
Abstract
Aim:
To determine the association between chronic diseases (CD) and the need for dental treatment in patients of the stomatology of special patients service (SSPS) of the Teaching Dental Center (TDC) of Universidad Peruana Cayetano Heredia (UPCH) in Lima-Peru from 2016 to 2019.
Materials and Methods:
A cross-sectional study with a total population of 2024 digital medical records of individuals over 18 years old. A dependent variable was need for dental treatment, so an instrument to assess it was created; additionally, the presence of CD was evaluated. Other covariates considered were pharmacological treatment, last dental visit, provenance, age group, and sex. Statistical analyses were performed, including a bivariate analysis using the Chi-square test. Finally, a Poisson linear regression was performed to determine crude and adjusted prevalence ratios (aPR) with the variables showing associations, with a 95% confidence level (95%CI) and a p < .05 value.
Results:
The need for low-complexity dental treatment was present in 2.62% (n = 52) of patients, moderate complexity in 27.21% (n = 541) of patients, and high complexity in 70.17% (n = 1395) of patients. In relation to CD, 30.58% (n = 608) had one, 31.39% (n = 624) had two, and 38.03% (n = 756) had three or more. In the multivariate analysis, the presence of three to more CD and the need for high-complexity vs. low-complexity treatment, an aPR of 1.02 (95%CI): 1.01–1.04; p = .019) was obtained.
Conclusion:
There is a positive association between the presence of three or more CD and the need for high complexity dental treatment compared to low-complexity dental treatment, adjusted for use of pharmacological treatment and age.
Abbreviations
Adjusted prevalence ratio
Chronic diseases
Prevalence ratio
Stomatology of special patients service
Teaching Dental Center
Universidad Peruana Cayetano Heredia
95% confidence interval
Introduction
Chronic diseases (CD) are characterized by being non-reversible, perennial pathologies that generate residual disability. The disease that presents one or more of these characteristics will be considered CD, so the patient with CD will require specialized rehabilitation with long periods of care. 1 In reference to CD, the World Health Organization (WHO) and the Center for Disease Control (CDC) establish similar concepts of CD, alluding to those of long duration using various classifications. 2 Among the most representative ones, cardiovascular diseases, respiratory diseases, cancer, and diabetes stand out; however, infectious diseases are excluded. 3 It is worth considering that some infectious diseases, such as the human immunodeficiency virus, can behave as a CD. 2 For this study, the term CD indicates the organic cause that, in the long term, generates health problems that give rise to medical and dental treatment needs. Likewise, CD represents the first avoidable cause of morbidity and mortality in Latin America, compromising a considerable and sustained increase in health expenditure in the countries. 4 In Peru, noncommunicable diseases represent the main causes of disability and early death, and their presence is equivalent to more than half of the annual burden of disease generated in the country. 5
On the contrary, WHO conceptualizes multimorbidity as the coexistence of two or more CD in the same person, which could be associated with immune changes related to aging that increase the intensity of pre-existing diseases; 6 in addition, it is observed that multiple CD, including some diseases of the oral cavity, share modifiable risk factors and can manifest themselves in the same individual. 7 The importance of adequate oral health for overall wellbeing is evident; however, the WHO reports that access to dental care is scarce and does not meet the needs for care of the world’s population.8,9 This last aspect reflects the impact of pathologies on people’s health, manifesting itself in the degree of deficiencies and dysfunctions they experience; however, oral health plays a particular role, being perceived in several cultures as a system independent of the body and its need for treatment as an elective decision, possibly affecting the high prevalence of oral cavity diseases in the general population, including patients with CD.10,11
In relation to what has been previously described, it is documented that people with chronic health conditions have a greater predisposition to present untreated CD, which can lead to partial or total edentulism, severe loss of teeth, periodontal disease, and so on. It should be emphasized that these are preventable if access to dental health is ensured in a timely manner and without limitations. 12 However, scientific evidence that addresses the need for treatment and characteristics that have an impact on the stomatological and general health conditions of people with CD in Peru is scarce. For this reason, the aim of the present investigation was to determine the association between CD and the need for dental treatment in patients of the stomatology of special patients service (SSPS) of the Teaching Dental Center (TDC) of Universidad Peruana Cayetano Heredia (UPCH) in Lima-Peru from 2016 to 2019.
