
Abstract
Introduction:
The objective of this systematic review is to assess the effect of vibrational force on biomarkers for orthodontic tooth movement.
Methods:
An electronic search was conducted for relevant studies (up to December 31, 2020) on the following databases: Pubmed, Google scholar, Web of Science, Cochrane Library, Wiley Library, and ProQuest Dissertation Abstracts and Thesis database. Hand searching of selected orthodontic journals was also undertaken. The selected studies were assessed for the risk of bias in Cochrane collaboration risk of bias tool. The “traffic plot” and “weighted plot” risk of bias distribution are designed in the RoB 2 tool. The 2 authors extracted the data and analyzed it.
Results:
Six studies fulfilled the inclusion criteria. The risks of biases were high for 4, low and some concern for other 2 studies. The biomarkers, medium, device, frequency and duration of device, as well as other data were extracted. The outcomes of the studies were found to be heterogenous.
Conclusion:
One study showed highly statistically significant levels of IL-1 beta with <.001. Rate of tooth movement was correlated with levels of released biomarkers under the influence of vibrational force in 3 studies, but it was found to be significant only in 1 study. It was further observed that vibration does not have any significant reduction in pain and discomfort.
Introduction
The average orthodontic treatment ranges from 2 to 3 years. Prolonged orthodontic treatment adversely affects the patients’ compliance and predisposes the patient to an increased risk of gingival inflammation, decalcification, dental caries, temporomandibular disorders, speech problems, and root resorption with future debilitating consequences. 1 Accelerating the rate of orthodontic tooth movement is desirable to both the orthodontists and the patient. It has received an increased attention by academicians and clinicians. Various procedures have been advocated to reduce the overall treatment time which includes both surgical and non-surgical modalities.
Surgical methods include corticotomy, 2 decortication, 3 and distraction osteogenesis. 4 However, these are associated with side effects such as periodontal defects, 5 post-operative pain and swelling, and in severe cases, subcutaneous hematomas 6 of the orofacial region. Various nonsurgical methods include low-intensity lasers, 7 pulsed electromagnetic fields, 8 electric currents, 9 and vibration, 10 and these are free from the above stated side effects.
Vibration is one of the latest methods to accelerate orthodontic treatment 11 and has been strongly promoted in recent years. Apart from enhancing tooth movement, it also exhibits the proposed advantages of pain reduction 12 after orthodontic adjustment as well as reduction of frictional resistance to sliding 13 (stick–slip phenomena) between brackets and archwires. Devices capable of delivering vibrational force are now commercially available and are convenient, portable, and can be used by the patients themselves. 14
Vibrational force can be defined by specifying 2 of the following 3 variables: frequency (number of oscillations per second expressed in Hertz), magnitude of the induced peak acceleration (expressed typically with the acceleration of the Earth as a referent where 1 g = 9.81 m/s 2 ), and/or the total displacement produced by the oscillating vibrating actuator (expressed in mm or cm). 15
Application of vibrational force initiates stress-induced charges by rapidly applying an intermittent force. Shapiro et al 16 have suggested that an increase in the rate of tooth movement occurs when the orthodontic forces are cyclic in nature, which is essential for generation of piezoelectric charges. These charges induce microcurrents to flow through bone and soft tissue and may enhance tooth movement by stimulating osteoblastic and osteoclastic activity.
Orthodontic tooth movement induces mechanical stress, following which a cascade of events takes place causing release of various cytokines, eicosanoids, and other arachidonic acid metabolites that are responsible for remodeling of surrounding hard and soft tissues. 17 Levels of these inflammatory cytokines can be measured in various extracellular fluids such as gingival crevicular fluid (GCF) 18 and saliva. 19 Therefore, these can be considered as potential biomarkers of orthodontic tooth movement. Several potential biomarkers have been identified in various studies such as interleukin (IL)-1 beta, IL 8, IL 5, IL 6, and IL 2, tumor necrosis factor (TNF)-alpha, receptor activator of nuclear factor kappa-Β ligand (RANKL), Osteoprotegerin (OPG), and osteocalcin, which are associated with orthodontic tooth movement. 20
Levels of proinflammatory cytokines are associated with vibrational force, as shown in several in vitro studies, 21 and other in vivo studies have demonstrated the effect of vibrational force with orthodontic appliance on biomarkers. However, in both in vivo and in vitro studies, results have been found to be contradictory.
