
Abstract
Aim:
Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy (APECED) is a rare, highly variable disease with significant oral health impacts. The aim of the study is to examine the existing evidence base surrounding the oral health impacts of APECED and consider the wider clinical significance of the condition relevant to the provision of pediatric dental care.
Materials and Methods:
The evidence surrounding APECED and the oral health impacts obtained from a review of multiple databases was qualitatively summarized in the form of a literature review. A case study was used to illustrate the relevance of literature in caring patients with APECED.
Results:
The literature describes a broad range of impacts from APECED, although it is characterized by chronic candidal infection, autoimmune hypoparathyroidism, and Addison’s disease. Oral manifestations of APECED appear frequently and can present early. Developmental defects of the teeth affect a large proportion of patients with APECED and together with candidiasis, characterize the key oral manifestations of the disease. An enhanced preventive and minimally invasive approach to oral health care is recommended for these patients in light of the complexities of their medical condition.
Conclusion:
Patients with APECED require careful multidisciplinary care to ensure that the optimal oral health outcomes are achieved.
Introduction
Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy (APECED) is a rare monogenetic autosomal recessive disease characterized by the destruction of target organs by cellular and/or antibody-mediated attack. 1 The key features of the syndrome are most commonly chronic candidal infection, followed by autoimmune hypoparathyroidism and Addison’s disease. 2 It is associated with mutations in the autoimmune regulator (AIRE) gene which code for the AIRE transcription factor. 1 This transcription factor is involved in immune tolerance mechanisms and contributes to the negative selection of autoreactive T-lymphocytes in the thymus, lymph nodes, and spleen. The condition is particularly rare, with an estimated prevalence between 1 in 1,000,000 and 9 in 1,000,000. 3 Females are affected twice as often as males, with an increased prevalence in populations with high levels of consanguineous marriage because of the autosomal recessive inheritance pattern. 3
Given the systemic nature of this multifaceted condition, some degree of impact on the developing dentition is to be expected, although the nature of this has not been widely explored. The following literature review examines the existing evidence base surrounding the oral health impacts of APECED and considers the wider clinical significance of the condition relevant to the provision of pediatric dental care. This is illustrated with a case study outlining the dental management of a young girl with APECED.
Materials and Methods
This is a narrative review of the literature which is based on a search of the StarPlus database. This is a University of Sheffield database which includes Google Scholar, PubMed, MEDLINE, OvidSP SCOPUS, SAGE, and ScienceDirect. The initial search on StarPlus was based on the key words “APECED,” “Autoimmune polyendocrinopathy- candidiasis-ectodermal dysplasia,” “dental,” and “oral health.” Relevant bibliographic information was also identified by hand searching. The search was undertaken on January 28, 2020. The search results were reviewed by one author (A.G.) for relevance. All study designs were included and there was no restriction on time period searched. Published studies in English were included. The included studies were reviewed by two authors (A.G. and H.R.) and a narrative review produced based on the Scale for the Assessment of Narrative Review Articles (SANRA) criteria.
Clinical Manifestation and Diagnosis
The clinical picture of APECED is highly variable and often progresses with age. 4 While the disease commences in childhood, other manifestations can continue to appear up to the fifth decade of life. 5
Oral candidiasis is typically the first manifestation of the disease, usually between the ages of 3 and 5 years for which families may seek the opinion of a dentist. 4 While dental professionals may be familiar with the presentation of oral candidiasis, the cause should be investigated thoroughly, considering APECED as a potential but rare, differential diagnosis.
The next clinical feature to arise is hypoparathyroidism which typically presents within the first 5 years. This is followed by adrenal insufficiency which may take another 5 years to clinically manifest. The timing of these manifestations is dependent on the development of self-antigen-targeting autoantibodies. 2 These conditions are discussed in greater detail later in this paper.
