
Abstract
Introduction:
There are concerns that the COVID-19 pandemic exacerbated oral care inequities globally. In Sweden, declines in oral care utilization, particularly among certain regions and public clinics, suggest disproportionate impacts across population groups. Yet, the effects of the pandemic on oral care equity in Sweden remain unexplored, highlighting a critical gap in evidence to guide ongoing equity initiatives and strengthen future pandemic preparedness.
Objective:
To examine changes in unmet oral care needs (UOCNs) inequities among Swedish adults before and during the pandemic, following an intersectional approach.
Methods:
Data came from the 2018 and 2021 waves of a national survey, including 31,493 adults. Single-indicator and intersectional inequities were examined by intersectional analysis of individual heterogeneity and discriminatory accuracy across 48 groups defined by gender, age, education, income, and immigrant status.
Results:
The prevalence of UOCNs increased during the pandemic. Notable shifts in single-indicator inequities included a decrease among immigrants but an increase among older adults. Modest increases were observed among individuals with low education and low income, while inequities decreased slightly for men and younger adults. The intersectional analysis revealed that inequities increased primarily among socially advantaged older adults, whereas decreases were more evident among immigrants and younger individuals facing other forms of social disadvantage. The discriminatory accuracy of both the single-indicator and intersectional inequities decreased during the pandemic, although intersectional models consistently showed slightly better accuracy.
Conclusions:
Patterns of UOCNs inequities shifted during the pandemic, with increased intersectional inequities among socially privileged older adults and decreased inequities among immigrants. These findings may reflect Sweden’s unique pandemic context, which emphasized individual responsibility over restrictive measures and may have influenced how people approached health-related behaviors, including seeking oral care.
Knowledge transference statement:
The reconfiguration of inequities in unmet oral care needs during the pandemic might be explained by the unique response in Sweden, which adopted less restrictive measures. These findings highlight the importance of tailoring future pandemic strategies to ensure equitable oral care access, that is, targeted interventions addressing the needs and challenges of both medically vulnerable populations, such as the elderly, and socially marginalized groups, such as immigrants facing structural disadvantages.
Keywords
Introduction
There are concerns that the COVID-19 pandemic contributed to exacerbating global oral care inequities (i.e., avoidable and unfair differences in access to oral care services between population groups) (Watt 2020). In Europe, these concerns are supported by evidence of increased inequities in the utilization of general health care services during the pandemic (González-Touya et al. 2021; Maddock et al. 2022; Frey et al. 2024). However, the specific impacts on oral care equity remain underexplored.
Although European studies have documented a marked decline in routine oral care utilization during the pandemic (Walter et al. 2021; Stennett and Tsakos 2022), few studies from the United Kingdom have examined oral care inequities over time (Brown et al. 2022; Aminu et al. 2023; O’Connor et al. 2023). Two of these studies observed a temporary reduction in disparities related to social deprivation, which appeared to return to prepandemic levels by 2022 (Aminu et al. 2023; O’Connor et al. 2023). However, these studies use composite area-level deprivation indices, which limit the assessment of single or intersecting social indicators. Another study focusing on age- and income-related inequities identified older pensioners with financial difficulties as the group most affected by increased inequities in oral care access (Brown et al. 2022). Additional research from other rich countries supports these findings. In the United States, increased disparities were associated with public insurance and residence in underserved areas (Choi et al. 2021). In Japan, income-related disparities in unmet oral care needs (UOCNs) were identified, although only during the pandemic (Koyama et al. 2022).
Despite their limitations, findings from the UK studies likely reflect the oral care situation in most European countries, given the widespread implementation of restrictive measures, including lockdowns, enforced quarantines, and temporary suspension of oral care services during the pandemic’s first wave (Coulthard 2020). In contrast, Sweden adopted a singular strategy focused on recommendations and citizens’ responsibility (detailed in Appendix 1), which may have influenced oral care outcomes differently. This approach sparked considerable debate and raised concerns about its impact on vulnerable groups, particularly older adults and immigrants (Rambaree and Nässén 2020). Between the first confirmed COVID-19 case on 31 January 2020 and March 2022, Sweden reported 16,645 COVID-19 deaths (Socialstyrelsen 2022), showing the highest mortality among the Nordic countries (Burström et al. 2025). Older age was the greatest risk factor for COVID-19 mortality (Drefahl et al. 2020), while immigrant status significantly increased the risk of infection, severe outcomes, and death, after adjusting for confounders (Folkhälsomyndigheten 2021b).
Regarding oral care, initial recommendations deferred routine oral care for older adults and other high-risk groups, while no recommendations were provided for other age groups, beyond protocols for symptomatic individuals and urgent care for confirmed or suspected cases (Socialstyrelsen 2020). Meanwhile, general recommendations emphasized avoiding unnecessary health care visits, self-isolation when symptomatic, physical distancing, and personal responsibility (Ludvigsson 2020). Governmental reports indicated that during the pandemic’s early months, utilization of oral care services declined more pronouncedly in specific regions and public facilities, suggesting disproportionate effects on certain population groups (Socialstyrelsen 2020).