Materials and Methods
The present study was cross-sectional and comprised a total population of 2024 digital medical records of adults over 18 years old who attended the SSPS of the TDC of UPCH from April 1, 2016, to December 31, 2019, where a final sample of 1988 records was established. Among the participation criteria, all records with complete information were included, and those that did not meet this consideration were discarded. Regarding the study variables, the need for dental treatment was conceptualized as an indispensable or obligatory treatment that seeks to maintain the oral health of the individual. It contemplates three possibilities: the need for low complexity treatment, the need for medium-complexity treatment, and the need for high-complexity treatment. To measure this variable, the instrument “Classification of dental treatment according to complexity in patients of the special patients stomat- ology service of the TDC of UPCH” was designed and developed. The validation of the instrument will be explained in more detail in the techniques and procedures section.
Likewise, another of the variables established was the presence of CD, defined as those diseases characterized by being permanent, leaving a residual disability, and always originating from non-reversible pathologies. 1 It was categorized according to whether the individual presented one CD, two CDs, or three or more CDs, according to the International Classification of Diseases (ICD-11). Other covariates considered were pharmacological treatment as a qualitative variable, which was categorized as no treatment, up to two drugs, and three or more drugs. Additionally, the last dental visit was included as a qualitative variable that is distributed into less than 6 months, 6 months to 1 year, and more than 1 year. Similarly, provenance was included: a qualitative variable that considered two options, namely, Metropolitan Lima and regions of Peru. The age group was also analyzed as a qualitative variable covering the years elapsed since birth, grouped as follows: young people aged 18–29 years, adults aged 30–60 years, and older adults aged 61 years and over. Finally, the sex variable was qualitative and grouped into men and women.
Techniques and Procedures
First, an instrument was designed and originated to measure the variable need for dental treatment, evaluated by addressing four dimensions: dental treatment, CD, pharmacological treatment, and patient behavior. The sum of its components results in the classification of dental treatment according to complexity. Once the design and structuring had been completed, a pilot test of experts judgment was carried out made up of eight specialists from different dental areas. It is worth mentioning that four of the specialists worked in the area of special patient stomatology: two in pediatric dentistry, one in geriatric dentistry, and one in community dentistry. It should be noted that these professionals came from other countries, so their contribution provided a broader perspective.
Following this, experts sent their comments through e-mail, attaching observations and recommendations on the instrument developed, its dimensions, and the score assigned to each one. These comments were accepted and corrected, and then sent to the specialists for a second opportunity to request their agreement and validation of the modifications made to the instrument. As a result, the professionals responded favorably, and the statistical analysis of the eight questions was carried out by means of Cronbach’s alpha test, reaching a value of 0.96, which ratifies the reliability of the instrument.
As for the dimensions contemplated in the instrument, these were dental treatment dimension, defined as the sum of diagnostic, preventive, and restorative services provided in the oral cavity to meet the needs of a patient. This was organized into three levels according to the degree of difficulty required to be performed, with values of one for low complexity treatments, two points for medium-complexity treatments and four points for high-complexity treatments. The group of treatments comprising each dimension is specified as follows:
Low complexity: fluoride, prophylaxis, sealants, atraumatic restorative technique, simple exodontia, scaling, simple restoration, uniradicular endodontics, tenon, and crown. Medium complexity: semi-complex exodontia, scaling and root planing, removable prostheses, complex restorations, multi-root root canals, fixed prostheses (more than 2 pieces), total prostheses, occlusal splints, and teeth whitening. High complexity: complex exodontics, bone remodeling, periodontal flaps, abscess debridement, oral cavity biopsies, implants, orthodontics, endodontic retreatment, periodontal surgery, and orthognathic surgery.