Thus, a focused research question was formatted: “What is the effect of various supplemental vibrational forces on different biomarkers involved in orthodontic tooth movement?”
Therefore, the purpose of this study was to systematically review the available literature to evaluate the potential effects of supplemental vibrational forces on biomarkers associated with orthodontic tooth movement in humans.
Objectives
The aim of this study was to elucidate through a systematic review the potential effects of supplemental vibrational forces on biomarkers associated with orthodontic tooth movement.
Materials and Methods
Protocols and Registration
The systematic review was performed in accordance with the preferred reporting items for systematic review and meta-analysis guidelines, and the main research question was formatted according to population/participants, intervention(s), comparator(s)/control , outcome(s) (PICO). The protocol was registered with the number CRD42020204763 in the PROSPERO database (
Search Strategy
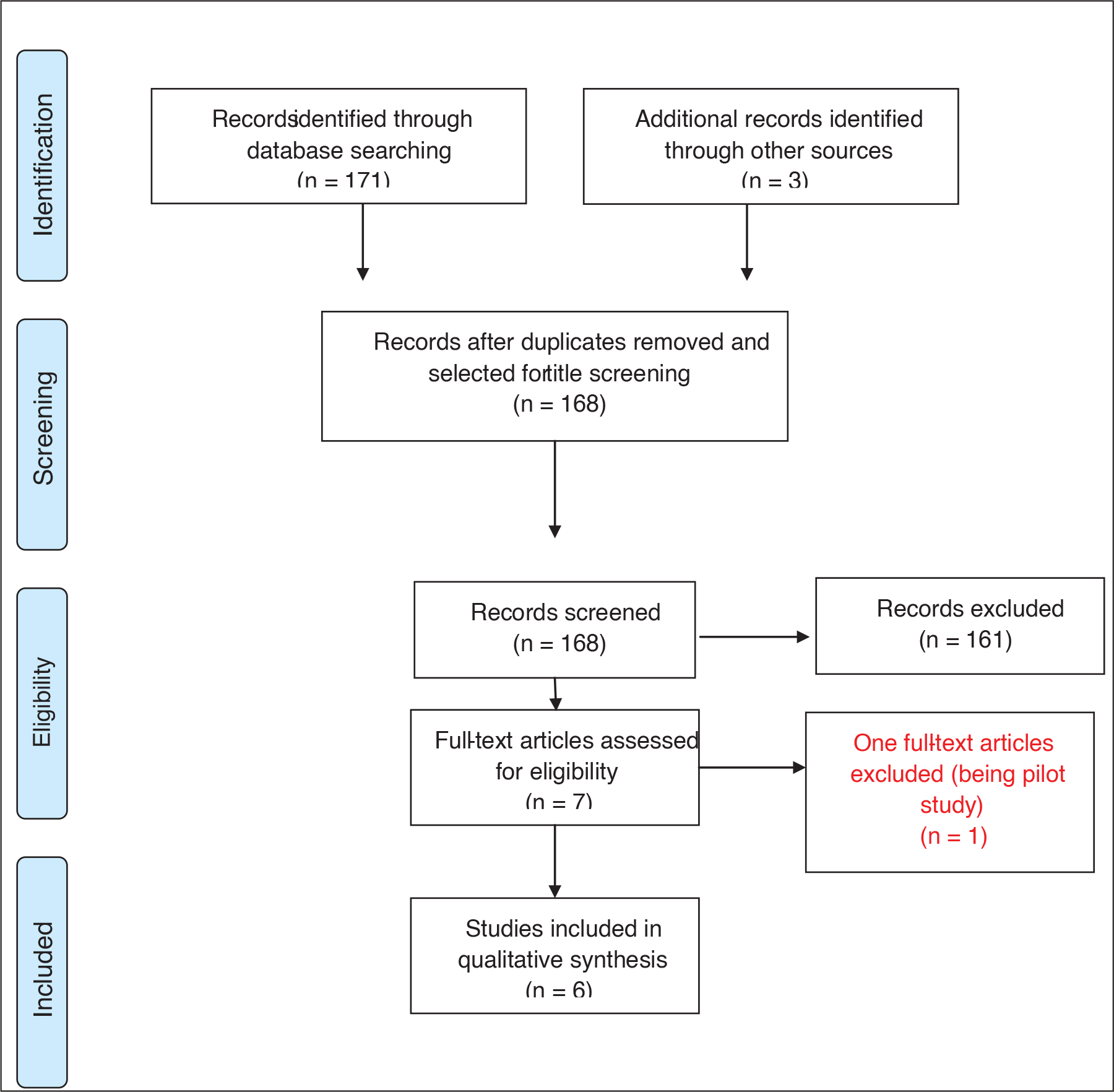
This systematic review was performed in accordance with the statement of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). The comprehensive electronic database search was conducted with no limit of date of publication.