The aim of this study is to employ an intersectional approach to examine changes in UOCNs inequities in the Swedish adult population before and early after the pandemic’s onset. Intersectionality-based research recognizes that multiple indicators of social position (e.g., income, immigration background) interlock with structural factors (e.g., poverty, nationality-based discrimination) in complex ways to produce health inequities (Muirhead et al. 2020). Thereby, it provides a more comprehensive understanding of inequities than traditional approaches that examine social indicators separately (Merlo et al. 2023). Prior intersectionality-based Swedish research has reported substantial UOCNs intersectional inequities over the past 2 decades (Anticona et al. 2023), with financial-related UOCNs increasing despite partial subsidies intended to promote equity (Anticona et al. 2024). However, no study has yet explored how intersectional inequities in oral care evolved during the pandemic, either in Sweden or globally.
This study hypothesizes that the pandemic disruptions exacerbated existing oral care inequities in Sweden, albeit with distinctive patterns compared to other rich countries, due to the unique pandemic approach. Evidence on the pandemic’s impact on oral care inequities is critically important both locally and globally. Locally, it can support the current policy process to advance equity (Swedish Government Official Reports 2021). Globally, the Swedish case could serve as an informative example for future pandemic strategies that aim to maintain equitable oral care with less restrictive measures.
Methods
Design and Ethics
This repeated cross-sectional study analyzed data from the 2018 and 2021 waves of the Health on Equal Terms (HET) surveys, representing the years before and during the pandemic, respectively. The Public Health Agency of Sweden conducts the HET survey annually to collect self-reported information on general and oral health, health care utilization, lifestyle, and living conditions from an unbounded random sample of individuals aged 16 to 84 y (the sampling strategy is summarized in Appendix 2). Data collection occurred between February–June 2018 and February–May 2021, with response rates of 42.1% and 44.5%, respectively. Survey data were linked to sociodemographic information from population registers. The initial sample included 34,334 respondents. Individuals aged 16 to 23 y (n = 2,368 [6.9%]) were excluded due to their eligibility for free oral care, which reduces financial barriers to UOCNs. Respondents with missing information on the outcomes or explanatory variables were also excluded (n = 473 [1.4%]). The final analytical sample comprised N = 31,493 individuals (15,332 in 2018 and 16,161 in 2021), representing 91.7% of all individuals aged ≥24 y. This study was approved by the Swedish Ethical Review Authority (approval no. 2021-02398) and complies with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.
Variables
UOCNs were the study outcome, representing the perceived oral care need (expressed as dental care need in the survey) that was left untreated and were assessed using the following question: “During the last three months, have you believed yourself to be in need of dental care but refrained from seeking care?” Respondents answering yes were coded as having UOCNs (coding = 1; otherwise 0).
The explanatory variables were 5 indicators of social position, categorized and coded as follows: gender, defined by the proxy variable of sex (man = 1; woman = 0); age (65–84 y = 2; 24–44 y = 1 and 45–64 y = 0); education (low = 1 [<3 y of high school]; high = 0 [≥3 y of high school]); immigrant status, determined as having immigrated to Sweden at any point in life (immigrant = 1; native = 0); and individual disposable income (low = 1 [<median]; high = 0 [≥median]), adjusted for inflation, using official consumer price indices. All categories were subsequently cross classified into a multicategorical variable comprising 48 mutually exclusive intersectional strata. The reference stratum consisted of native women aged 45–64 y, with both high education and income. Rather than selecting reference stratum presumed to be most privileged, this stratum was selected as it displayed the largest and most stable sample sizes and most consistent UOCNs prevalence over the study period. No covariates were included in the models to avoid overadjustment bias from controlling for potential mediators. While residual confounding is a known limitation in observational studies, adjusting for covariates on the causal pathway—particularly among intersecting social indicators—may introduce bias and obscure the key effects.
Analysis
The intersectionality-informed analysis of individual heterogeneity and discriminatory accuracy (AIHDA) was used as the analytical framework. AIHDA surpasses traditional methods for examining inequities by simultaneously assessing both average differences in health outcomes across population groups and the total individual variance within these groups. The individual heterogeneity component uses regression models to analyze health outcomes among individuals nested within a matrix defined by the intersection of several social indicators (intersectional strata). The discriminatory accuracy (DA) component evaluates the extent to which these indicators can distinguish between individuals with and without the outcome of interest (Merlo et al. 2023).
Group-average differences in UOCNs were estimated using additive models (generalized linear models with binomial family and identity link) to quantify absolute inequities and additive-scale interactions. Additive-scale interactions align more closely with social causation and are more relevant to population health than multiplicative-scale interactions (Bauer 2014). Accordingly, additive scales are recommended for intersectionality-based studies using regression with interaction terms (Guan et al. 2021).
Single-indicator inequities for each year were estimated as prevalence differences (PDs) with 95% confidence intervals (CIs) of UOCNs in a crude model (including each of the social indicators separately) and an adjusted model (including all other indicators). Each indicator was treated as an independent variable, using the following reference categories: women, high education, 45 to 64 y, high income, and Sweden-born. Intersectional inequities were estimated using a model that included the multicategorical variable comprising 48 strata, rather than individual social indicators.