There are three additional considerations that must be evaluated and included in the total sum:
CD dimension: If the patient presents CD, two points are attributed, whereas, in the absence of CD, zero points are awarded. The breakdown of CD was performed according to ICD-11,
13
where conditions are classified by systems and not by single diseases. No additional points were assigned in the case of patients presenting more than one CD. Pharmacological treatment dimension: It was considered whether the patient has medication currently prescribed, assigning a score of two points if he/she receives it and zero points if he/she does not. No additional points were assigned in the case of patients taking more than one drug for their pharmacological treatment. Patient behavior dimension: Frankl’s scale
14
was used as a reference. Following what was previously established, the patient was considered a collaborator when he/she was type three or four according to Frankl’s scale, while he/she was classified as non-cooperative when he/she was type one or type two. Thus, a value of zero was indicated when the patient was a collaborator and a value of two when he/she was a non-collaborator.
The sum of the four dimensions offers an overall score of up to 10 points, so ranges were established for these, considering the degree of complexity.
Low complexity (1–3 points): This level accepts dental management by a practitioner with little or very limited experience in the care of CD patients.
Medium complexity (4–5 points): This level contemplates professionals with basic and moderate levels of knowledge and management of CD patients.
High complexity (6–10 points): This level contemplates professionals with more complete and advanced knowledge in the management of patients with CD.
Statistical Analysis