List of Search Engines and Their Results.
We used the following search terms for Pubmed:
All electronic search strategies shared similar combinations of medical subject headings (MeSH) terms and texts. Two independent authors (TM and AA ) screened initial titles and abstracts to find any potential eligible studies. The short-listed studies were selected for full text reading and full texts were retrieved carefully according to inclusion and exclusion criteria.
Any disagreement was resolved after discussion. If necessary, the third author was consulted.
PRISMA flow diagram has been presented separately (Figure 1).
Selection Criteria
The selection criteria were worked out according to Population; Intervention; Comparison; Outcomes; Study design (PICOS).
Population
All subjects indicated for fixed orthodontic treatment.
Intervention
Fixed orthodontic therapy along with vibrational device either on the experimental or split mouth technique in selected sample.
Comparison
Between control and experimental groups or in split mouth designs in selected samples.
Outcome
To identify the levels of biomarkers in response to fixed orthodontic therapy along with vibrational device.
Study Design
RCTs.
(b) Subjects: patients indicated for removable appliances or orthognathic surgery, patients lacking dexterity, taking drugs such as corticosteroids or non steroidal anti inflammatory drugs (NSAIDS), and systemically compromised patients.
Data Extraction
The data extraction was performed by 2 reviewers (TM and AA) independently to record the general information such as author, year of publication, vibration frequency and duration, biomarker, medium, characteristics of subjects, interventions, sample size, method of examination, additional effects, observation time, and outcome.
Risk of Bias/Quality Assessment of Selected Studies
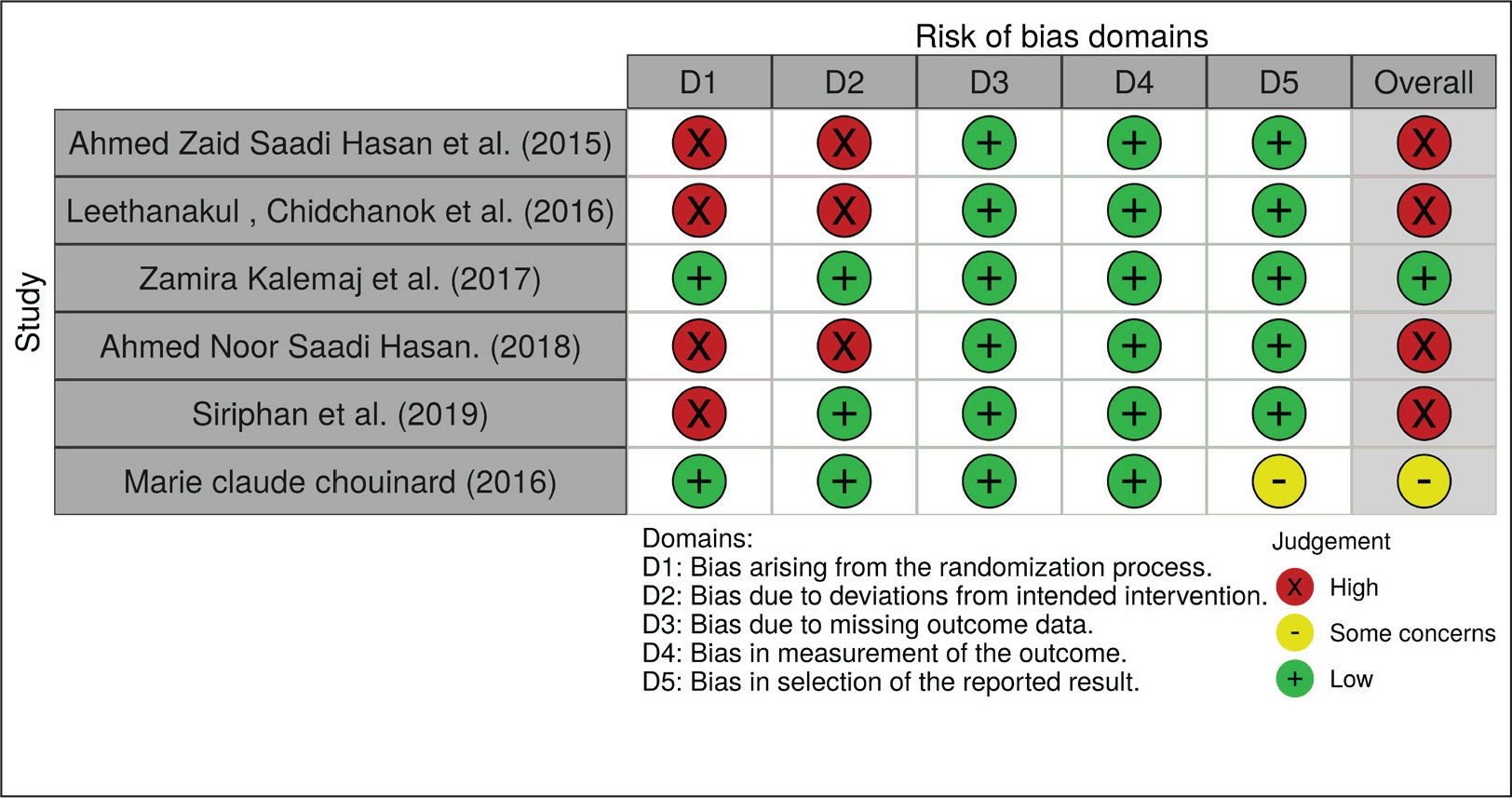
Independent quality assessment of the included studies was performed by a pair of observers (TM and AA) using the Cochrane collaboration risk of bias tool Risk-of-bias VISualization (ROBVIS) (RoB 2)
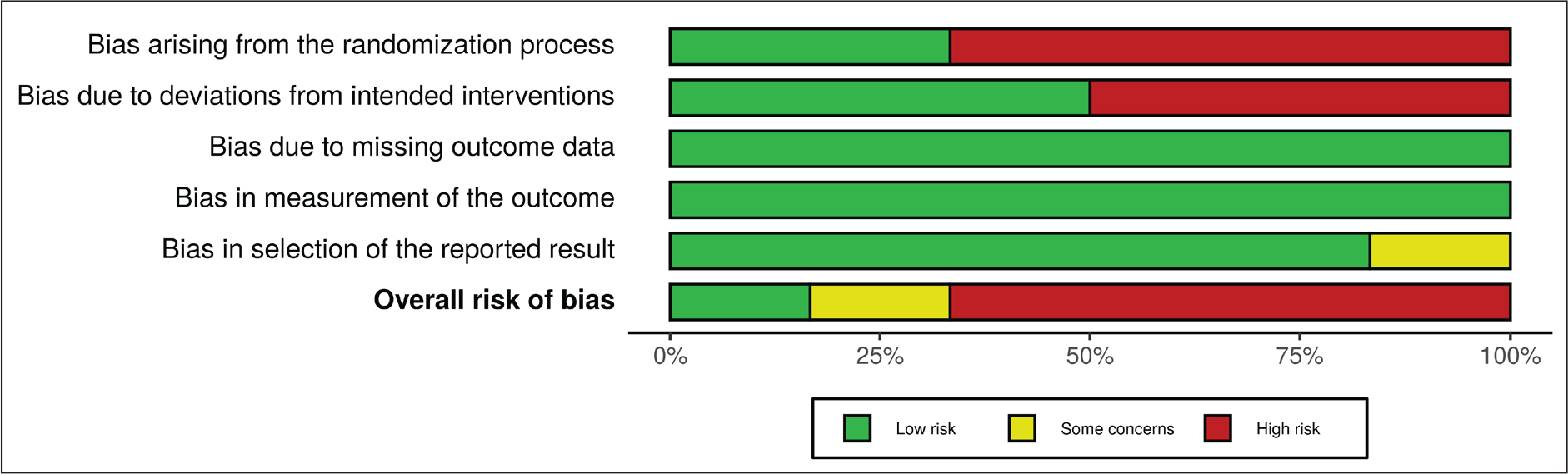
A total of 5 domains of bias were assessed: (a) bias arising from randomization process, (b) bias due to deviation from intended intervention, (c) bias due to missing outcome data, (d) bias in measurement of the outcome, and (e) bias in selection of the reported result.
