (VGEF) expression in the Wistar rat after intramuscular vitamin D injection. Another 2019 study evaluated the effects of intramuscular injection on OTM in rats. The results showed no significant growth in the number of osteoblasts or bone alkaline phosphatase (BALP) expression compared with the control group. 43
Kale et al. 38 compared the effects of 1,25,2(OH)D3 and prostaglandin E2 on OTM. They showed that both PGE2 and 1,25,2(OH)D3 significantly increased the amount of tooth movement compared to the control group. Additionally, there were considerably more osteoblasts on the alveolar bone’s external surface on the pressure side in the 1,25,2(OH)D3-injected group than in the PGE2 group. They therefore concluded that 1,25,2(OH)D3 is effective in modulating bone turnover during OTM in rats.
In 2016, Cui et al. 44 suggested that local administration of 1,25,2(OH)D3 might provide a suitable periodontal ligament environment for OTM in rats. This was due to a decrease in the expression of HMGB1 (High Mobility Group Box 1); an inflammatory cytokine that can act as a regulator in remodelling of periodontal tissue and bone resorption during OTM.
Based on a study by Takano-Yamamoto et al., 45 the number of osteoclasts triggered by the insertion of an elastic band can be increased with daily injections of 1,25,2(OH)D3. It was synergistic with mechanical stimuli and resulted in higher counts of osteoclasts compared to mechanical stimuli alone. These results suggest that local application of 1,25,2(OH)D3 can increase osteoclast counts as well as osteoclastic bone resorption activity induced by mechanical stimuli.
In a study by Baran et al. 46 on rats, it was shown that areas with local administration of 1,25,2(OH)D3 had a significantly higher unilateral apposition compared to the control group.
In another study, Takano-Yamamoto et al. 47 reported that in young rats who received 10–10 mol/L of 1,25,2(OH)D3 injections every three days, tooth movement increased by 245%. Moreover, upon receiving 10–8 mol/L injections, tooth movement increased by 154% compared to that observed in the control group by the end of the experiment.
However, Shetty et al. 36 showed in 2015 that local injection of vitamin D3 can significantly reduce the rate and amount of tooth movement in humans after a 60-day trial period, contradicting previous results.
The findings of our research suggested that higher levels of vitamin D3 in the blood can reduce the rate of OTM.
Strengths and Limitations
The sample size in our study was smaller than expected due to the need for a preliminary blood test and the unwillingness of patients to do so. Because of this lack of cooperation, the secondary vitamin D3 level (after the experiment) could not be measured. Also, the study period was limited for ethical reasons.
Noteworthy, however, was the innovation in this study, which for the first time used oral supplements instead of injections. In this study, we also measured the preliminary level of vitamin D3, which has not yet been carried out in other studies. Vitamin D3 or placebo capsules were orally administered at the start of each follow-up visit under the researcher’s supervision, which reduced the risk of not taking vitamin D3 to zero. This trial was one of the few studies on humans and the first to look at the Iranian population. There are only a few studies on this subject examining the effects of local injections of vitamin D3, most of which were carried out on animals. Due to the normal distribution of the data, the findings of this investigation can be reliably generalized.
Conclusion
The findings of this research indicated that vitamin D3 deficiency increased OTM. There was no noticible difference between the placebo and intervention groups. The lowest rate of OTM was found in the control group without vitamin D3 deficiency. According to the results, the short-term intake of vitamin D3 supplements (2 months) did not have a major influence on the rate of tooth movement.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Informed Consent
After primary case selection, the study phases were explained to the patients, and signed informed consent was obtained from each of them (no changes were made to the methods after the start of the study).
The study protocol was approved by the research ethics committee of the Mashhad University of Medical Sciences.
Funding
This study is funded by the Research Chancellor of the Mashhad University of Medical Sciences.