
Abstract
Aim:
This review examines the studies on resin composites within the past decade and evaluates the materials’ application methods and success through Fédération Dentaire Internationale (FDI) scores.
Materials and Methods:
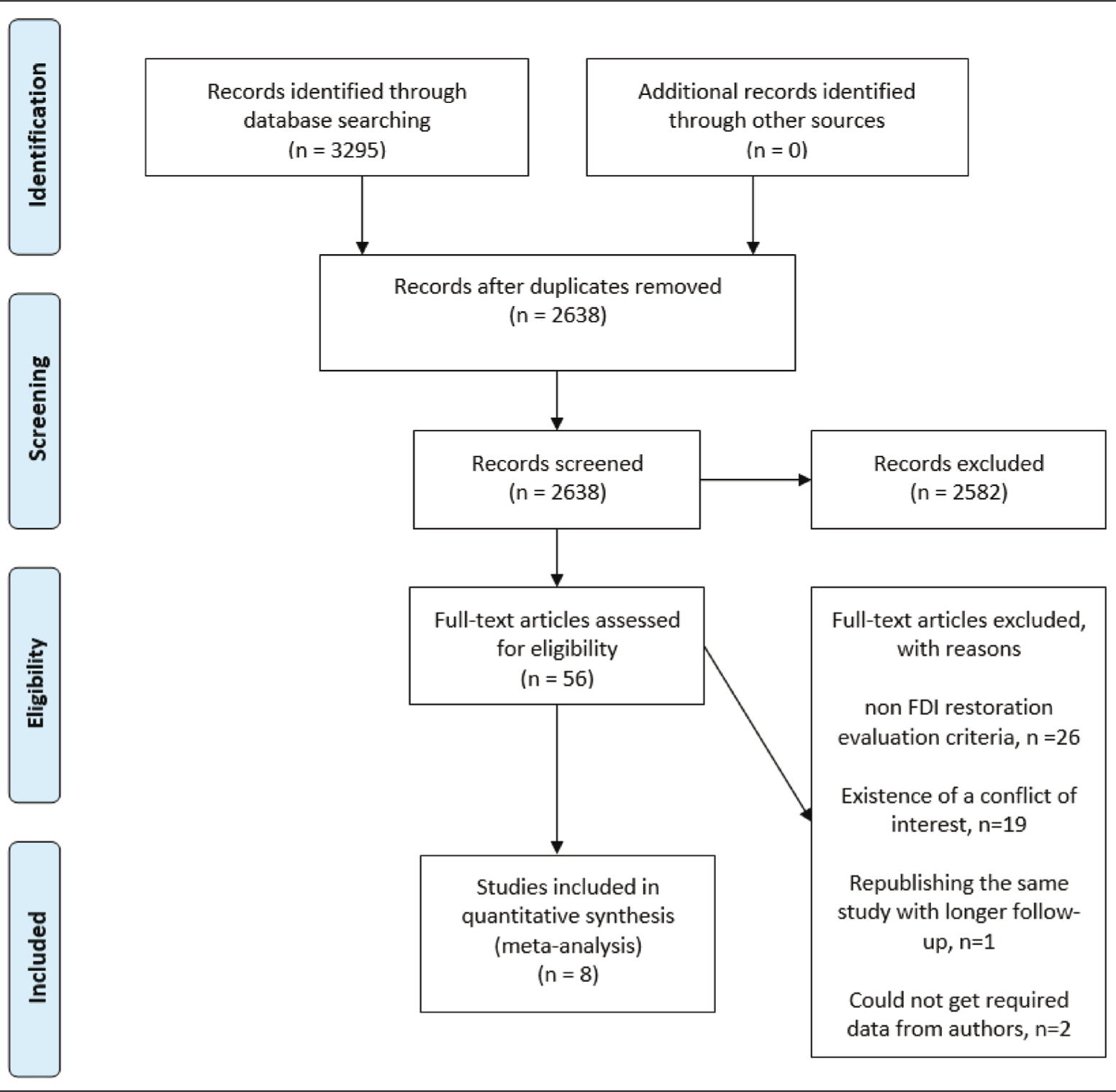
Search results from three databases (a total of 3295 studies) were transferred to Mendeley Desktop (Mendeley, London, UK) software and deduplicated (2638 studies). Eight studies were included in this meta-analysis after scanning the title, abstract, and full-text screening. Risk of bias analysis was performed using the Cochrane Handbook tool. Shapiro–Wilk, Kolmogorov–Smirnov, Kruskal–Wallis, and post hoc Tamhane’s T2 were used for statistical analysis.
