
Abstract
Aim:
Although the shelf life is a key property of dental composites and bonding agents, these materials may often be used in simple procedures after expiration. In this study, the microleakage of two year expired and non-expired dental composites (Filtek Ultimate Universal A2 Enamel, 3M ESPE, USA, and Tetric N Ceram A2, Ivoclar Vivadent, Schaan, Liechtenstein) and a universal bonding system (Single Bond Universal, 3M ESPE, USA) was examined.
Materials and Methods:
In 40 freshly extracted human molars, two standardized Class II cavities (buccolingual and mesiodistal width of 3 mm and 4 mm, respectively) were prepared (80 cavity preparations). The teeth were thermocycled in distilled water for 1000 cycles in a 5°C to 55°C water bath. Next, the teeth and their apical foramens were coated with water resistant nail varnish, except for 1 mm around the restoration–tooth interface, and retained in a 1% methylene blue solution. After 24 h, the specimens were cut into two halves and analyzed using a stereomicroscope. Scanning electron microscopy images of two samples of the groups were obtained.
Results:
The Kruskal–Wallis test indicated no significant differences between the groups (P < .05). The occlusal median scores were not significant (P = .99). Moreover, the gingival median scores were not significant (P = .48). No difference was found between the occlusal and gingival values in any group (P > .05).
Conclusion:
These findings indicated that two-year-expired dental composites and bonding agent, which were maintained under proper conditions, do not have any significant difference in terms of the microleakage.
Introduction
Restorative dentistry techniques are being increasingly enhanced with the introduction of novel materials to the dental domain. 1 Although the use of resin composites is preferred by clinicians owing to the indisputable aesthetics, ease of handling, and polymerization process of such materials, their application is limited owing to the low wear resistance, poor bonding at the resin–dentin interface, and occurrence of polymerization shrinkage. 2 Moreover, dental composites deteriorate over time owing to exposure to different intraoral and extraoral conditions, corresponding to chemical changes and a combination of oxidative chain scission effects, oxidation hydrolysis, and changes in crystallinity or environmentally dependent factors. 3 This degradation depends on the organic and inorganic characteristics of the materials and coupling agent chemistry. 4 The breakdown of the resin structure leads to the fracture of the dental materials or a strength reduction of the resin–dentin interface, 5 thereby decreasing the material lifetime. 4
The shelf life of composite materials can be defined as the period in which the materials are expected to exhibit the desired physical and mechanical properties in the appropriate indication from the date of production. 6 Manufacturers usually define this period as two years after the production date. If a material is applied after its expiration date, its performance may be suboptimal. 7 In clinical practice, in general, only small amounts of dental composites are necessary to perform restorative procedures, and a considerable amount of the materials may expire prior to being used. 8 Nevertheless, several dentists continue to use these materials. 9 In addition, many suppliers offer discounts on expired dental composites, and thus, the extended use of these materials is increasing. Notably, the use of expired dental composites is not ethically acceptable and not recommended medically. However, other uses for expired composites that are still polymerizable may be considered, such as in direct mock-ups, for diagnostic purposes, and for stabilizing matrix bands and temporary crowns.9,10
In this regard, it is necessary to examine the properties of expired products and clarify the degree of change in the material properties. Microleakage, as a key aspect in resin composite-based restorations, is related to the marginal integrity.4,11 Microleakages may occur if a marginal gap exists or disruption of integrity occurs between the tooth and the restoration interface, even in a temporary restoration. 12
Considering these aspects, in this study, the microleakage performance of two year expired and non-expired dental composites and universal bonding systems was compared. The tested null hypothesis was that the use of expired dental composites and universal bonding systems did not correspond to a significant change in the microleakage characteristics of dental restorations.
Materials and Methods
Setting and Design
This study was conducted from January 2020 to February 2020 at Faculty of Dentistry, Trakya University, Edirne. This study was approved by the Ethical Committee of Trakya University Faculty of Medicine (TÜTF-BAEK 2019/331).