The diagnosis of APECED is understandably challenging because of the rarity of the condition, the wide variation in its presentation, and the potential differential diagnoses. The literature states that any two of the following three key conditions should be observed to define the syndrome: (a) hypoparathyroidism (HPT; present in 80% of patients), (b) adrenal failure (>70%), and (c) chronic mucocutaneous candidiasis (CMC), although in cases where patient’s sibling is affected, just one of the three criteria is sufficient for initial diagnosis. The presence of organ antibodies or more general antibodies, such as anti-interferon AC, can support a diagnosis, although molecular analysis is required for confirmation. 3
Genetic testing and counseling of APECED patients and their relatives will aid in expedited diagnosis, although prenatal testing is not routinely recommended. 3 Differential diagnoses include immune dysregulation polyendocrinopathy enteropathy X-linked (IPEX) syndrome and, principally, autoimmune polyendocrinopathy type 2. The main manifestations of both syndromes include the development of multiple autoimmune disorders, specifically of the endocrine glands, resulting in a similar initial presentation to APECED. 3
General Characteristics
The majority of the features of APECED result from the body’s immune system, attacking the network of hormone-producing glands. 2
Hypoparathyroidism is the most common autoimmune endocrine involvement, affecting 79 to 96% of individuals with APECED. 6 Hypoparathyroidism occurs in APECED when the parathyroid glands fail to secrete sufficient amounts of parathyroid hormone (PTH) because of autoimmune destruction of the parathyroid glands. 7 This hormone is important for the regulation of calcium and phosphorous levels in the bloodstream. 8 Diagnosis is based on biochemical measurements of serum calcium and reduced levels of PTH. 7 Symptoms of hypoparathyroidism include numbness around the mouth, hands or feet, seizures, low blood pressure, dental problems, and coarse/brittle hair. 8 If left untreated or controlled poorly, hypoparathyroidism can lead to cardiac arrhythmias and signs of congestive heart failure. 7
Addison’s disease is another endocrine disorder commonly seen in APECED. It has been observed in all age groups and affects around 1 in 100,000 people. 9 It occurs when the adrenal glands are damaged, resulting in insufficient production of cortisol and aldosterone hormones. 10 Adrenal failure most commonly presents with coexisting mineralocorticoid and glucocorticoid deficiency. 6 It is commonly unrecognized in the early stages of its manifestation which can result in life-threatening crisis. Symptoms of the disease begin gradually and often start with chronic fatigue, hyperpigmentation of the mucus membrane and skin, reduction in appetite, generalized weakness, hypotension, and weight loss. 9 Hyperpigmentation of the mucosa and skin usually precedes all the other symptoms by a month to a year. 9 This is important for dental professionals, as hyperpigmentation of the oral mucosa may be the first observed manifestation of Addison’s disease and could lead to a prompt diagnosis for the patient. 11
Additionally, the following autoimmune manifestations are common: intestinal malabsorption, atrophic gastritis, autoimmune hepatitis, alopecia (hair loss), vitiligo (loss of skin pigment), ungual dystrophy (nail wasting), keratoconjunctivitis and rheumatologic, bony, muscular, renal, bronchiol, and hematologic impairments. Rarer pathologies affecting these patients include ovarian failure, diabetes, autoimmune thyroiditis, and lymphocytic hypophysitis. 3 It should be noted that splenic atrophy increases the likelihood of severe infections 5 which may have an impact on the severity of dental infections.
Oral Health Impacts
Oral health manifestations of APECED have been reported minimally; however, the mouth appears to be affected early and frequently.5,12
As the first manifestation of APECED, CMC affects the mucosa of the mouth, nails, and rarely the genitals. This places individuals with APECED at risk of developing oral cancer at a younger age, even in the absence of risk factors such as tobacco and alcohol use, immunosuppression, and genetic factors. 13 Furthermore, the progression of cancer in APECED patients is more rapid when compared to non-APECED patients. 13 A Finnish study showed 10.5% of APECED patients over 25 years of age with CMC developed squamous cell carcinoma of the oral cavity or of the oesophagus. 4 This highlights the importance of controlling candida infections in APECED patients with rigorous antifungal treatment. 13
Developmental defects of the teeth affect a large proportion of patients with APECED and, together with candidiasis, characterize the main oral manifestations of the disease. 5 Enamel defects are considered to be the most distinguishing ectodermal manifestations of APECED. Perheentupa reported that enamel defects were present in 75% of a cohort of 89 Finnish patients with the condition. 14 Similarly, McGovern and coworkers reported that 12 out of 16 patients (75%) with APECED displayed enamel defects. 12 The etiology of these enamel defects, however, remains unclear.