Results:
Conventional composite’s surface staining FDI score was higher than flowable and silorane composites (no difference between these two). Also, conventional composite has the highest score in terms of staining. Conventional composite + two-step self-etch adhesive and bulk fill composite + two-step self-etch adhesive have lower FDI scores in marginal staining. In noncarious cervical lesions (NCCL), conventional composite + two-step total-etch adhesive has a higher score than flowable composite + two-step self-etch adhesive. Flowable composite + two-step self-etch adhesive and conventional composite + single-step self-etch adhesive have the highest FDI scores for marginal adaptation (no statistical difference between them). Conventional composite + two-step self-etch adhesive and bulk fill composite + two-step self-etch have the lowest scores (no statistical difference between them). For recurrence of caries, all groups have Score 1, the best score, and there is no significant difference between them.
Conclusions:
Each restorative material and adhesive system has different advantages, and the practitioner must choose the most appropriate.
Introduction
The search for an ideal esthetic material for restoring teeth has significantly improved resin-based composite materials. 1 Today resin composites are the most frequently used esthetic restorative material in dentistry. 2 Restorations have a lifespan, and standardized criteria are used to evaluate them. A more sensitive and discriminative scale than the “modified Ryge criteria” was required to detect early deterioration and signs of failure. In 2007, Hickel et al. proposed a new system based on three criteria categories: aesthetic, functional, and biological. 3 The criteria defined by Hickel et al. were approved by the Science Committee of the Fédération Dentaire Internationale (FDI) World Dental Federation in 2007. 4 Later, some criteria and scores were updated in 2010. 5 Successful restorations are evaluated in three stages (clinically excellent, clinically good, and clinically sufficient). Unsuccessful restorations are evaluated in two stages (clinically unsatisfactory, clinically poor) in 16 criteria (surface luster, marginal staining, surface staining, color match and translucency, esthetic anatomical form, fracture of material and retention, marginal adaptation, occlusal contour and wear, approximal anatomical form, radiographic examination, patient’s view, postoperative sensitivity and tooth vitality, recurrence of caries-erosion-abfraction, tooth integrity, periodontal response, oral and general health). 5
Restoration evaluations solely based on the success rate can be misleading. Evaluations made with only two categories, successful and unsuccessful, ignore the stages of success and failure. A more detailed approach is required in evaluating restorative materials or applications. This study aims to examine the studies on resin composites within the past decade and evaluate the application methods and the success of the materials through FDI scores, which is thought to be a more detailed approach.
Materials and Methods
Protocol
This systematic review followed the recommendations established by the preferred reporting items for systematic reviews and meta-analyses (PRISMA) protocol. 6
Eligibility Criteria
Randomized controlled clinical trials on humans for the success of resin composite restorations on humans with permanent dentition.
The study must have at least three years of follow-up.
The evaluation of the restorations should be made according to the FDI criteria.
Exclusion Criteria
Studies on endodontically treated teeth.
Any conflict of interest.
Information Sources and Search Strategies
Study selection was conducted in the following electronic databases: PubMed, Cochrane, ScienceDirect. The term “resin composite” was used to search these databases. The search was done on 07 October 2020, and the date range filter was set as 01 January 2010 to 07 October 2020.
Study Selection
Search results from three databases (a total of 3295 studies) were transferred to Mendeley Desktop software and deduplicated (2638 studies). With the help of RobotSearch, 7 a machine learning-based artificial intelligence (AI) application, 8 randomized controlled trials were filtered. In addition to the appropriate articles, undecided articles were included in the abstract evaluation. Abstracts considered potentially eligible and those not providing sufficient information on the eligibility criteria were separated for full-text evaluation. After the full-text evaluation, it was decided that 10 articles met the acceptance criteria of this meta-analysis. Three of these articles did not have a cumulative FDI scoring table. Relevant authors were contacted; Favetti et al. 43 shared the dataset, Loomans (2018) 44 did not reply, and ÖZ et al. 37 did not contribute. So, this meta-analysis was conducted with eight studies.
Data Extraction
Two reviewers (TK and AYU) conducted data extraction. General information includes authors, year of publication, geographic region, scores of FDI restoration evaluation criteria (surface luster, surface staining, color stability and translucency, anatomic form, marginal staining, fractures and retention, marginal adaptation, wear, contact point/food impact, radiographic examination, patient’s view, postoperative sensitivity, recurrence of caries, tooth integrity, periodontal response, adjacent mucosa, oral and general health), type of restored cavity, used resin composite and adhesive type, power of polymerization unit, polishing process, number of restorations performed and evaluated, follow-up time, and conflict of interest state extracted. In addition, the randomization type, accepted patients and their acceptance criteria, blinding type, sample size and recall rate, outcomes, and funding data were extracted for the bias assessment.