Presampling Procedure for all Specimens
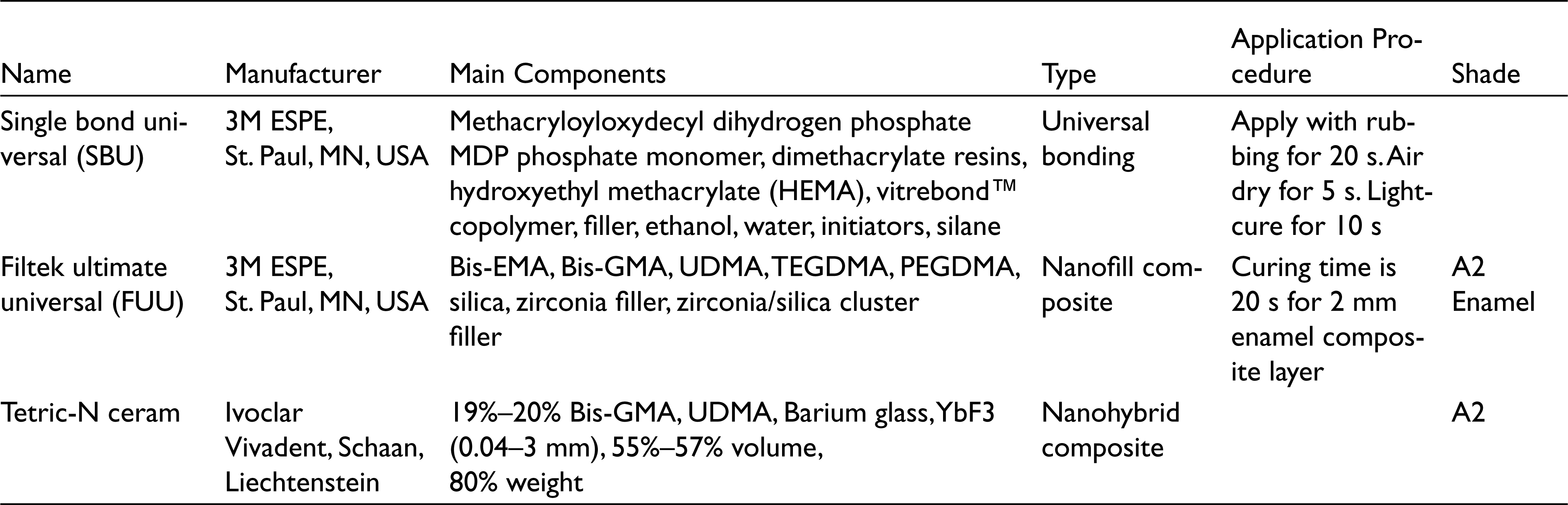
Forty human molars, extracted for periodontal or orthodontic reasons, were used in the study. None of the teeth had any caries, hypoplastic defects, old restorations, or cracks. After the surface of the teeth were cleaned using hand instruments and ultrasonic scaling, the teeth were stored in 0.1% thymol solution for up to three months at room temperature until the research was performed. The details of the adopted products are listed in Table 1.
Materials Used in This Study
Cavity Preparation and Restoration
Occlusomesial and occlusodistal cavities were prepared in each tooth by a single operator, leading to a total of 80 Class II cavities. A cylindrical round-end diamond bur (Bosphorus, Turkiye) was used with a high-speed hand piece in the presence of sufficient water, and the tool was changed after every five preparations to enable efficient cutting. The dimensions of the cavities were standardized: the occlusal depth, buccolingual width, and mesiodistal width were 3 mm, 3 mm, and 4 mm, respectively. For the proximal cavities, the buccolingual and gingival widths were 3 mm and 3 mm, respectively. Gingival floors were finished at the cemento-enamel junctions. Notably, 2 mm sound tooth tissue was retained between the occlusomesial and occlusodistal cavities. After the cavity preparation, the teeth were etched (15 s and 30 s for dentin and enamel, respectively) by using 37% phosphoric acid (Extra Gel, Wp Dental, Germany). The teeth were washed and dried and randomly divided into eight groups.