The information contained in the database was processed in an Excel spreadsheet; subsequently, statistical analysis was performed, starting by obtaining the relative and absolute frequencies of the qualitative variables. Then, a bivariate analysis was performed using the Chi-square test to find possible associations between variables. Finally, a Poisson linear regression was performed to determine crude (PR) and adjusted prevalence ratios (aPR), with the variables showing associations. The study considered a confidence level of 95% and a p < .05 value. Finally, to determine whether the covariates presented multicollinearity bias, the variance inflation factor test was performed, and the results showed values of less than ten; consequently, it was not necessary to eliminate any of the variables. The statistical program used was STATA 15.0.
Ethics
The study was developed after receiving the approval of the Institutional Ethics Committee of UPCH (CIE-UPCH) SIDISI code N° 201950. It should be mentioned that the confidentiality of all participants was guaranteed since all records were coded.
Results
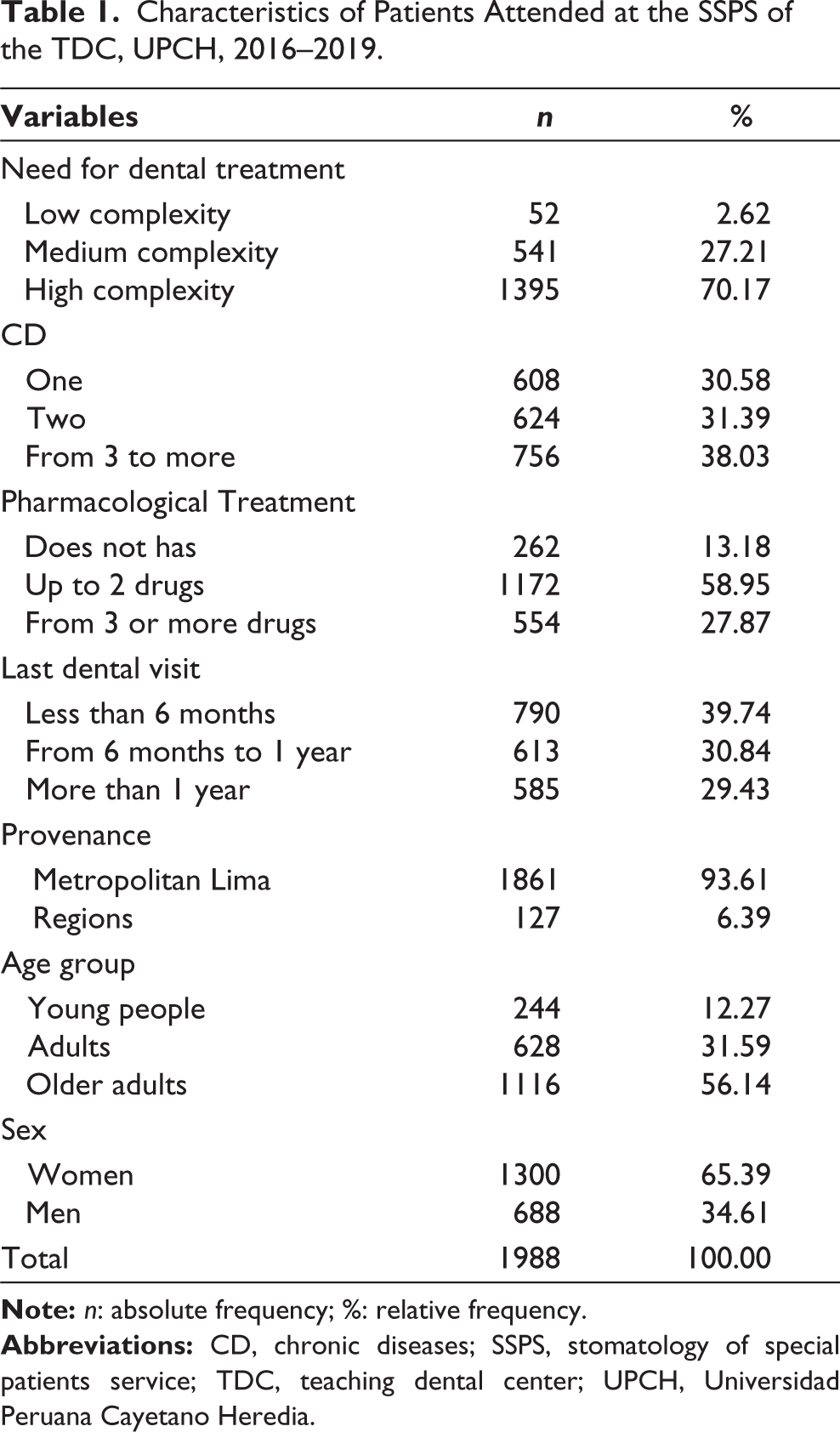
The total study sample consisted of 1988 digital medical records from the TDC. The need for low-complexity dental treatment was present in 2.62% (n = 52) of patients, moderate-complexity in 27.21% (n = 541) of patients, and high-complexity in 70.17% (n = 1395) of patients. In relation to CD, 30.58% (n = 608) had one, 31.39% (n = 624) had two, and 38.03% (n = 756) had three or more. According to pharmacological treatment, 13.18% (n = 262) of patients did not take one, 58.95% (n = 1172) reported taking up to two drugs, and 27.87% (n = 554) took three or more. Regarding the last visit to the dentist, 39.74% (n = 790) reported having attended in a period of less than 6 months, 30.84% (n = 613) from 6 months to 1 year, and 29.43% (n = 585) more than 1 year. In relation to sociodemographic characteristics, 93.61% (n = 1861) came from Metropolitan Lima and 6.39% (n = 127) from the regions. According to age groups, 12.27% (n = 244) belonged to the youth group, 31.59% (n = 628%) to adults, and 56.14% (n = 1116) to older adults. According to sex, 65.39% (n = 1300) were women and 34.61% (n = 688) were men (Table 1).
Characteristics of Patients Attended at the SSPS of the TDC, UPCH, 2016–2019.