Between-year changes in inequities were estimated for each social indicator and intersectional stratum, expressed as prevalence difference differences (PDDs) with CI. For social indicators, a crude model examined the interaction between year and each indicator:
To illustrate overall patterns across all intersectional strata, the strata were further classified based on the change in PD before versus during the pandemic: little/no change (<2 percentage point [pp] change) and decreased and increased inequities (≥2 pp negative or positive change). Because of the cross-classification, several strata contained few individuals (7 strata with n < 50 in both 2018 and 2021). Therefore, 1 stratum (n = 8 in 2018 and n = 2 in 2021) could not be classified and was excluded from the results, and a few strata (k = 7) reported statistically significant changes. Importantly, intersectionality-based research emphasizes identifying strata with favorable and unfavorable health estimates for further targeted policy, rather than focusing solely on statistical significance (Mahendran et al. 2022).
DA was assessed annually by calculating the area under the receiver operating characteristic curve (AUC) expressed as a prevalence ratio and 95% CI of UOCNs in 2 models. Model 1 considered single-indicator inequities, and model 2 replaced the indicators with the multicategorical variable comprising 48 strata. Further results were classified as follows: absent or very small (AUC 0.5–0.6), moderate (AUC >0.6–≤0.7), large (AUC >0.7–≤0.8), and very large (AUC >0.8) (Axelsson Fisk et al. 2021). The change in AUC value (ΔAUC) quantified the improvement in DA when intersectional strata replaced single indicators. DA between years was compared using the AUC equality test (Cleves 2002).
Given the moderate survey response rates of 42.1% (2018) and 44.5% (2021), selection bias related to the explanatory variables and the outcome was assessed using quantitative bias analysis (Fox et al. 2021) (Appendix 3). All analyses were conducted using STATA 17.0.
Results
Population Characteristics
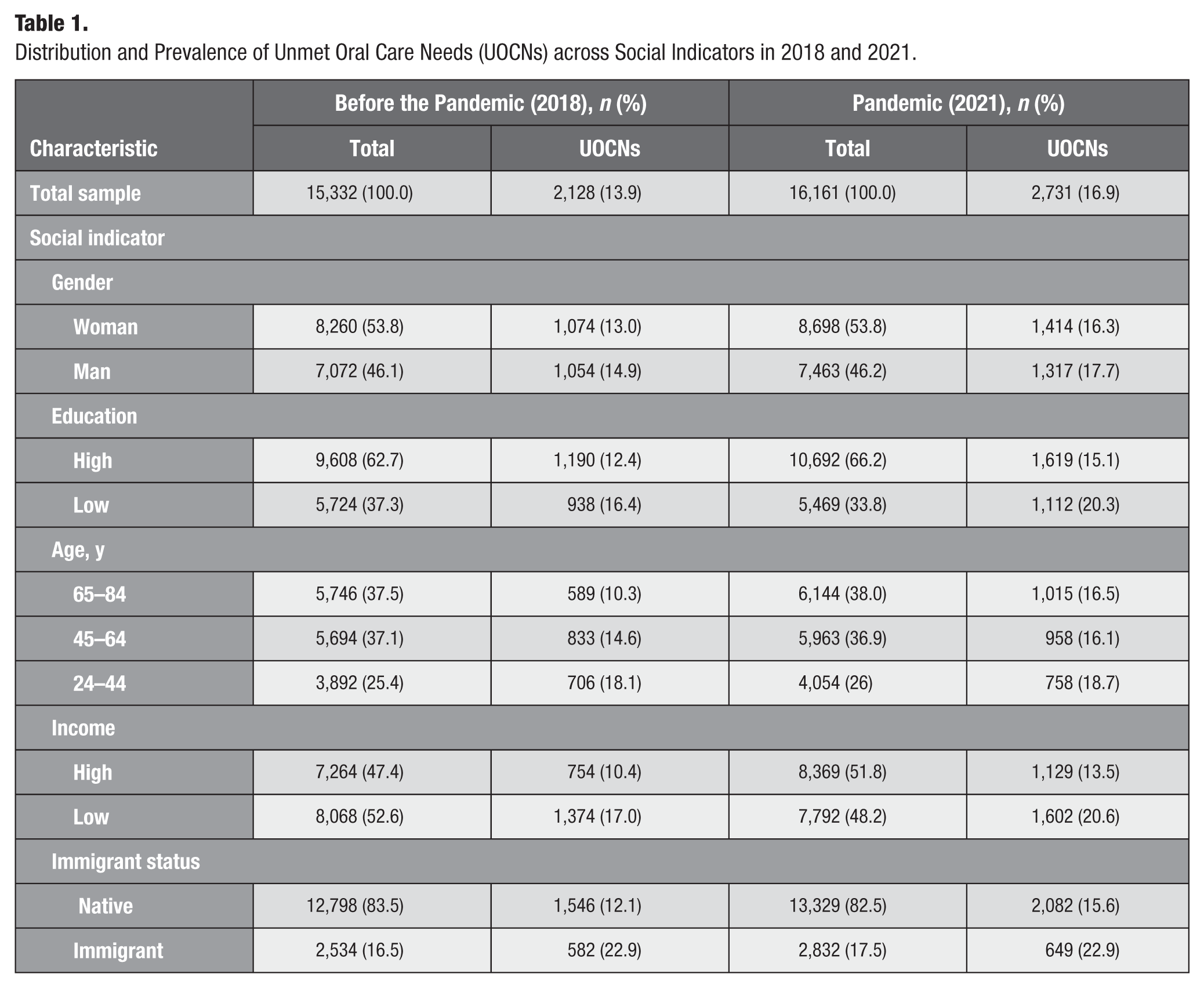
The samples from both years were comparable in terms of the relative distribution of social indicators. The overall UOCNs prevalence increased following the pandemic, but the social patterning remained similar, with a numerically higher prevalence among participants with low education, low income, younger age, and immigrant status, but comparable prevalence between gender categories (Table 1).