For the material use, all the manufacturer instructions were followed. The circumferential straight metal matrix (Matrix Band, Polydentia SA, Mezzovico, Switzerland) was adapted, and the bonding agent (Single Bond Universal 3M ESPE, St. Paul, MN, USA) was applied to the cavities for 20 s. The sample was air dried for 5 s and light cured for 10 s by using an LED light-curing unit with a light irradiance of 1200 mW/cm2 (Elipar S10; 3M ESPE, USA). The teeth were restored in 2 mm increments of the dental composite, and each incremental section was irradiated for 20 s. The restorations were finished and polished using polishing discs (Shofu, Super-Snap Rainbow Technique Kit, Shofu, Inc., Kyoto, Japan).
The details of the groups are as follows
Group I: (n = 10; occlusomesial cavities) non-expired dental bonding (Single Bond Universal, 3M ESPE, USA) and non-expired dental composite (Filtek Ultimate Universal A2 enamel, 3M ESPE, USA) Group II: (n = 10; occlusodistal cavities) non-expired dental bonding (Single Bond Universal, 3M ESPE, USA) and non-expired dental composite (Tetric N Ceram A2, Ivoclar Vivadent, Schaan, Liechtenstein). Group III: (n = 10; occlusomesial cavities) non-expired bonding (Single Bond Universal, 3M ESPE, USA) and two year expired dental composite (Filtek Ultimate Universal A2 Enamel, 3M ESPE, USA). Group IV: (n = 10; occlusodistal cavities) non-expired bonding (Single Bond Universal, 3M ESPE, USA) and two year expired dental composite (Tetric N Ceram A2, Ivoclar Vivadent, Schaan, Liechtenstein). Group V: (n = 10; occlusomesial cavities) two year expired bonding (Single Bond Universal, 3M ESPE, USA) and two year expired dental composite (Filtek Ultimate Universal A2 Enamel, 3M ESPE, USA). Group VI: (n = 10; occlusodistal cavities) two year expired bonding (Single Bond Universal, 3M ESPE, USA) and two year expired dental composite (Tetric N Ceram A2, Ivoclar Vivadent, Schaan, Liechtenstein). Group VII: (n = 10; occlusomesial cavities) two year expired bonding (Single Bond Universal, 3M ESPE, USA) and non-expired dental composite (Filtek Ultimate Universal A2 Enamel, 3M ESPE, USA) Group VIII: (n = 10; occlusodistal cavities) two year expired bonding (Single Bond Universal, 3M ESPE, USA) and non-expired dental composite (Tetric N Ceram A2, Ivoclar Vivadent, Schaan, Liechtenstein).
Thermal Cycles and Dye Penetration Test
After being stored at 37°C and 100% humidity for 24 h, all the samples were thermocycled (SD Mechatronik, Germany) in distilled water for 1000 cycles in a 5ºC to 55ºC water bath. The thermocycle duration was 30 s, and the transfer time was 5 s. Subsequently, the teeth and their apical foramens were coated with water resistant nail varnish, except for 1 mm around the restoration–tooth interface. The specimens were retained in a 1% methylene blue solution (Gündüz Kimya, Turkiye) for 24 h. 13 Next, the specimens were washed using water and cut into two halves in the mesiodistal direction by using water-cooled low-speed discs (San-I, China). The halves that were most stained by the dye were analyzed under a stereomicroscope (Leica stereomicroscope MZ 9.5, Leica Microsystems, Wetzlar, Germany) at 20× magnification.