Data Analysis
For evaluating marginal staining, retention and fractures, marginal adaptation, and recurrence of caries, following groups were created based on the studies included in this meta-analysis:
Conventional composite + two-step total-etch adhesive Conventional composite + two-step self-etch adhesive Conventional composite + single-step self-etch adhesive Bulk-fill composite + two-step self-etch adhesive Bulk-fill composite + single-step self-etch adhesive Flowable composite + two-step self-etch adhesive Silorane composite + silorane system adhesive
For surface luster, surface staining, and color stability, following groups were created:
Conventional composite Bulk-fill composite Flowable composite Silorane composite
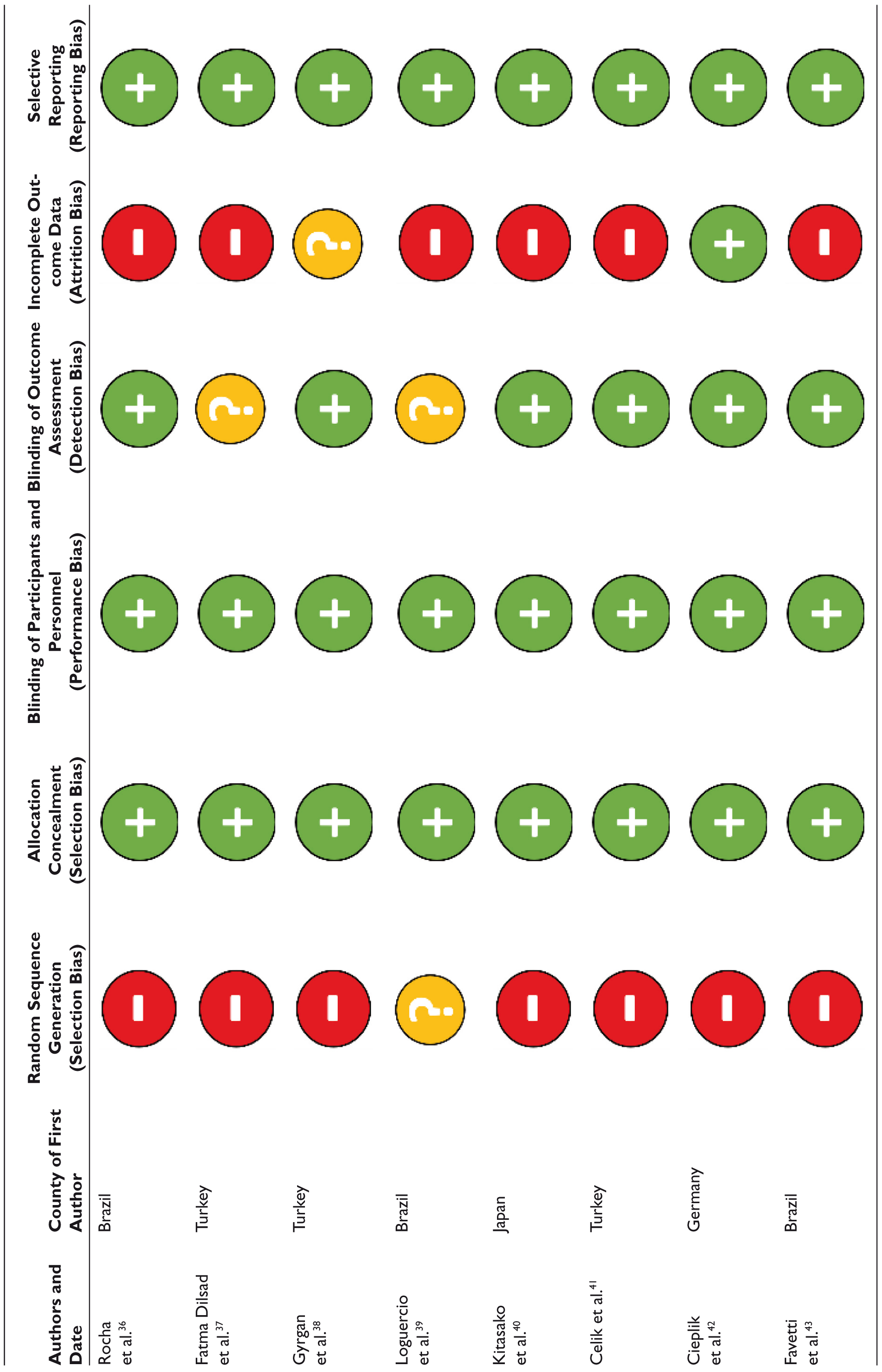
Risk of bias analysis was performed using the tool available in the Cochrane Handbook.
9
The evaluation criteria comprised six items: random sequence generation, allocation concealment, blinded evaluations of results, blinding of participants and staff, results with incomplete data, selective report of the outcome, and other possible sources of bias. The six domains were evaluated, and the included studies were classified. The datasets generated during the current study are available in the Mendeley Data repository, “
PRISMA Flow Diagram
Statistical Analysis
Shapiro–Wilk and Kolmogorov–Smirnov analyzes were performed to determine the FDI score dataset’s distribution characteristic. Skewness and kurtosis values were also examined. Because the FDI scores are generally at a value of one, they did not show a normal distribution. Therefore, Kruskal–Wallis, a nonparametric test used to compare more than two independent samples and a powerful alternative to the one-way analysis of variance, 10 and post hoc Tamhane’s T2 analyzes were used for further statistical analysis.