Distribution and Prevalence of Unmet Oral Care Needs (UOCNs) across Social Indicators in 2018 and 2021.
Single-Indicator UOCNs Inequities
Absolute UOCNs inequities by single indicators are reported in Table 2. Adjusted models for 2018 confirmed the descriptive patterns, showing the largest UOCNs inequities for immigrant status (9.1 pp higher UOCNs prevalence among immigrants), followed by income (6.1 pp higher among low-income individuals), age (5.8 pp lower and 3.8 pp higher among individuals aged 65–84 and 24–44 y, respectively), education (4.9 pp higher among low-educated individuals), and gender (2.5 pp higher among men).
Absolute Inequities in Unmet Oral Care Needs by Single Social Indicators in Crude and Adjusted Models, 2018 (n = 15,332) and 2021 (n = 16,161).
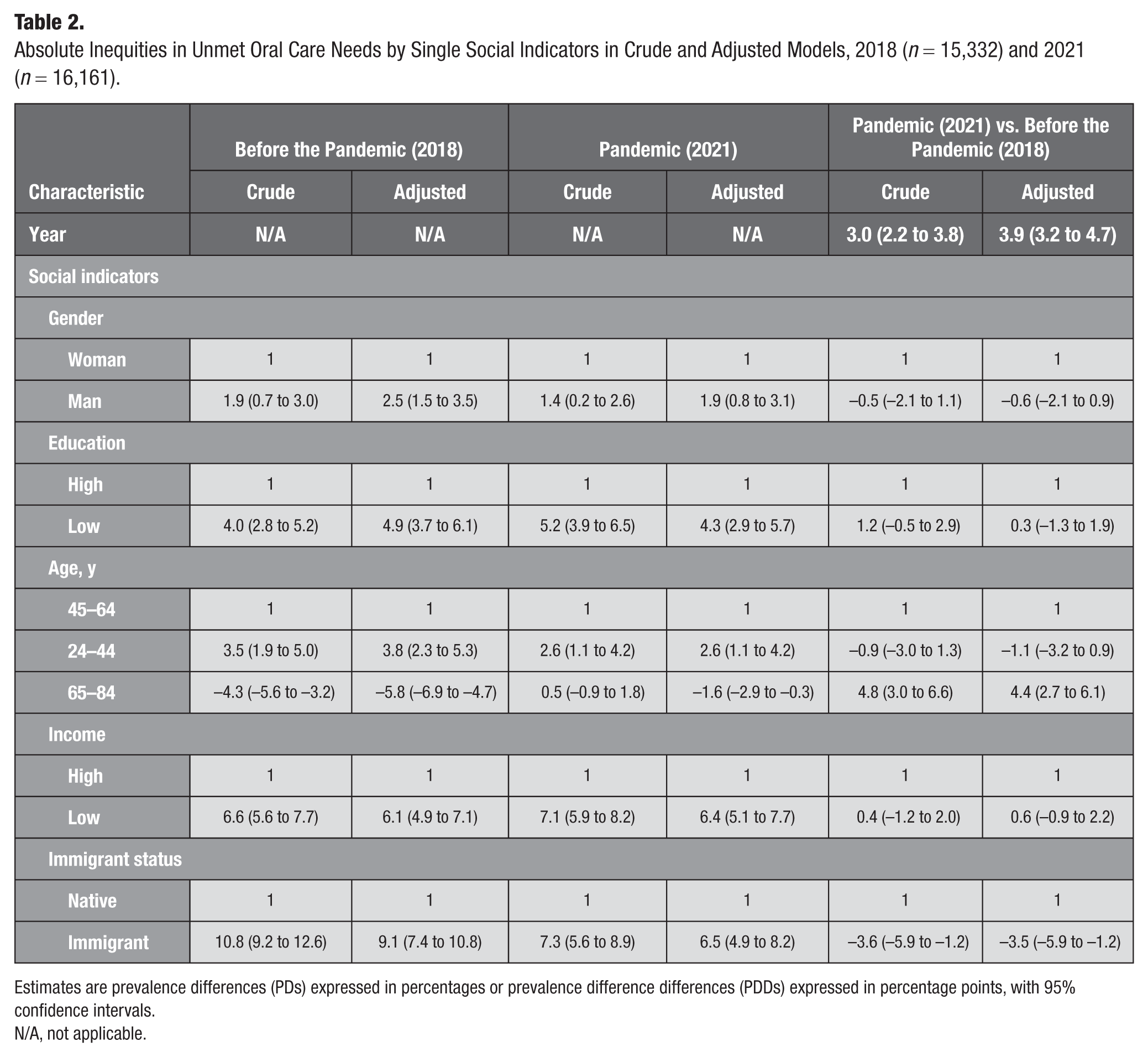
Estimates are prevalence differences (PDs) expressed in percentages or prevalence difference differences (PDDs) expressed in percentage points, with 95% confidence intervals.