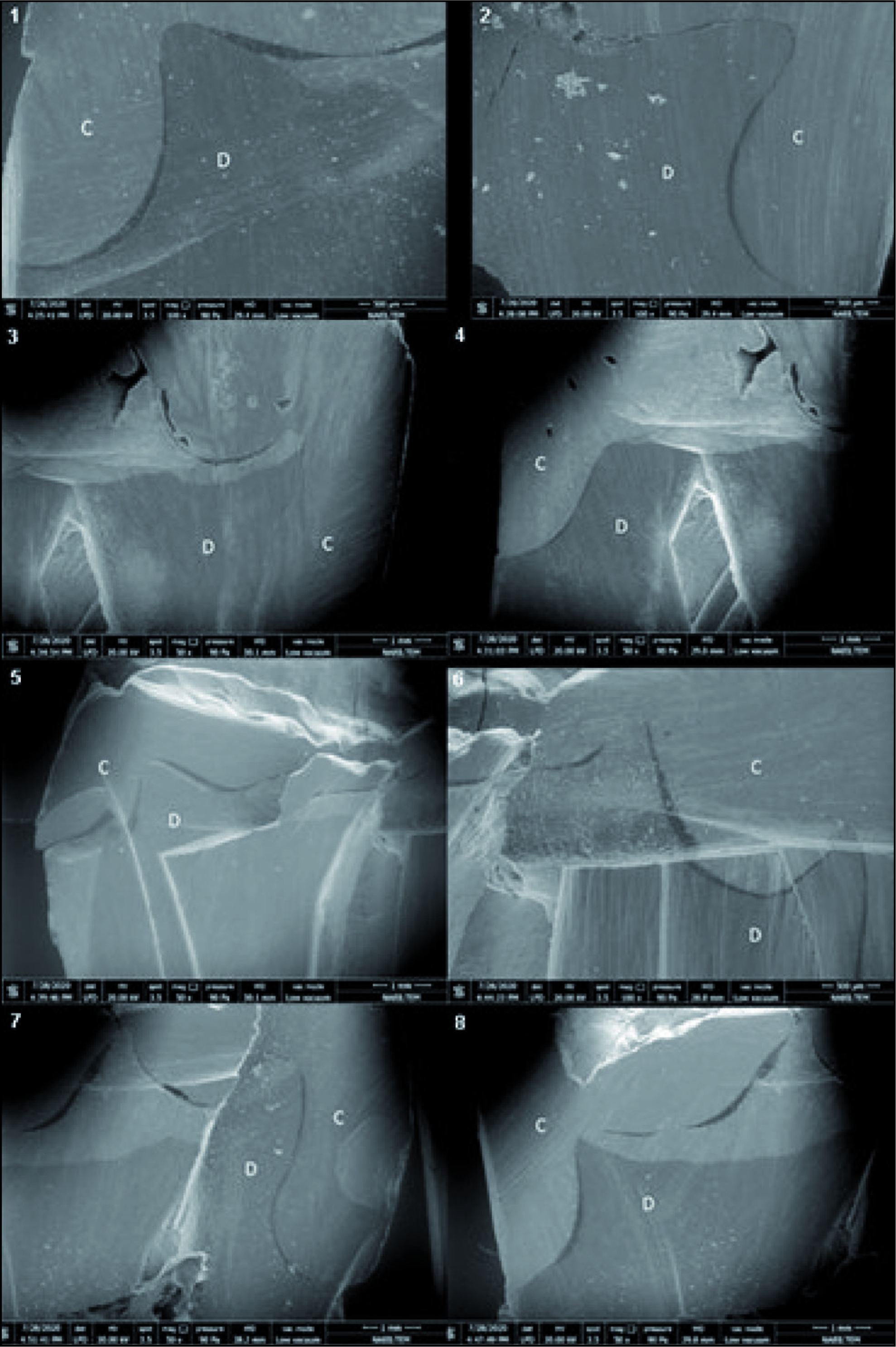
Both gingival and occlusal areas were analyzed and assigned suitable scores: the scores for the occlusal restorations were as follows: 0 (no dye penetration), 1 (dye penetration toward the enamel), 2 (dye penetration toward the dentin not containing the pulpal and gingival wall), and 3 (penetration toward the dentin containing the pulpal wall). 10 The scores for the gingival restorations were as follows: 0 (no dye penetration), 1 (dye penetration along half of the gingival wall), 2 (dye penetration along the entire gingival wall), and 3 (dye penetration along the entire axial and gingival wall). 10 Scanning electron microscope (SEM) photographs of two samples of the group were captured using the Quanta FEG 250 device manufactured by the FEI company (Hillsboro, OR, USA) at ×50, ×100, ×200, ×400, ×800 magnifications.