Results
Risk of bias analysis was performed with the tool available in the Cochrane Handbook, summarized in Table 1.
Risk of Bias Assessment
The average three-year follow-up results of the studies evaluated according to the determined groups are shown in Figures 2 and 3.
Descriptives
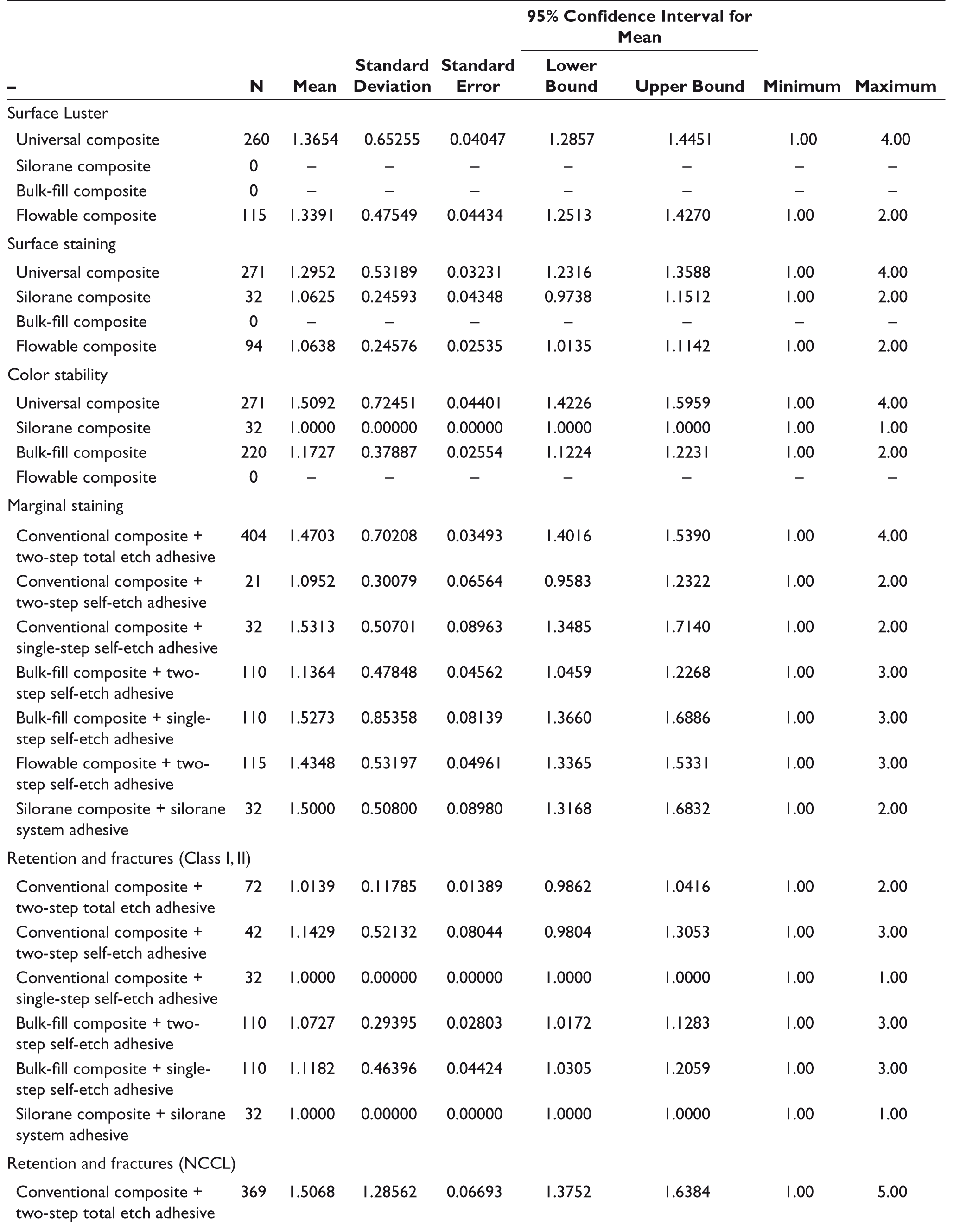
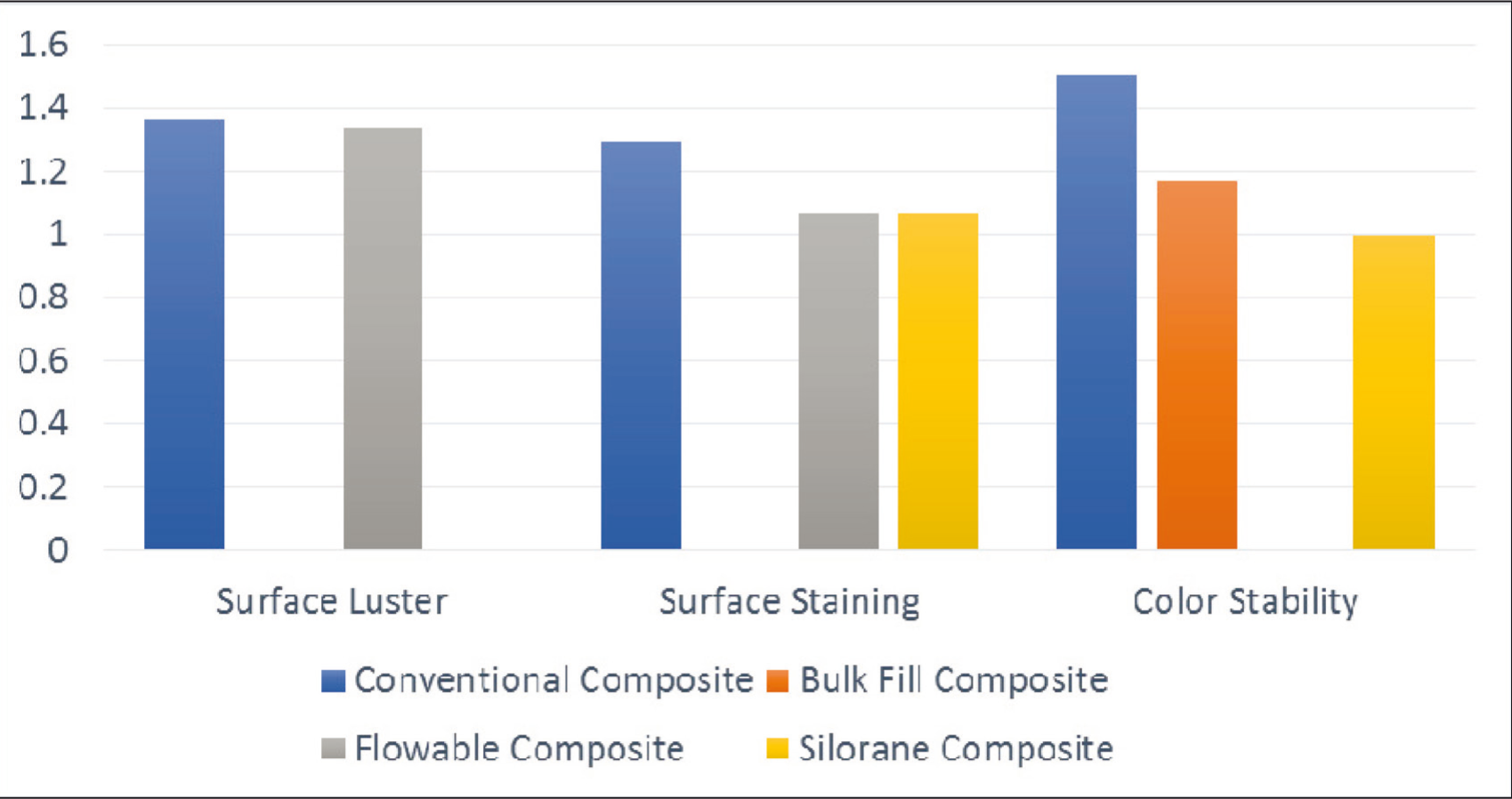
As a result of the statistical analysis of the available data, there was no difference between the conventional composite and flowable composite in surface luster scores. The surface staining FDI score of the conventional composite was higher than flowable composite and silorane composite (no difference between these two; P < .05). Also, conventional composite has the highest score in terms of staining.
Conventional composite + two-step self-etch adhesive and bulk-fill composite + two-step self-etch adhesive have lower FDI scores in marginal staining. There is no statistical difference between the other composite-adhesive systems.