The studies were categorized as follows: (a) high risk, (b) some concern, and (c) low risk categories (Figures 2 and 3).
Results
Study Selection and Criteria
List of Excluded Studies and Their Reasons.

Basic Characteristic of the Selected Studies.
Outcomes of the Studies Under Consideration.
Synthesis of Results
Meta-analysis was not performed due to the heterogeneity of the devices, techniques, additional outcomes measured in each study, and statistical method used.
Discussion
Accelerated tooth movement reduces the overall treatment time which is beneficial to both the orthodontist and the patient. Research in this field has been conducted extensively, and it is fetching promising results. Increase in the rate of tooth movement by enhancing the biochemical reaction within the hard and soft tissues has been investigated using different methodologies.
Reducing friction during fixed orthodontic therapy, surgical corticotomy, 2 biostimulation using low energy laser, 7 photobiomodulation, application of magnetic field, 8 microampere electric stimulation, 9 and injection of proinflammatory cytokines 23 are few modalities for enhancing tooth movement, although there are few disadvantages in response to the above therapies like pain and discomfort to the patients. Vibration device is an alternative for stimulating levels of biomarkers such as IL-1 beta, IL 6, TNF-alpha, and osteocalcin in the tissue, which indicates increased bone remodeling and probable increased tooth movement.
Animal studies have not clearly indicated the beneficial effects, and various clinical studies have reported mixed results24-26 in response to vibration devices; therefore, a systematic review of viability and effect of vibration device on biomarkers is deemed necessary. This will be useful in future research relating to Wilckodontics.
At the time of registration with Prospero, this systematic review was the first to specifically examine the effect of vibrational device on levels of biomarkers when applied simultaneously with fixed orthodontic therapy.
In vitro studies27-31 and different in vivo studies32-37) conducted in the past using various biomarkers and vibration devices have reported mixed results.
For this systematic review, a total of 174 articles were selected through the use of MeSH terms and few articles were handpicked. After using regressive scrutinization using inclusion and exclusion criteria, 6 articles were finally considered for this systematic review.
Summary of Evidence
Six different RCTs were assessed and evaluated to analyze the effect of different vibration devices on tooth movement. The impact of vibration forces on different biomarkers present in saliva and GCF was studied in all the RCTs. The methodological heterogeneity was noted in all these studies, as some authors have used different devices as well as frequency of vibration.
Also, the medium tested for biomarkers was different, with some considering saliva while others considered GCF as the respective medium for their analysis.
In their RCT, Leethanakul et al 32 evaluated the levels of IL-1 beta on application of vibratory stimuli, which was delivered via an electrical toothbrush. The sample size was 15 (11 females, 4 males) with an age range of 19 to 25 years who underwent fixed orthodontic therapy with extraction. They were randomly divided into 2 groups: the experimental group was instructed to hold the toothbrush to apply mechanical vibration on the mesiolabial surface of canine for 5 m 3 times a day for 2 months and the control group received no vibrational device. The duration of the study was of 3 months and the force used for canine distalization was 60 g, which was determined using a force gauge. The measured outcomes were IL-1 beta levels in the GCF and the amount of tooth movement. Amount of tooth movement was assessed on models from each subject before starting canine retraction and subsequently after 1 month, 2 months, and 3 months. GCF levels of IL-1 beta were analyzed using ELISA kit before placement of brackets and then at similar time intervals as described above. The results of the study have shown that vibratory stimuli enhanced secretion of IL-1 beta in GCF as well as accelerated tooth movement. Furthermore, for the pressure side, the IL-1 beta levels were significantly higher for experimental teeth than for control teeth (T2; P = .001, T3; P = <.001). For the tension side, a significant difference between the levels of IL-1 beta of control and experimental teeth was observed only at T3 (P = 0.001).
The study has an overall high risk of bias, as the author has not stated any method for concealment of allocation sequence, and it was also mentioned that the experimental side was selected by the trial supervisor. In addition, important non-protocol interventions were also not balanced among the groups, with no appropriate analysis being implemented to estimate the effect of adhesion, which also contributes toward high risk of bias.