Statistical Analysis
Data were analyzed using IBM SPSS V23. The Shapiro–Wilk test was performed for normal distributions. For the non-normal data, the Kruskal–Wallis test was adopted. Data were analyzed as median (minimum-maximum) values. The significance level was P < .05.
Results
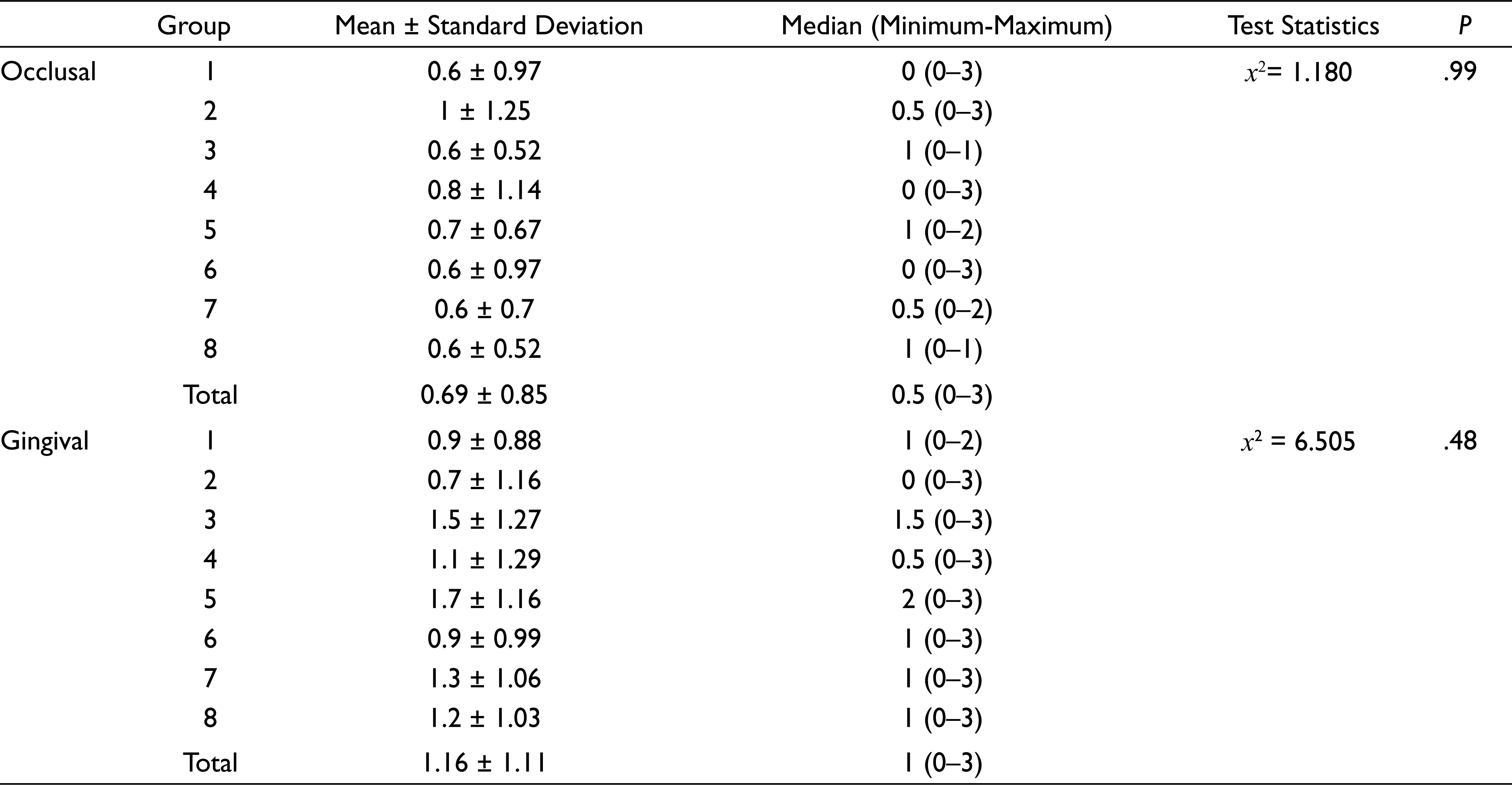
Figures 1 shows the SEM evaluations for each group. The median leakage scores and mean values for each group are listed in Table 2.