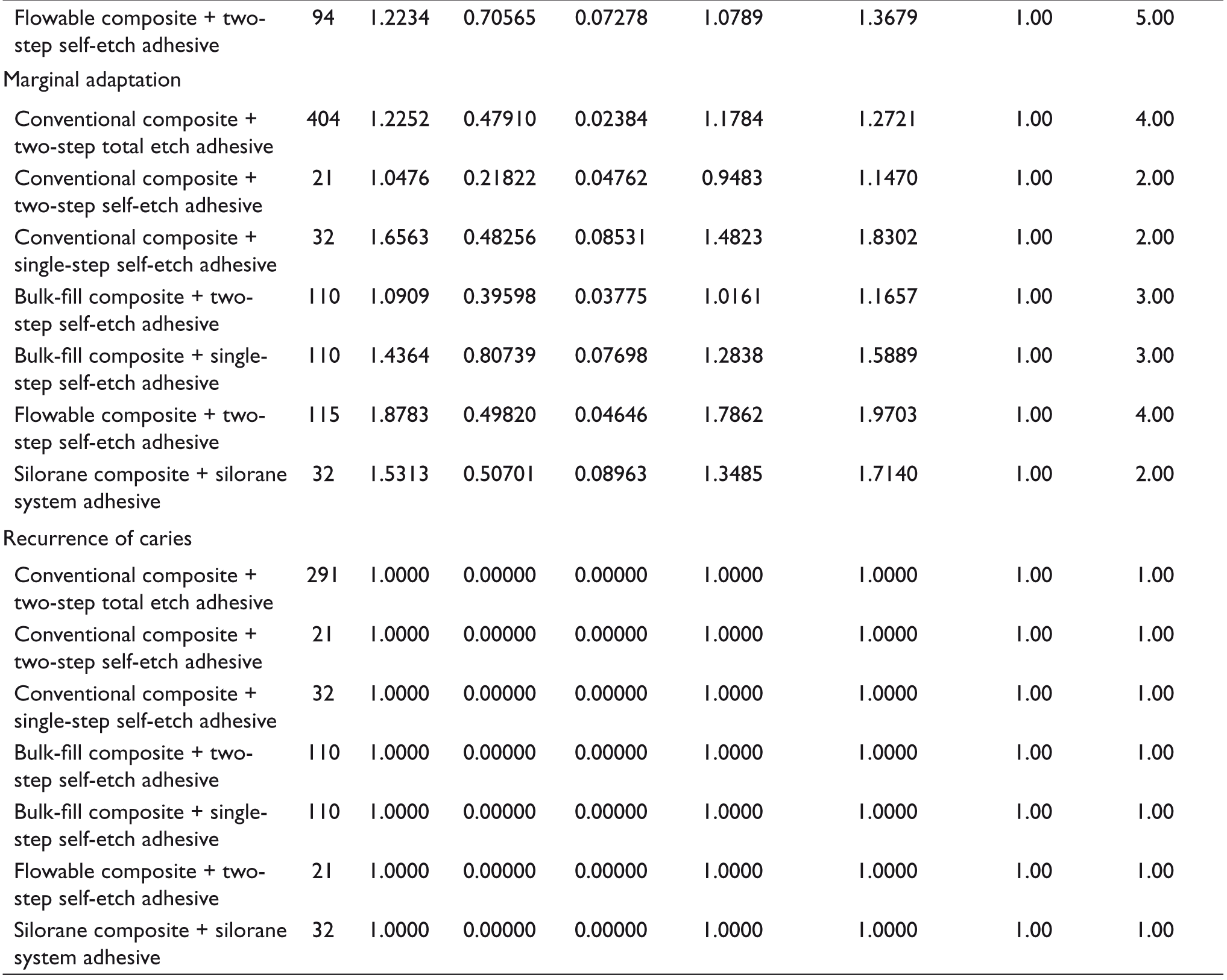
There is no statistical difference between composite and adhesive systems groups for FDI retention and fracture scores in occlusal restoration. In contrast, NCCL conventional composite + two-step total-etch adhesive has a higher score than flowable composite + two-step self-etch adhesive.
Flowable composite + two-step self-etch adhesive and conventional composite + single-step self-etch adhesive has the highest FDI scores (no statistical difference between them) for marginal adaptation. Conventional composite + two-step self-etch adhesive and bulk-fill composite + two-step self-etch have the lowest scores (no statistical difference between them).
For recurrence of caries, all groups have Score 1, the best score, and there was no significant difference between them. Descriptives for all scoring groups can be found in Table 2.
Discussion
The purpose of systematic reviews is to provide the best available evidence of the effects of interventions given a particular research question. Meta-analysis is a statistical method that uses the results of independent studies included in a systematic review and whose accuracy is high, thanks to the combined analysis of independent studies. 11 The studies included in this meta-analysis were requested to be of the highest quality possible. The median survival time of resin composite restorations is 10 years. 12 The longer the follow-up period in the studies, the more useful information they may provide us, but the number of studies with a long follow-up period is quite limited. FDI criteria were reported as practical (various and freely selectable criteria), relevant (sensitive as well as appropriate to current restorative materials and clinical studies design), and standardized (making comparisons between different investigations easier). 4 FDI recommends at least three years of follow-up for clinical evaluation of direct restorative materials. 5 Considering the balance between follow-up time and the number of studies, we used restoration score data for the three-year follow-up in this meta-analysis. Additionally, techniques and materials used in dentistry change rapidly with the advancement of technology, and the use of the old ones is disappearing. For this reason, we only examined studies conducted in the past decade. To avoid any potential bias, we did not include studies with conflicts of interest in this meta-analysis. Eight studies were included in this meta-analysis. The clinical success of resin composite and adhesive systems at the end of the three-year follow-up was evaluated according to FDI criteria.
Composite resins are the most preferred material for direct dental restorations. 13 Based on the studies included in this meta-analysis, resin composites were evaluated under four main headings; conventional composite resin, bulk-fill composite resin, flowable composite resin, and silorane composite resin.
Although bulk fill is not new and several materials have been available over the years, recently, there has been a surge of interest in these materials. A host of new products, including both flowable and high viscosity pastes, have become available from various manufacturers. The newer materials have increased translucency, thus allowing for greater light transmission and consequently increased depth of cure. One product incorporates a new germanium initiator to enable greater cure depths. 14 Some meta-analysis studies show that conventional and bulk-fill composite resins do not significantly differ in terms of the type of restoration, the type of tooth restored, and the technique applied.15–17 According to the results of our study, the color stability of the bulk-fill composite is more successful than the conventional composite resin (Figure 1).