Ahmed et al 33 conducted an RCT with 32 adult patients of mean age 19-23 years who were randomly allocated into 2 groups: study group (acceledent device with fixed orthodontic therapy) and control group (fixed orthodontic appliance only). The study was aimed to determine the effect of vibrational device with fixed orthodontic appliance on salivary IL-1 beta and TNF-alpha levels as well as effect of vibration on gingival health. All subjects were with class I or class II malocclusion indicated for first premolar extraction. Vibration of 30 Hz was delivered to teeth for approximately 20 min/day. Unstimulated whole saliva was collected before placement of fixed orthodontic appliance, 1 h after placement of appliance and subsequently after 1 week and 2 weeks. Levels of salivary IL-1 beta and TNF-alpha were determined with the help of ELISA kit. Gingival health was assessed using gingival and plaque index. The authors found that the mean value of both salivary IL-1 beta and TNF-alpha among study group were higher than control group at T1 (1 h after placement), followed by T2 (1 week after placement), then T3 (2 weeks after placement) with statistically significant difference (P < .05).
Values of plaque index with respect to study group were found to be higher for males than females with statistical significance of P < .05; however, it was observed only at T3, whereas among control, no statistical significance was found at any time interval. Values of gingival index among study group showed lowest mean value at T3 with significant difference (P < .01) among total sample and both males and females, while the value for the control group was not found to be statistically significant.
In this trial, no method has been described for concealment of allocation sequence which puts the study in high risk. Also, the carers were aware of participants’ assigned intervention and important non-protocol interventions were not balanced between the groups. In addition, appropriate analysis to estimate the effect of adhesion was not conducted, which contributes toward high risk of bias. Therefore, the study has an overall high risk of bias.
Kalemaj et al 34 conducted a 3-armed parallel group RCT with the allocation ratio of 1:1:1. A sample of 33 patients was randomly categorized into 3 groups (conventional ligating appliance group, self-ligating appliance group, and self-ligating appliance with accledent group). The age of the patients who underwent non-extraction fixed appliance therapy was less than 25 years. The primary outcomes were rate of mandibular incisor alignment, concentration of 1L-1 beta, and pain and discomfort. Secondary outcomes included quantity of GCF and periodontal depth. Little’s Irregularity Index was used to measure alignment on dental cast before placement of archwire and at monthly intervals for the first 3 months. Levels of IL-1 beta were analyzed by ELISA in GCF collected before application of archwire, after 1 h, after 1 week, and after 3 weeks.
Pain and discomfort were evaluated through visual analog scale (VAS) at 4 h, 24 h, 3 days, and 1 week after their first visit. Patients were instructed to use acceledent device 20 min/day for 4 weeks. The authors found that vibrational devices seem to enhance GCF secretion of IL-1β particularly at 1 hour, especially for the SLA-VA group when compared to SLA group (P = .0209) and more importantly when compared to CLA and SLA-VA group (P = .0018). Regarding the mandibular incisor alignment, during the first month, higher alignment was observed for SLA and SLA-VA groups as compared to CLA group, with differences being statistically significant (P = .0267). No relevant differences in terms of pain and discomfort were observed between groups at any time point of measurement. The study has an overall low risk of bias.
Ahmed 35 evaluated the effect of acceledent in conjunction with conventional orthodontic force on salivary levels of osteocalcin during early stages of tooth movement. Thirty adults with average age of 18 to 23 years requiring fixed orthodontic therapy were randomly allocated in 2 groups: control group (fixed orthodontic appliance only) and intervention group (fixed orthodontic appliance with acceledent device). The intervention group was instructed to use acceledent device for 20 m once daily. Unstimulated whole saliva was collected before placement of appliance, 1 h after placement, and subsequently, after 1, 2, and 3 weeks. No additional effect was measured. Salivary osteocalcin levels were determined using ELISA. It was concluded that both groups show a statistically significant (P = <.001) mean increase in levels of salivary osteocalcin at each time interval; however, the intervention group was associated with an extra increase in salivary osteocalcin compared to control, especially after 1 h and after 3 weeks of treatment (P = <.001).
No method for concealment of allocation sequence has been described, which puts the study in high risk. In addition, the carers were aware of the intervention that has been given to the participating subjects; also, important non-protocol interventions were not balanced between the groups with no use of appropriate analysis to estimate the effect of protocol adhesion, which also contributes toward high risk of bias. Therefore, the study has an overall high risk of bias.