The SEM Photographs of Groups 1–8
The Kruskal–Wallis test did not indicate any significant differences between the groups (P < .05). The occlusal median scores were not significant in terms of the groups (P = .99). Moreover, the gingival median scores were not significant in terms of the groups (P = .48).
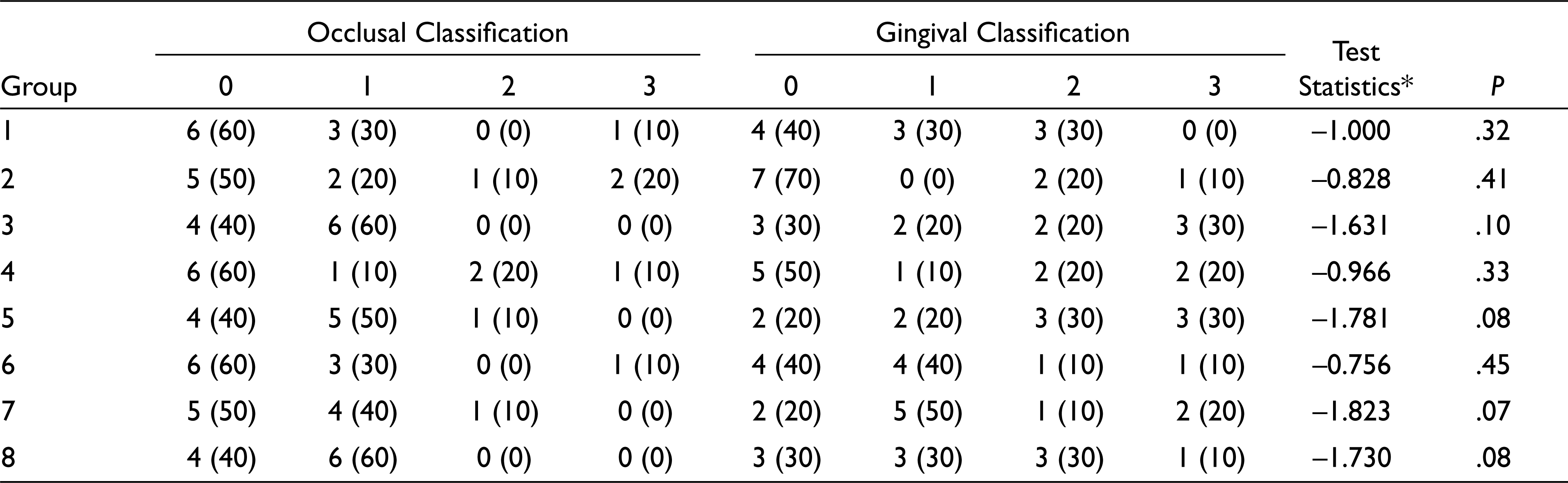
The occlusal score distributions did not differ between the groups (P = .99); the detailed distribution information is presented in Tables 2. Furthermore, the gingival score distributions did not differ between the groups (P = .48); the detailed distribution information is presented in Table 2. Moreover, no difference was found between the occlusal and gingival values in any group (P > .05; Table 3)
Comparison of Occlusal and Gingival Scores in Terms of the Groups
Although no dye penetration occurred in 50% of the occlusal group, 37.5% of the samples exhibited dye penetration extending into the enamel, 6.3% exhibited dye penetration extending into the dentine not involving the pulpal-gingival wall, and 6.3% exhibited dye penetration extending into the dentine with the pulpal wall. Although 37.5% of the gingival group did not exhibit any dye penetration, 25% exhibited dye penetration in half of the gingival wall, 21.3% exhibited dye penetration through the whole gingival wall, and 16.3% exhibited dye penetration in the gingival and axial walls (Table 3).