N/A, not applicable.
During the pandemic, an increase in the overall UOCNs prevalence (3.9 pp higher) was observed alongside a reconfiguration of inequities. The gap increased 4.4 pp for the oldest group but decreased 3.5 pp for immigrants. Smaller changes were observed for the youngest age group (1.1 pp lower), men (0.6 pp lower), and individuals with low education (0.3 pp higher) and low income (0.6 pp higher).
The bias analysis, assuming a 10-pp selection bias by the outcome, showed larger adjusted estimates for all indicators except age in 2018 (Appendix 3). Furthermore, age group estimates shifted similarly in both years, with older groups becoming more disadvantaged. The impact of selection bias was comparable for both years.
Intersectional UOCNs Inequities
The distribution, prevalence of UOCNs, and inequities of each of the 48 intersectional strata are shown in Appendix Table 2 and the Figure. The UOCNs prevalence varied substantially across strata and years (3.2%–44.3% before and 9.1%–55.6% during the pandemic).
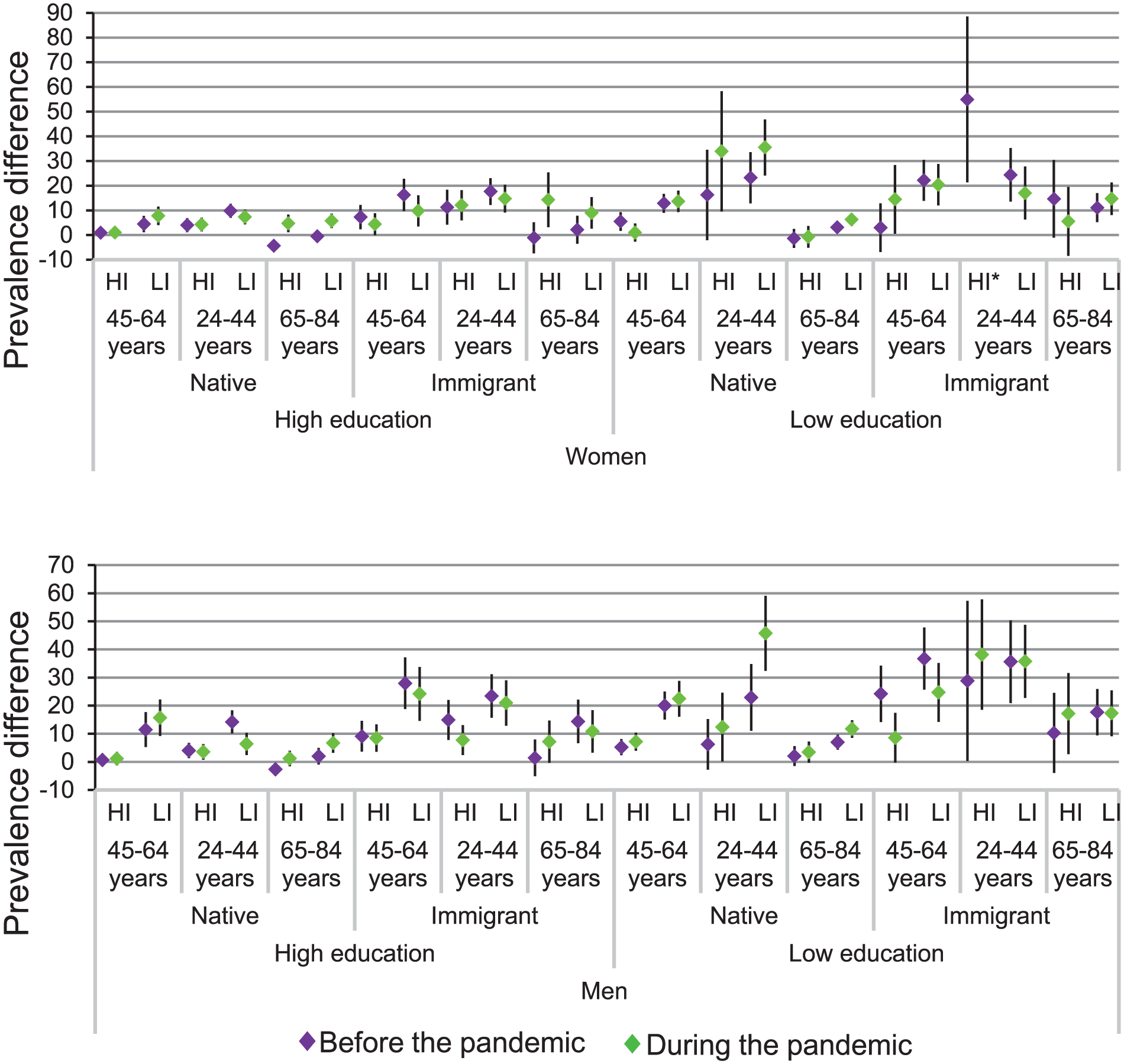
Absolute inequities of unmet oral care needs for 48 intersectional strata before and during the pandemic. Estimates are prevalence difference differences and 95% confidence intervals. The reference stratum consists of native women aged 45 to 64 y with high education and high income. HI, high income; LI, low income.