Siriphan et al 36 conducted an RCT to determine the effects of vibratory stimulus on canine distalization as well as on RANKL and OPG secretion. Sixty patients with mean age of 18 to 25 years and with first premolar extracted were randomly allocated into 3 groups: 30 Hz with canine distalization group, 60 Hz with canine distalization group and canine distalization group (control). A force of 60 cN was used to distalize canine using NiTi closed coil springs, reactivated every 4 weeks. A modified electric tooth brush was used for delivery of vibrational stimulus. GCF was collected for analysis of RANKL and OPG using ELISA immediately before canine distalization, and thereafter at 24 h, 48 h, 7 days, and 3 months. Rate of canine movement and its angulation was assessed with study models, and lateral cephalogram was taken immediately before canine distalization and after 3 months. Authors found no within- or between-group differences in RANKL and OPG (P > .05) except for RANKL on the compression side of the control group at T2, T3, and T4 than T1 (P < .001). Also, it was concluded that vibratory stimulus does not accelerate the rate of canine movement when compared to orthodontic force being applied alone. The study has an overall high risk of bias as the allocation sequence was not concealed.
Chouinard 37 conducted an RCT to determine the effects of vibration along with fixed orthodontic appliance on the expression of biological factors involved in bone remodeling, degree of tooth mobility, rate of tooth movement during alignment phase, and control of pain and quality of life. A total of 14 patients with ages ranging from 15 to 35 years were randomly allocated to 2 groups: 1 group used a vibration device 20 min/day in combination with fixed appliances and the other group solely had fixed appliances treatment (control). The patients who were allocated to the vibration treatment group were instructed to use the vibration appliance (Acceledent) 20 minutes per day according to the manufacturer’s instructions. Data were collected before bonding of brackets and thereafter at 5 to 6 weeks, 10 to 12 weeks, and 15 to 17 weeks. Levels of biomarkers, degree of tooth mobility, rate of alignment, and control of pain and quality of life were assessed using ELISA, periotest, irregularity index, VAS, and oral health impact profile 14, respectively. The author found no statistically significant difference in the expression of IL-1B, IL-8, and TNF-α when control group was compared to acceledent group. Further application of vibration during orthodontic treatment did not show a statistically significant difference in the rate of tooth movement, the level of pain experienced by the patient, as well as the oral quality of life assessment compared to the control group. However, tooth mobility at the level of the incisors significantly increased after bonding, peaking at the 5 weeks’ adjustment appointment. The study was found to have an overall some concern due to bias in selection of reported result as the authors have not mentioned the data for the levels of TNF-alpha.
Various RCTs revealed that different kinds of vibration devices used in fixed mechanotherapy had significant effect on rate of tooth movement. They advocated that it is because of effects of various biomarkers being present in bone and GCF. Leethanakul et al, 32 Ahmed et al, 33 Kalemaj et al, 34 and Chouinard 37 evaluated the effect of interleukins, TNF-alpha biomarkers on tooth movements. In a study by Ahmed 35 effect of vibrating devices was analyzed on osteocalcin. Siriphan et al 36 conducted an RCT to determine the effects of vibratory stimulus on secretion of RANKL and OPG.
Thus, in all the studies, the basic aim was to study the impact of vibration forces on fixed orthodontic appliances causing increased rate of tooth movement. Results of all RCTs advocated that effect on various kinds of biomarkers can lead to changes in movement of teeth.
Conclusion
The ability of vibration to enhance bone remodeling by increasing the levels of various biomarkers has been studied by several authors. One study showed highly statistically significant levels of IL-1 beta with P < .001. Rate of tooth movement was correlated with levels of released biomarkers under the influence of vibrational force in 3 studies, but it was found to be significant only in 1 study. It was further observed that vibration does not have any significant reduction in pain and discomfort. It is, therefore, conclusive that efficacy of vibration device for accelerating tooth movement cannot be considered definitive. Further research concerning parameters such as frequency levels, wavelengths of vibration device, duration of its application, and rate of tooth movement should be considered.
Limitations
Using vibrational force in orthodontics is an emerging method with controversial evidence in scientific literature.
Original results may vary due to different devices, time duration of use of these devices, associated fixed orthodontic appliance, circadian rhythm, and specimen type.
Footnotes
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.