Comparisons Within Groups
Discussion
Non-expired and expired (for two years) universal bondings and resin composites were evaluated in terms of the microleakage. Teeth restored using an expired bonding and composite exhibited comparable microleakage scores to those of teeth restored using non-expired materials. Moreover, no statistically significant differences in the microleakage scores were observed for different combinations of expired and non-expired dental composites and bondings. Thus, the null hypothesis was accepted.
In general, the advancements in resin adhesives and dental composites have extended their usage for both anterior and posterior restorations. However, polymerization shrinkage occurs in dental composites owing to the presence of methacrylate monomers.14,15 Moreover, cuspal deflection, and marginal microleakage often occur owing to polymerization shrinkage. 14 Marginal microleakage is a key criterion to predict the performance of dental restorations, and dentists must aim to ensure the marginal sealing of the restorations. 16 Notably, a previous study reported that the use of a dental material after its expiration date corresponds to a suboptimal performance. 3
In general, the marginal sealing is influenced by many factors including the layering technique, polymerization of dental composites, dental composite characteristics, and cavity geometry and size.17,18 This standardized study was performed to clarify the effect of only the resin variables. Although no consensus exists regarding the cavity dimensions, in this study, the prepared cavities had a mesiodistal width, buccolingual width, and occlusocervical depth of 4 mm, 3 mm, and 3 mm, respectively. 15 Each cavity was restored via oblique layering to reduce the polymerization shrinkage. 15 All the materials were applied according to the manufacturer recommendations. The test materials were kept refrigerated in the manufacturer-specified ranges before the research. 19
To mimic the thermal difference of the oral environment, thermocycling was performed. In general, the environment for a single day corresponds to 20 to 50 cycles, 20 and 10,000 cycles likely represent approximately one year of in vivo functioning. No significant difference in the microleakage scores has been previously observed for 250, 1000, and 5000 cycles. 21 Moreover, in many microleakage studies, 1000 cycles have been implemented to mimic the thermal conditions of the oral environment.13,14,22 Thus, in the present study, the samples were subjected to 1000 cycles. However, different results can be obtained in long-term aging.