Before the pandemic, the largest gaps in the UOCNs risk were observed among 4 socially disadvantaged strata of immigrant men under 65 y, particularly those aged 45 to 64 and 24 to 44 y with both low income and education, showing a 36.7-pp and 35.6-pp higher UOCNs prevalence, respectively, compared to the reference stratum. Additional high-risk strata included men aged 24 to 44 y with high income but low education (28.8 pp higher) and those aged 45 to 64 y with low income but high education (27.9 pp higher).
Conversely, the lowest UOCNs risk (<3 pp), even lower than the reference stratum, was found among older adults, including Sweden-born women and men with high income and either high or low education (–2.6 pp, –1.3pp for women and –4.3 pp, 2.1 pp for men), as well as immigrant women and men with both high income and education (–1.1 pp and 1.4 pp). Small gaps were also found among younger strata with other social privileges, for example, Sweden-born men aged 45 to 64 y with both high education and income (0.7 pp). Notably, old age did not consistently result in lower risk, particularly among older men with additional disadvantage. For example, 2 strata of immigrant men with either high income or education exhibited a >10-pp higher UOCNs prevalence than the reference stratum, and 1 stratum of Sweden-born men with both low income and education reported a 7-pp higher UOCNs prevalence.
Between-year comparisons revealed a 2.2-pp increase in the overall UOCNs prevalence during the pandemic. There was a slight tendency toward increased inequities: 20 strata displayed increased, 15 decreased, and 11 little or unchanged inequities (Appendix Table 2 and Fig.). Six strata of socially advantaged older adults who had the lowest UOCNs risk before the pandemic exhibited increased inequities. These included immigrant women and Sweden-born men with both high income and education (15.4-pp and 9.1-pp increase, respectively), as well as Sweden-born men and women with high education and either high income (9.1-pp and 3.8-pp increase, respectively) or low income (6.3-pp and 4.7-pp increase, respectively). Nuances to this general pattern included older-age strata showing little or unchanged inequities (<2 pp), including Sweden-born men and women with high income and low education, and younger-age Sweden-born strata showing notable increased inequities (>9 pp), including men with both low education and income, as well as women with low education regardless of income. Less notable increased inequities (<5 pp) were observed among Sweden-born men and women aged 45 to 64 y, with either both low education and income or high education but low income.
Conversely, decreased inequities were primarily observed among men under 65 y, including immigrant men aged 45 to 64 y with high income and low education (15.6-pp decrease) and Sweden-born aged 24 to 44 y with low income and high education (7.9-pp decrease). Other notable reductions (PDD >9) were found among immigrant women and men with low education, either aged 45 to 64 y with low income or 65 to 84 y with high income. The most substantial decreases occurred in strata with the largest inequities before the pandemic.
Discriminatory Accuracy
The estimates for model 1 (separate indicators) and model 2 (intersectional strata) were predominantly moderate (AUC 0.65–0.66 in 2018 and 0.60–0.61 in 2021), with a marginal difference between them (ΔAUC 0.01 for both years). The DA decreased significantly from before to during the pandemic in both models (Table 3).
Discriminatory Accuracy of Single Indicators and Intersectional Model in 2018 and 2021.
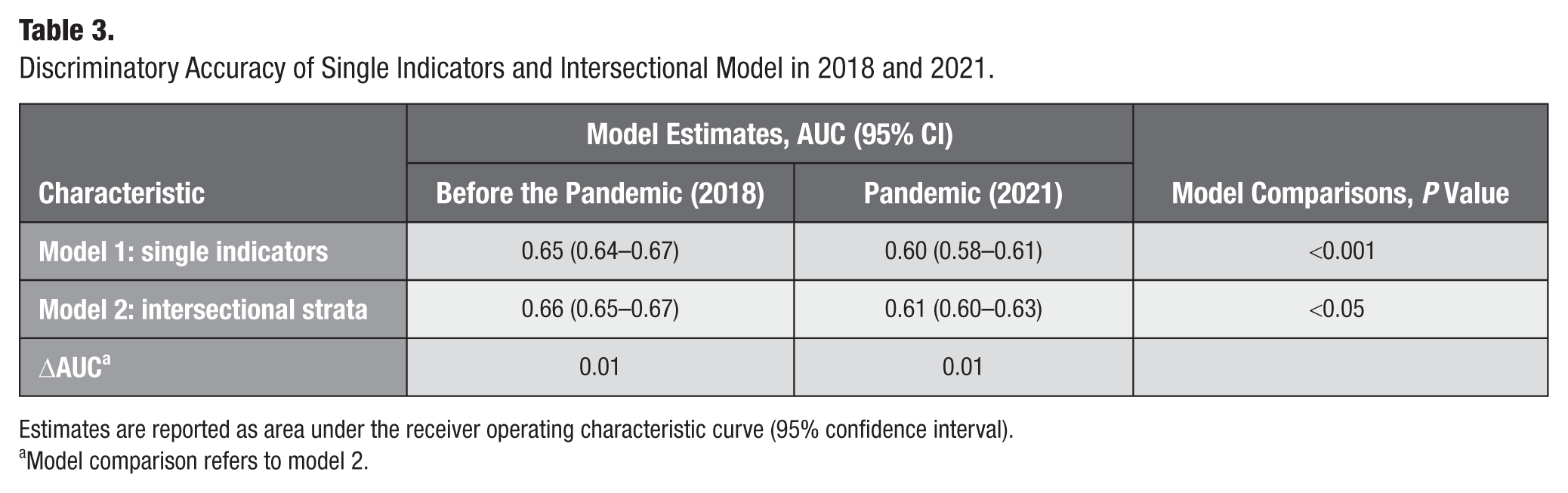
Estimates are reported as area under the receiver operating characteristic curve (95% confidence interval).