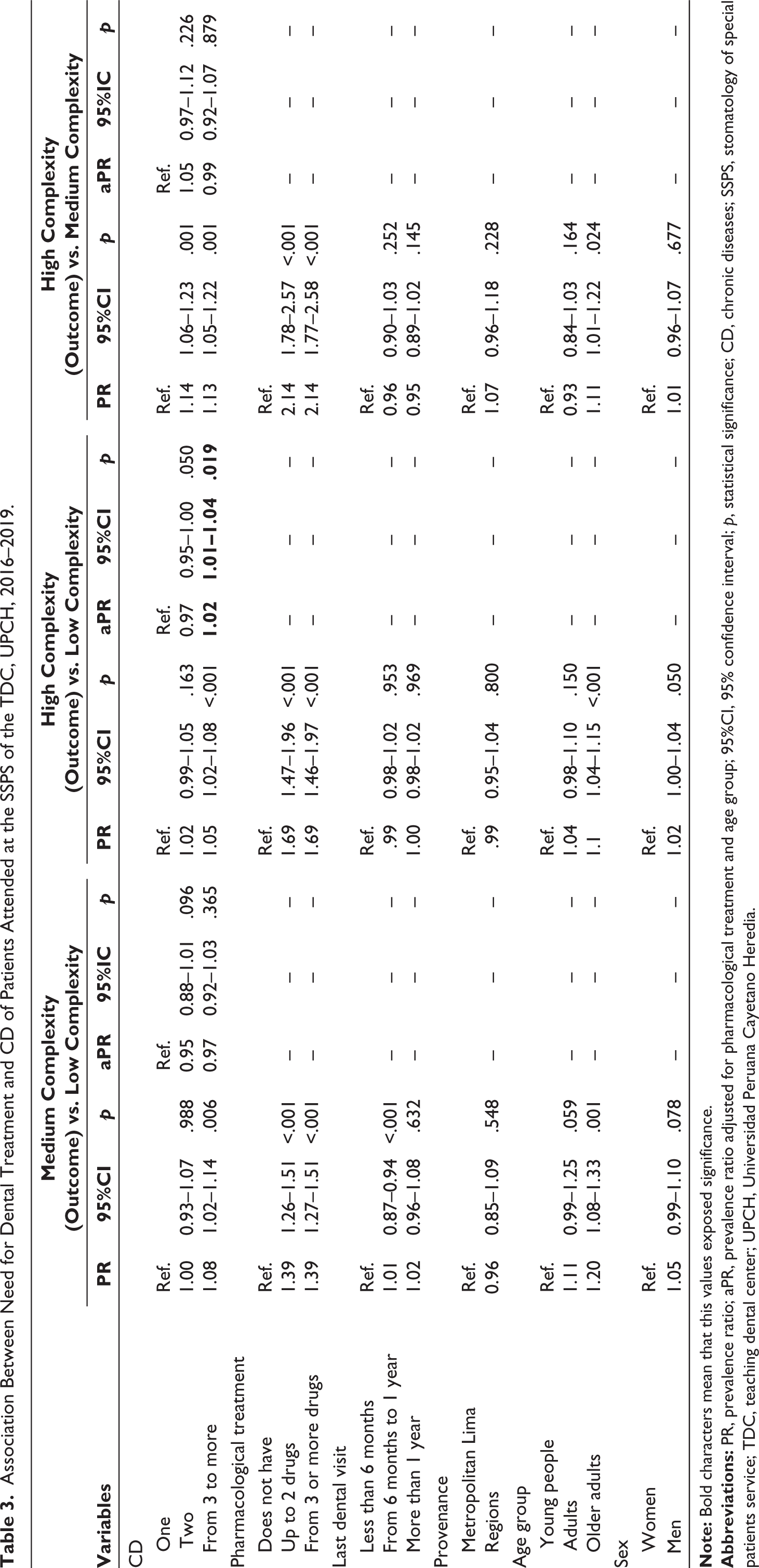
In the bivariate analysis, there was an association between the presence of more than three CD and the necessity for highly complex dental treatment, and these differences were statistically significant (p < .001). Likewise, there was an association between those who consumed more than two drugs and the need for highly complex dental treatment, compared to those who did not have pharmacological treatment. Additionally, there was an evident association in the older adult group (Table 2). In the multivariate analysis, due to the presence of three to more CD and the necessity for high-complexity vs. low-complexity treatment, an aPR of 1.02 (95% confidence interval (95%CI): 1.01–1.04; p = .019) was obtained (Table 3).
Need for Dental Treatment According to Characteristics of Patients Attended at the SSPS of the TDC, UPCH, 2016–2019.