Flowable composites are easy to use and have good rheological properties. 18 Its low elasticity module has been recommended suitable for use in noncarious lesions, especially in the cervical region. 19 The surface luster of the flowable composite resins is similar to the conventional composite resin. In addition, while the surface staining has similar values to the bulk-fill composite, it was more successful than the conventional composite resin (Figure 1). This situation contradicts the perception that flowable composites undergo more color change than conventional composites. 20 , 21
Silorane composite has been developed to minimize polymerization shrinkage and eliminate the stresses caused by it. Unlike others, silorane composites are polymerized via cationic intermediates. During this polymerization, space is gained through the cleavage and opening of the ring system, and then this area is lost during the formation of chemical bonds. Thus, polymerization shrinkage is claimed to be reduced. 22 According to this meta-analysis, silorane composites show a more positive appearance than conventional composite resins in surface coloration and color stability (Figure 1). Still, a very limited number of studies on silorane were included in this meta-analysis, and more quality studies are needed to make a more precise conclusion.
Because marginal staining, retention and fractures, marginal adaptation, and recurrence of caries parameters can also be affected by the applied adhesive system, it was thought that it would be appropriate to make the evaluations according to the combinations of resin composite and adhesive system.
Conventional composite + two-step self-etch adhesive and bulk-fill composite + two-step self-etch adhesive are more successful for marginal staining. There was no significant difference between the other groups (Figure 2). As a result of another meta-analysis study conducted on direct composite resins, marginal staining did not make a statistically significant difference. 23 One of the studies of marginal staining reported that the worst marginal staining was found in silorane resin composites. 24 Marginal staining may be related to the nature of the adhesive system used in restorations and individual factors such as smoking and drinking (wine, coffee, etc.).25–27
Distribution of the Scores of the Resin Composite Types According to the Selected FDI Criteria
Distribution of the Scores of the Resin Composite and Adhesive Systems According to the Selected FDI Criteria
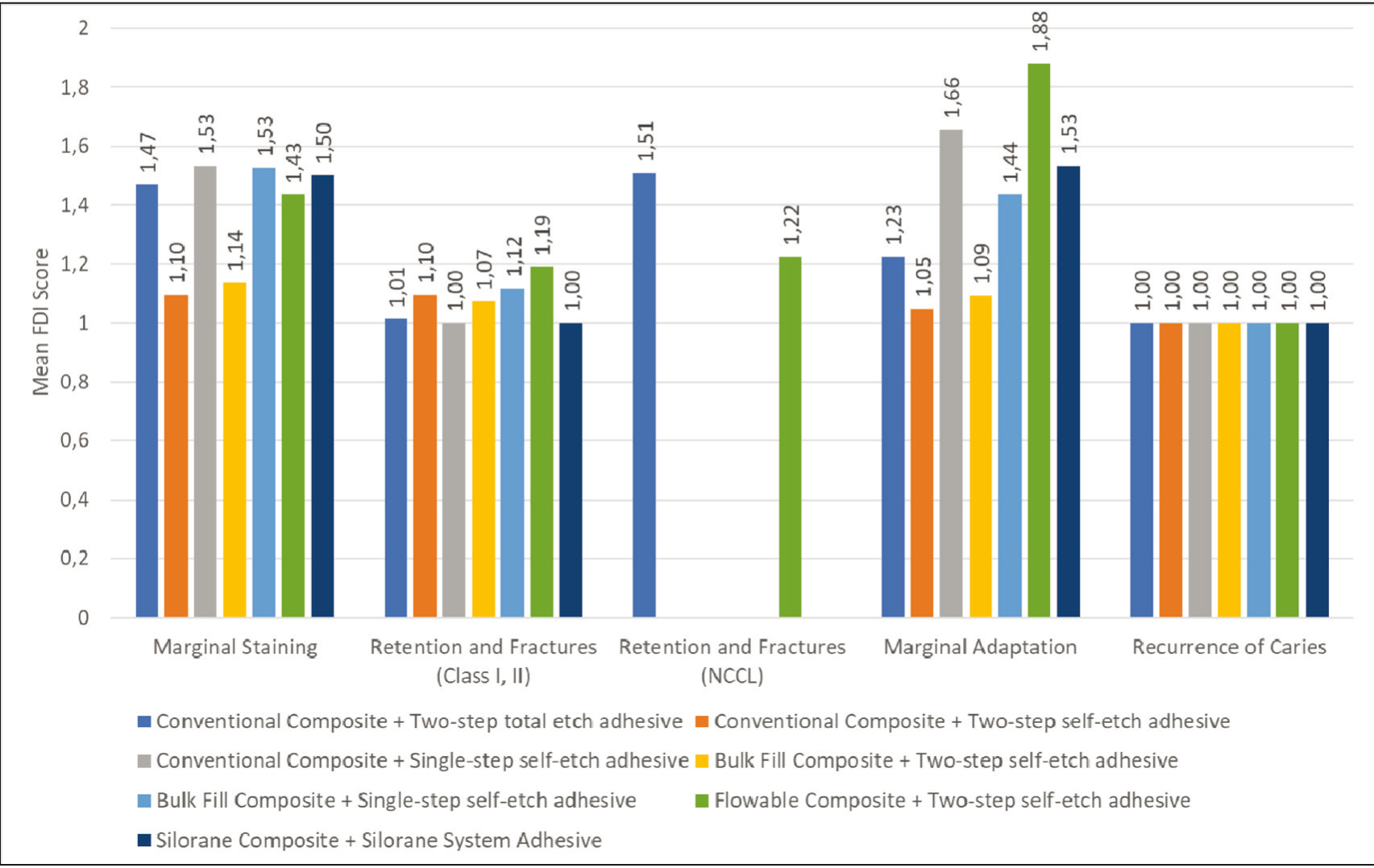
Because restorations made to the cervical region differ significantly from those made to the occlusal surface in terms of retention and fracture, we have examined them under a separate heading. Our study shows this difference when the conventional composite + two-step total-etch in Figure 3 is examined. Although this system has a very good score in the restoration of occlusal surface lesions (1.01), its score is considerably increased (1.51) when used in the cervical area (it should be noted that a lower score is better according to the FDI criteria). Restoration retention and polymerization shrinkage of resin composites are directly related to each other. 28 The volumetric shrinkage of the resin composite and its tendency to detach from dental tissue create stresses that can cause marginal loss of adaptation and retention. 29 When the flowable composite + two-step self-etch adhesive system is examined, a comparable level of success is observed between occlusal restorations and cervical restorations. This situation may be because flowable composites are more flexible because of their high resin content and are more resistant to shear forces and fatigue. 30 Another study found no significant difference between the retention rate of the three-step etching rinse or the one-step etching rinse in NCCL. 31