As mentioned previously, the composite polymerization affects the microleakage and marginal sealing. In particular, the degree of polymerization, which is directly related to the photoinitiator concentration, is degraded over the shelf life of the composite, thereby influencing the mechanical properties of dual-cured resin composites. 23 Degradation of the photoinitiators may lead the incomplete curing of the monomers, corresponding to higher microleakage scores. 9 Notably, certain studies reported that the use of uncured monomers led to debonding and deterioration in the characteristics of the filler particles, owing to the reduced photoinitiator over the shelf life of the composite. 9 This degradation also continues in other forms, for instance, coupling agents which are disposed to hydrolysis through ester linkage which formed with the filler particles. 3 Debonding occurs after the stress transfer, which leads to the detachment of the coupling agent from the filler surface, resulting in the degradation of the filler particles. 3
Microleakage can be assessed using different techniques involving biological, electrical, chemical, radioactive, and physical elements. 24 The dye penetration test is a common, simple, inexpensive, and fast technique. 25 The dyes used in microleakage studies include ethylene blue, basic fuchsin, aniline blue, eosin, crystal violet, erythrosine, and drawing ink. 24 Methylene blue is one of the most commonly used organic dyes, and its concentration varies between 0.5% and 5%. In the present study, after thermocycling, the teeth were stored in 1% methylene blue for 24 h. 26 The sectioned teeth were observed under a stereomicroscope by two examiners in a blind framework. In the case of a disagreement among the microleakage scores, the researchers observed the teeth again, and the inferior score was selected. The microscopic observations were analyzed using the ISO microleakage scoring system (ISO/TS 11405:2003), according to which, the dye penetration was represented by numerical values between 0 and 3 for the occlusal and gingival regions. 27 In addition, the samples were observed using a SEM.
Microleakage can be prevented by varying the characteristics of the filler particles to enhance the rigidity and modulus of elasticity of adhesive systems. Specifically, the filler content and size considerably influence the performance of adhesive systems. 28 Nanofilled composites have been produced by increasing the volume of the filler loading by 60%. 29 Although nanosized filler particles are used in nanofilled composites, a combination of nanomeric and conventional filler particles is used in nanohybrids. 30 In the present study, nanofilled and nanohybrid dental composites and their two year expired equivalents were considered to clarify the effect of not only the expiration date, but also the type of dental composites on the microleakage scores. However, no statistically significant difference in the microleakage scores was observed between the two types of dental composites, likely because of the similar characteristics of these composites. In a previous study, no difference was observed between the flexural strength and modulus of expired and non-expired composites 15 months beyond the expiration date. 31 Another study reported that six-month-expired conventional and bulk-fill dental composites did not exhibit notable changes in the hardness and water sorption compared to the non-expired variants. 6 However, the hardness, roughness, and conversion degree of dental composites were noted to be adversely affected six months beyond the expiration date. 8 The differences between the results of these studies may pertain to the storage conditions and chemical compositions of the materials.
When using universal adhesives, total etch and self-etch adhesive techniques may be applied. 32 In the present study, the resin–dentin bond quality of expired and non-expired universal bonding was evaluated in terms of microleakage. Certain defects may occur as a sign of degradation between the resin and dentin 33 ; however, no difference in the statistical microleakage score was observed among the eight groups considered in this study, pertaining to different combinations of expired and non-expired dental materials. This lack of statistically significant changes in terms of the microleakage scores may be related to the adopted storage conditions (in dark and refrigerated conditions, as recommended by the manufacturers), in line with those of the previous study. 3 Such conditions can likely enhance the shelf life by slowing the decomposition of the initiators.
It must be noted that this finding is not in line with that of Nidhi et al’s study 9 which argues that expired dental composites may be used with the combination of non-expired dental bondings. The universal bonding agent used in this study involved a polyalkenoic copolymer. 34 The long-term performance of this bonding can likely be attributed to the presence of this copolymer, which interacts with the calcium in hydroxyapatite. 35 The present in vitro study involved certain limitations. Tooth-related differences and different results can be obtained when expired and non-expired materials are applied to the mesial-distal cavities on the same tooth. Several patient-related factors such as masticatory forces, salivary characteristics, and diet were not considered. Future work must be aimed at examining dental materials that have been expired for more than two years, taking into account the patient-related factors. In addition, it is necessary to further examine the impact of storage conditions and different mechanical properties and cytotoxicity. Biocompatibility studies should be done to evaluate these materials.
Conclusion
The results of the in vitro study suggest that two year expired dental composites and bondings which have been maintained under proper conditions do not have any significant difference in terms of the microleakage scores. Thus, the expired dental composites and bondings may be used for several simple clinical procedures like temporary restorations. The results of this study should be supported by further research to reach a definite conclusion.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.