Developing dental enamel is extremely sensitive to genetic, nutritional, metabolic, infective, and immune diseases and unlike bone, it permanently records systemic and/or local stresses. 15 Hypoparathyroidism is known to cause alterations in the levels of calcium and phosphate metabolism and has been suggested to have a number of impacts on the developing dentition.7,16 As such, atypical oral findings are relatively common in patients with hypoparathyroidism. Case reports have described an increased incidence of hypodontia, microdontia, shortened roots, enamel hypoplasia, malformed roots, enlarged pulp chambers, pulp calcifications and delayed tooth eruption in patients with hypoparathyroidism. 17 These findings are attributed to low–serum calcium levels because of reduced PTH, coinciding with dental development. 7
Disturbances to the mineralization of dental hard tissues have been shown to occur as a result of altered mineral levels in both human and animal teeth. 18 As a result, a number of studies attribute enamel defects of APECED to hypoparathyroidism. 17 Conversely, supporters of the autoimmune theory uphold that enamel hypoplasia is independent of hypoparathyroidism and caused by an autoimmune attack on the enamel organ.5,15 Evidence for the latter includes cases in which enamel hypoplasia is present in patients with APECED, in the absence of hypoparathyroidism. 6 Additionally, microanatomical examination reveals several alterations to the enamel, while the dentine remains normal or slightly altered. 16
While enamel hypoplasia may not be initiated by hypoparathyroidism, it may intensify the damage caused to the enamel. 16 Additionally, while enamel hypoplasia is observed in many patients before hypoparathyroidism manifests, it should be noted that calcium and phosphate alterations arise long before the clinical onset of hypoparathyroidism. 16 As such, these biochemical alterations may affect enamel formation, while hypoparathyroidism remains undiagnosed. 5 In order to clarify this, a study comparing the onset of occurrence of hypoparathyroidism compared to the development and extent of enamel hypoplasia would be required. 16
Enamel defects in individuals suffering from APECED most commonly appear as grooves or rows of pits distributed horizontally around the circumference of the crown. 12 The areas vary in width and depth, but sometimes a large portion of crown is hypoplastic. 16 Both hypomineralized and hypoplastic defects have been reported; however, it was found that hypoplasia was more prevalent in the APECED group. 16 The teeth most commonly affected in the study by McGovern and coworkers were incisors, premolars, and second permanent molars. 12 However, Perniola and colleagues reported canines to be the worst affected. 16
Enamel defects tend to affect the permanent dentition only and are rarely seen in primary teeth, hence the onset of the process interfering with amelogenesis is thought to occur after birth.15,16 While the enamel defects do not become evident until the eruption of the teeth, microscopic analysis shows the enamel defects dating back to the time of tooth development. 15 Amelogenesis of a permanent tooth spans over several years, therefore damage to enamel may precede the diagnosis of APECED. The study by Lukinmaa et al 15 proved inconclusive regarding the pathogenesis of the enamel defects in APECED patients, noting that the distribution pattern corresponds to the sequence of tooth development, while the defects appear as horizontal bands in otherwise healthy enamel. 15
Further to the presence of enamel defects, McGovern and coworkers found that the overall oral health of patients with APECED was poor in comparison to age- and gender-matched groups of healthy controls. 12 In particular, caries experience, enamel erosion, and periodontal disease were more prevalent in the APECED group. A possible etiological factor could be that medications taken by patients with APECED are cariogenic or have erosive potential. Consideration should be given to the frequency of consumption of these medications which may increase during periods of illness. 12
Plaque accumulation may also be increased in this group of patients because of sensitivity resulting from the presence of enamel defects, as well as oral discomfort arising from longstanding oral candidiasis. These conditions present a challenge to the maintenance of good oral hygiene which could explain the increased prevalence of periodontal disease in individuals with APECED. 12 Nonetheless, a potential systemic cause of periodontal disease should be investigated further.
Increasing evidence suggests a potential role for the skin, oral, and gut microbiotas in the pathogenesis of autoimmunity. 19 Bruserud et al 19 described that how the oral microbiota in APECED patients is altered compared to healthy controls. Additionally, the Sjögren-like syndrome without extractable nuclear antigen antibodies has recently been described in APECED patients. Reduced salivary flow rate alters the oral microbiota and increases caries prevalence. Nevertheless, it remains unclear whether an altered microbiota causes disease manifestations, or the altered microbiota is an effect of disease components. 19
Management
General Management
There are a multitude of potential endocrine manifestations and complications that can arise in patients with APECED as all hormone-producing glands can be affected, hence specialist care in diagnosis, treatment, and long-term management is required. 20 Management of hypoparathyroidism typically centers on the use of activated vitamin D analogues and calcium supplementation. 21 The literature suggests a growing interest in the use of synthetic PTH replacement for children and young people with poorly controlled hypoparathyroidism. 21 Hormone replacement, such as this, is also key to the management of other endocrine disorders of APECED including Addison’s disease and diabetes. 21
Management of Addison’s disease involves glucocorticoid and mineralocorticoid replacement. Replacement should resemble the natural cycle of corticosteroid release. Children have a much higher mineralocorticoid requirement (dosage depends on the age and weight of the child and the severity of the condition) and they may need salt supplementation. 10