There is no significant difference between the flowable composite + two-step self-etch adhesive and the conventional composite + one-step self-etch adhesive in marginal adaptation, and their marginal adaptation success is low. However, the adaptation success of traditional composite + two-step self-etch adhesive and bulk-fill composite + two-step self-etch adhesives is high (Figure 2). In a meta-analysis study, 15 studies were evaluated and showed that the overall effect of conventional composite resins was better than other new-generation composite resin types in the first 12 months, with no difference between them in longer follow-ups. 23 However, it should be taken into account that various factors related to the properties of composites (such as the type and viscosity of the composites) and application procedures can affect marginal adaptation. According to some authors, the type and viscosity of the resin composite affect the formation of gaps between the tooth and restoration. 32 , 33
There is no difference between all groups for caries recurrence, and success rates are high (Figure 2). The recurrence of carious lesions observed around the restoration is one of the causes of failure of composite restorations, which is still under debate.34,35 It should be considered that the type of restorative material used in developing recurrence caries lesions, individual habits, as well as the type of carious cavity and the restoration site, may be effective. 35
According to FDI, evaluating every parameter in clinical studies is unnecessary. Researchers generally evaluate popular parameters such as retention, marginal discoloration, and postoperative sensitivity in their studies. None of the clinical studies included in this meta-analysis have evaluated all the parameters determined by the FDI. The use of FDI criteria in the evaluation of restorations is increasing. However, many studies are based on other criteria (mainly the United States Public Health Service (USPHS) and some custom criteria), and excluding these studies may create bias. This meta-analysis involves data from studies performed by different clinics in different institutions and countries, and the calibration of the evaluators may differ between studies. Experts usually carry out studies at universities, and restorations are carried out with care because they will be the subject of a scientific study; the result of these studies may not be reflected in general use.
Conclusion
Each restorative material and adhesive system has different advantages, and the practitioner must choose the most appropriate.
Footnotes
Acknowledgements
The authors declare that there is no conflict of interest. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. T.K. and A.Y.U conceived the ideas, T.K. and A.Y.U. collected the data, T.K. analyzed the data, T.K. led the writing, and T.K. and A.Y.U. gave final approval. The data supporting the findings of this study are openly available in Mendeley Data at
Authors’ Contribution
Türkay Kölüş: conceptualization, methodology, software, data curation, writing-original draft preparation, visualization, investigation, supervision, validation, writing-reviewing, and editing. Arzu Yağmur Uçar: data curation, investigation, and writing-original draft preparation.
Ethical Approval institutional statement
The meta-analysis study is exempt from ethics approval as the study authors will be collecting and synthesizing data from previous clinical trials in which informed consent has already been obtained by the trial investigators.
Data Availability Statement
The data that support the findings of this study are openly available in Mendeley Data at “
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for research, authorship, and/or publication of this article.