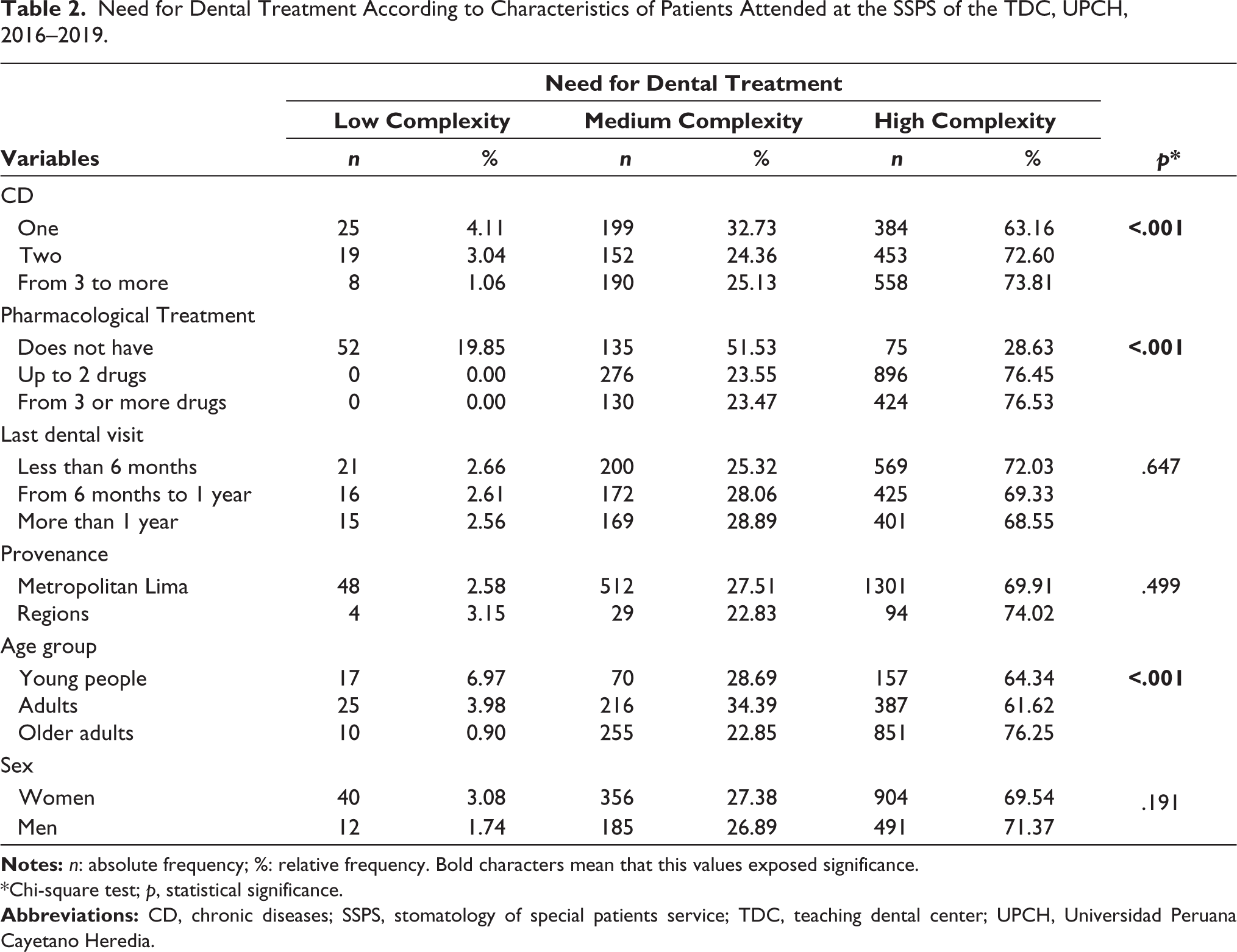
*Chi-square test; p, statistical significance.
Association Between Need for Dental Treatment and CD of Patients Attended at the SSPS of the TDC, UPCH, 2016–2019.