Model comparison refers to model 2.
Discussion
This study elucidates considerable UOCNs inequities both before and during the pandemic, with varied patterns of change. Single-indicator inequities shifted significantly during the pandemic, with inequities markedly increasing among older adults, while income- and education-related disparities rose moderately. Conversely, inequities decreased among immigrants and slightly among young adults and men. The intersectional analysis provided further details to this shift in inequities, revealing the most pronounced increases among socially privileged older adults with high education and income, as well as the greatest decreases among younger adults and immigrants with additional disadvantages such as low education and income. An important nuance to these group-average inequities was the reduced DA of single indicators and intersectional strata during the pandemic, suggesting their lower potential to discriminate between those with and without UOCNs.
The single-indicator findings of this study may not be comparable to most prior oral care research due to methodological differences, including the use of indexes compiling several social indicators (Aminu et al. 2023; O’Connor et al. 2023) or the exclusive focus on the pandemic period without a prepandemic comparison (Koyama et al. 2022). An exception is the widening gap in oral care utilization observed among economically disadvantaged older adults in the United Kingdom (Brown et al. 2022), which generally aligns with the results of this study. Although European research on health care inequities could be informative, health care and oral care disparities likely follow distinct patterns and would not be directly comparable (Eurostat 2024). Nonetheless, one of the most salient findings of this study (i.e., the increasing gap among older adults) aligns with evidence of disproportionate declines in health care utilization among the elderly in the Netherlands (Frey et al. 2024) and in the United Kingdom (Maddock et al. 2022). These findings also support results from a national survey showing that during the first wave, over 30% of Swedes older than 69 y refrained from seeking health care, mainly due to transmission risk concerns, compared to less than 20% of individuals under 40 y (Folkhälsomyndigheten 2021a). In contrast, the smaller gap observed among immigrants in this study diverges from previous findings reporting widened health care utilization inequities among immigrants in the Netherlands (Frey et al. 2024).
The intersectional analysis further expanded upon how the interaction of social indicators influenced the risk of experiencing UOCNs before and during the pandemic. The cumulative effect of social disadvantages or advantages on the risk of UOCNs was clearly illustrated before the pandemic. While 4 strata of immigrant men under 65 y with both low income and education exhibited the largest UOCNs inequities, the smallest inequities were observed among privileged strata of Sweden-born older adults with high education and income. Additionally, the contingency of inequities was evident both before and during the pandemic. For example, older age did not protect immigrant men from a high UOCN risk before the pandemic, even in the presence of either high education or income. Moreover, immigrant women exhibited increased inequities during the pandemic if they were older and highly educated, but they displayed decreased inequities if they were young with low education and income. These nuances underscore the value of intersectional approaches in identifying the most vulnerable groups and further understanding the underlying drivers.
The reduced DA of both single indicators and intersectional strata during the pandemic likely reflects the complex and unpredictable impact of the pandemic on the population. Given that the AUC values correspond to a very specific context, which may not be replicable, further examination of the predominantly moderate DA in both years is unlikely to yield meaningful insights for policy development.
Interpretation of the overall findings requires consideration of Sweden’s unique pandemic response, with less stringent measures compared to most countries. The emphasis on individual responsibility was crucial for compliance with public health recommendations (Söderberg et al. 2023), which may be reflected in other health behaviors, such as seeking oral care. In Sweden, significant gaps have been reported in the communication of COVID-19 information by public institutions, particularly in ensuring that messages were accessible and actionable for all population groups, especially immigrants (Söderberg et al. 2023).