Discussion
It is complex to determine the need for dental treatment when the individual has multiple CDs, despite the evident association between these and the existence of oral pathologies. 15 In addition, multiple studies report a high need for dental treatment in populations of adults and the elderly with CD, particularly when they face hospital treatment. 16 It should be mentioned that some physical or cognitive conditions can play a limiting role in the maintenance of adequate oral health; similarly, oral health status can influence general health and/or exacerbate pre-existing CD.17,18 In Peru, more than two-thirds of the population suffers from CD, with a higher prevalence in women, according to the National Institute of Statistics and Informatics in 2020. 19
It was observed in this research that the percentage of women with CD is higher than that of men, and it is important to highlight that more than one disease was identified in an individual and that the consumption of more than one medication. Likewise, there was evidence of an association between CD, pharmacological treatment, age group, and the need for highly complex dental treatment. It is well known that during the course of life there is a cumulative and irreversible effect of diseases, which affects the quality of life of individuals and could lead to the need for more complex treatments. 20 This scenario has a direct impact on the fact that, before a dental treatment, possible effects and pharmacological interactions, the presence of multimorbidities, and considerations for the patient’s approach should be considered. 20
In reference to oral healthcare, this research broke down the need for dental treatment into dimensions due to the particularity of caring for a patient with chronic health pathologies, where the following were considered: the required dental treatment, the existence of CD or the coexistence of multiple diseases, the pharmacological treatment received, and the patient’s behavior. This made it possible to identify that most of them had a need for highly complex dental treatment. In addition, the most common clinical findings in older adults were the absence of teeth and severe periodontal deterioration. It is understood that this situation has a direct impact on the functionality and biopsychosocial well-being of the individual, affecting healthy aging.21,22
Of the entire population evaluated, the majority attended dental consultations at least once during the year, with women being the predominant group. WHO establishes that access to dental services at the international level is low, which is associated with aspects such as economic barriers, limited human health resources, and precarious and inefficient infrastructure. 9 Zhang et al. state that attendance to dental services in patients with diabetes, regardless of whether for prevention and/or treatment, was lower compared to those who did not have diabetes; 23 similarly, people with chronic obstructive pulmonary disease, heart pathologies, or stroke. 24 Likewise, in a study of hospitalized older Argentinian adults over 60 years of age, it was observed that only 16% reported having seen a dentist in the last 6 months prior to hospitalization. 17
Bethel et al. 25 and Spinler et al. 26 state that attendance at dental services decreased with age. In addition, the latter author mentions that people with some type of disability, physical mobility problems, or psychiatric illness face greater difficulty attending these services. 27 Other studies of the elderly indicate that there are additional factors beyond having health insurance, such as gender, income, and educational level. At the national level, about a quarter of Peruvian elderly used dental health services during 6 months prior to their participation in the 2018 Demographic and Family Health Survey (ENDES), which indicates a reduction compared to previous years. In addition, it is mentioned that 2 out of 10 elderly people do not have health insurance. 28
In the present study, more than two-thirds of the population evaluated reported two or more CD; coincidentally, Maxwell et al. report similar results in their research. 29 It should be mentioned that multimorbidity is the coexistence of two or more diseases in an individual; 16 in addition, it has been identified that the coexistence of multiple CD increases with age.30–33 On the contrary, the interaction between CD and dental health is evident. According to the pharmacological treatment, 86.86% indicated consuming two or more drugs; hence, the definition of polypharmacy is derived, which refers to the use of multiple drugs 29 without specifying an exact amount. It is known that the consumption of multiple drugs brings with it events such as drug interactions, increased risk of falls, allergic reactions to medications, cognitive deterioration, poor adherence to treatment, and inadequate nutritional status. 34
In addition, this research showed that more than 80% of men and women receive some form of pharmacological treatment. In contrast, Stafford et al. report that this situation is more common in men with more than one pre-existing CD. In addition, it should be considered that there are differences according to sex and age in relation to the effects that can be caused by the use of various drugs. 35 In addition, Maxwell et al. reported an increase in polypharmacy in men of all ages with multiple CD. 29 According to the prevalence of multimorbidities, Lee et al. reported a predominance of men compared to women, and differences between ethnic groups were also observed.