Several explanations can be postulated for our findings. The overall increased inequities among older adults may result from care access barriers following initial quarantine recommendations for those aged ≥70 y and restrictions on nursing home visits, which led to postponed nonurgent oral care services for the elderly at health facilities and suspended domiciliary oral care (Eldh et al. 2021). However, intersectional analysis brought to light the heterogeneity of this group, showing the most pronounced inequities among socially advantaged older adults with high education and income. This may reflect well-grounded concerns about disease transmission among older adults and high compliance with the targeted recommendations for this group. From a broader public health perspective, the increased risk of UOCNs among socially advantaged older adults during the pandemic may be a positive sign of compliance with the recommendations to limit transmission, including the avoidance of nonurgent oral care. The opposite situation might be applicable for the socially disadvantaged younger adults experiencing decreased UOCNs risk. Previous research has shown that young Swedish adults struggled to interpret and implement social distancing recommendations and had a low acceptance of such measures, likely due to their perceived lower risk of infection and severe outcomes (Nilsen et al. 2023; Stefánsdóttir et al. 2024). Nevertheless, some intersectional strata of young adults, predominantly Sweden-born, exhibited a higher UOCNs risk during the pandemic, suggesting that Sweden-born youth faced fewer challenges to access and implement recommendations than their foreign-born counterparts. Indeed, the overall lower risk of reporting UOCNs among immigrants during the pandemic may reflect specific challenges in aligning with the recommendations. Interview studies have reported that the lack of official COVID-19 information in other languages than Swedish, coupled with ineffective information channels, led immigrants to rely on social media and social contacts, through which significant misinformation was disseminated (Söderberg et al. 2023; Söderberg et al. 2024), and immigrant groups indeed had a disproportionally high risk for COVID-19 infection, severe outcomes, and mortality during the pandemic (Folkhälsomyndigheten 2021b). Thus, while the limited changes in oral care–seeking behavior among immigrants during the pandemic may be seen as positive in the context of oral care, it may ultimately reflect an underlying structural disadvantage, where the public health system failed to effectively disseminate important pandemic-related information to protect this group from severe consequences of COVID-19 infection.
Taken together, our findings indicate a reconfiguration of inequities during the pandemic, with both increased and decreased inequities for different intersectional groups. These patterns likely reflect differences in oral care-seeking behaviors shaped by the emphasis on individual responsibility in adhering to public health recommendations, alongside gaps in health communication efforts aimed to reach the whole population.
The strengths of this study include the use of a large sample from a nationwide population survey and a novel intersectional approach. However, the repeated cross-sectional design without a control limited causal inferences. Despite offering valuable insights, the intersectional analysis involved small group sizes, underrepresentation of certain strata, and a simplified categorization of social indicators, potentially underestimating heterogeneity in UOCNs. UOCNs were self-assessed, introducing potential information bias. The potential effect of selection bias was assessed, suggesting that the observed magnitude of inequities disfavoring socially disadvantaged groups may be underestimated. Nonetheless, the consistent magnitude of the estimated bias across both years suggests a minimal effect on the observed changes in inequities. Finally, UOCNs served as a proximal indicator of care utilization; future studies using oral care utilization registers could provide a more comprehensive evaluation.
Conclusions
This study highlights evolving patterns of UOCNs inequities from before to during the pandemic. While disparities related to gender, income, and education persisted, notable shifts included increased inequities among older adults and reduced disparities among immigrants. The intersectional analysis revealed that these changes were most pronounced among socially privileged older adults and least privileged younger immigrants with low education and income. These patterns may reflect the unique Swedish pandemic context, where emphasis on individual responsibility alongside inequitable health communication likely influenced adherence to public health recommendations and health care-seeking behaviors. These findings highlight that future pandemic strategies to ensure equitable oral care access might benefit from addressing the needs and challenges of both medically vulnerable populations, such as the elderly, and socially marginalized groups, such as immigrants facing structural disadvantages.
Author Contributions
C. Anticona, contributed to conception and design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; A.L. Suominen, contributed to conception, data interpretation, critically revised the manuscript; J.L. Bastos, contributed to conception, data interpretation, critically revised the manuscript; P.Lif Holgerson, contributed to conception, critically revised the manuscript; P.E. Gustafsson, contributed to conception and design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Supplemental Material
sj-docx-1-jct-10.1177_23800844251403963 – Supplemental material for Impact of the COVID-19 Pandemic on Intersectional Inequities in Unmet Oral Care Needs in Sweden
Supplemental material, sj-docx-1-jct-10.1177_23800844251403963 for Impact of the COVID-19 Pandemic on Intersectional Inequities in Unmet Oral Care Needs in Sweden by C. Anticona, A.L. Suominen, J.L. Bastos, P.Lif Holgerson and P.E. Gustafsson in JDR Clinical & Translational Research
Supplemental Material
sj-docx-2-jct-10.1177_23800844251403963 – Supplemental material for Impact of the COVID-19 Pandemic on Intersectional Inequities in Unmet Oral Care Needs in Sweden
Supplemental material, sj-docx-2-jct-10.1177_23800844251403963 for Impact of the COVID-19 Pandemic on Intersectional Inequities in Unmet Oral Care Needs in Sweden by C. Anticona, A.L. Suominen, J.L. Bastos, P.Lif Holgerson and P.E. Gustafsson in JDR Clinical & Translational Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by TUA, the County Council of Västerbotten, grant RV-989481 to C.A.; the Swedish Research Council for Health, Working Life and Welfare (FORTE), grant STY-2024/0005 to P.E.G.; and the Faculty of Medicine, Umeå University, grant FS2.1.6-339-20 to P.E.G.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.