In primary care, hypertension, hyperlipidemia, and depression are documented as the most prevalent pathologies in the adult population. 36 From this, it is reported that patients with diabetes have weak preventive behaviors compared to those who do not present this disease and are two to three times more likely to develop periodontal disease. 25 For the present investigation, both sexes presented a higher prevalence of diseases of the circulatory system, followed by those of the endocrinological system. This information corresponds to that published in the first quarter of 2020 in the report of the National Household Survey applied in Peru, where the most prevalent CD were arthritis, hypertension, asthma, rheumatism, diabetes, and tuberculosis, among others. 37
According to life course, the group with the highest representation in the study was the elderly, most of whom were women. It is worth noting that older women represent 13.2% of the total Peruvian female population and older men, 12.2%. Some 12.7% are over 60 years old, and 15.6% are octogenarians. 19 Some authors state that the amount of damage accumulated over time in the older adult group implies the need for very complex treatments, stating that a limited group of this age group considers tooth extraction as an option compared to the past, 38 which reflects the acceptance of more conservative alternatives, seeking functionality and esthetics regardless of their age. 39
It was found that the consideration of a high-complexity vs. low-complexity dental treatment was influenced by the presence of more than 3 CD; likewise, when adjustments were made to the model, the same association was found, although the impact decreased due to the immersion of other variables. Tahani et al. mention that tooth loss, systemic diseases, and medications are factors that increase the complexity of treatment. 40 The association of these variables implies that the dentist should prioritize a comprehensive and systematized assessment to identify the real need for treatment, highlighting the importance of the minimum competencies that every professional who attends this population group should acquire.18,26
In relation to the aforementioned, the stomatology of special patients is defined as a dental specialty aimed at the care of patients with special needs, including those with physical and mental disabilities. 41 To address these patients, the presence of specialized oral health care providers is a requirement, which helps to alleviate problems such as accessibility barriers. It is therefore necessary to promote public policies that promote equitable care for these users, ensuring that the dentist is part of the basic health team and engaging in interdisciplinary work to ensure the welfare of patients and improve the quality of their care.
One of the limitations of the study was the loss of records during data cleaning. In addition, the paucity of previous scientific evidence that described the studied phenomenon was noted. On the contrary, the records from the clinical histories were not digital, so the entire process of collecting and evaluating this tool was manual. Since this is a cross-sectional study, this research does not have the capacity to establish causal relationships. However, to avoid multicollinearity bias, the variance inflation factor test was used for the covariates analyzed. Nevertheless, it is recommended that the results of this study be interpreted with caution and not generalized.
This research can conclude that there was an association between having a CD, the use of pharmacological treatment, age, and the need for dental treatment in the medical records evaluated. In addition, an association was found between the presence of three or more CDs, consumption of two or more drugs, and the need for highly complex dental treatment in the group of older adults. There is a positive association between the presence of three or more CD, and the need for high-complexity dental treatment compared to low-complexity dental treatment, adjusted for use of pharmacological treatment and age.
The importance of the study lies in the possibility of comprehensively assessing the treatment required by the patient from an integral perspective, which not only assesses dental health indicators but also general health conditions, such as the presence of CD, for which specialized care is necessary. By being able to identify the real dental treatment requirement that fits the patient’s needs, it is possible to work in conjunction with various dental or medical areas where the instrument used for this research is precise and stands out for its easy application, being covered by the competencies of the professional in charge.
Footnotes
Acknowledgements
We would like to thank all the participants involved in this study.
Authors’ Contributions
All the authors were involved in study conception, data collection, data acquisition and analysis, data interpretation, manuscript writing, and review and editing. All the authors read and approved the final version of the manuscript for publication.
Data Availability Statement
The data analyzed in this study are available upon request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study received approval of the Institutional Ethics Committee of UPCH (CIE-UPCH) SIDISI code no. 201950.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The authors certify that all the participants provided their written consent to participate in the research and have the analyzed data published.
Reprint Statement
Reprints are not available from the authors.