Medication regimes may need to be adjusted to account for additional stress or strain that an individual with Addison’s disease may experience. 11 The patient’s endocrinologist should be consulted if the patient experiences illness or infection, an operation, dental or medical procedure, or an accident, as an increased dosage may be required to ensure the level of corticosteroid is maintained. 9
Patients with vitiligo should avoid friction or trauma to the skin to reduce the incidence of new depigmentation, while prescription of topical corticosteroids and certain immunomodulators have been found to be effective at delaying the progression of the condition. 22
The psychological impacts that a diagnosis, such as APECED, can have on a patient should not be underestimated. Chronic illnesses present in children and their parents with the acute stress of diagnosis, followed by the long-term stress of managing the condition. 23 Patients with APECED will be under the care of numerous medical teams and may suffer from appointment attendance burnout, additionally chronic illnesses in childhood can cause significant stress. Both these factors can lead to failed attendance to appointments and lack of compliance with medications or disease management regimes. A patient’s psychological needs must also be considered and managed carefully alongside other management of the condition. 24
The long-term prognosis of APECED is highly variable and can be worsened by the development of oral or esophageal squamous cell carcinoma, sepsis, and renal failure. 20 The average life expectancy is around 40 years of age, yet this may vary considerably depending on the severity of the component disorders. 3
Dental Management
Treatment of oral manifestations of the disease may often take second place in terms of priority because of the severity of other manifestations affecting the patient. Nonetheless, the oral pathologies require attentive, specialized care. 12
Treatment for candidiasis most commonly involves a long course of oral systemic antifungal treatment. This also presents a challenge as some patients develop resistance to azole antifungals, following years of treatment. 14 Candidiasis preferentially affects the oral mucosa causing a mild form of intermittent angular cheilitis. More severe cases include inflammation of most of the oral mucosa, hyperplastic CMC, and atrophic form with leukoplakic areas. It is acknowledged that persistent oral candidiasis and an associated sore mouth may present difficulties in maintaining good oral hygiene. 12
APECED patients are at an increased risk of developing squamous cell carcinoma because of persistent oral and esophageal CMC. 4 The increased risk should be highlighted to general dental practitioners who should be particularly vigilant during soft tissue examinations and should refer any changes in the oral mucosa or suspicious lesions to a specialist in oral medicine urgently. 13 This further highlights the importance of communication, information distribution, and shared care between specialist and general dental care providers in these patients.
The dentition of these patients is often weakened by hypoplasia of enamel making the patients prone to caries. 16 Patients with APECED should be on a strict preventive regime to support oral health. 12 This should involve, specifically, tailored oral hygiene instruction and dietary analysis, paying particular attention to any medications and nutritional supplements taken and their cariogenic and erosive potential. 25
Hypoparathyroidism has a range of diverse oral and extraoral manifestations. Osteoporosis is a common finding, frequently affecting the mandible. Intraoral findings related to hypoparathyroidism include pulp canal obliteration, alterations in dental eruption, loosening and spacing of teeth, malocclusions, cessation of dental development, hypodontia, microdontia, and development of brown tumor. 26 Dental management of patients with hypoparathyroidism requires special consideration and liaison with the patient’s endocrinologist is advised prior to any surgical intervention.
Further to the effects described above, APECED may have serious implications for patients during dental treatment. Adrenal crisis is a rare but potentially lethal medical emergency, most commonly triggered by stressful events (infection, trauma, and surgery). 11 APECED patients are more commonly affected because of reduced adrenal reserve as a result of Addison’s disease, meaning the body is unable to secrete sufficient amounts of steroid required during periods of increased stress. 4 The clinical presentation of adrenal crisis occurs rapidly and includes fever, gastrointestinal complaints, hypotension, and tachycardia. Prompt diagnosis and treatment are required to prevent hypovolemic shock and cardiovascular failure. 11 While there is an absence of reports in the literature of adrenal crisis occurring as a result of dental treatment in a patient with APECED, the risk remains. 11 Liaison with the patient’s endocrinology team is essential, prior to any treatment, to ensure appropriate cover is provided.
Lastly, APECED is also associated with the development of diabetes, hence a full periodontal examination is recommended. Additionally, sources of infection, such as a tooth abscess, must be dealt with rapidly to prevent serious spread of infection. 27
Case Report
A 12-year-old female attended the joint pediatric- restorative dentistry clinic for management of visible enamel defects and generalized spacing of her dentition. Patient informed consent was taken before clinical examination. Medically, the patient was diagnosed with APECED when she was 5 years old. Since her initial diagnosis, the patient was also diagnosed with hypoparathyroidism and Addison’s disease. Steroid cover was therefore required for invasive procedures or periods of illness. She had no known allergies and a previous general anesthetic was uneventful. Others related medical history included ovarian failure, alopecia, vitiligo, and nail dystrophy.
Medications hydrocortisone, fludrocortisone, alfacalcidol, and oestrogen hormone replacement therapy were patch taken.
The patient had previously been seen on the pediatric dentistry clinic since the age of 8. At this time, the patient had received direct composite veneers on her incisors and resin fissure sealants on her first permanent molars. The veneers had fractured multiple times which was the patient’s main complaint. She wished to be provided with a longer lasting solution and was keen to address the generalized spacing of her dentition.
Clinical Examination
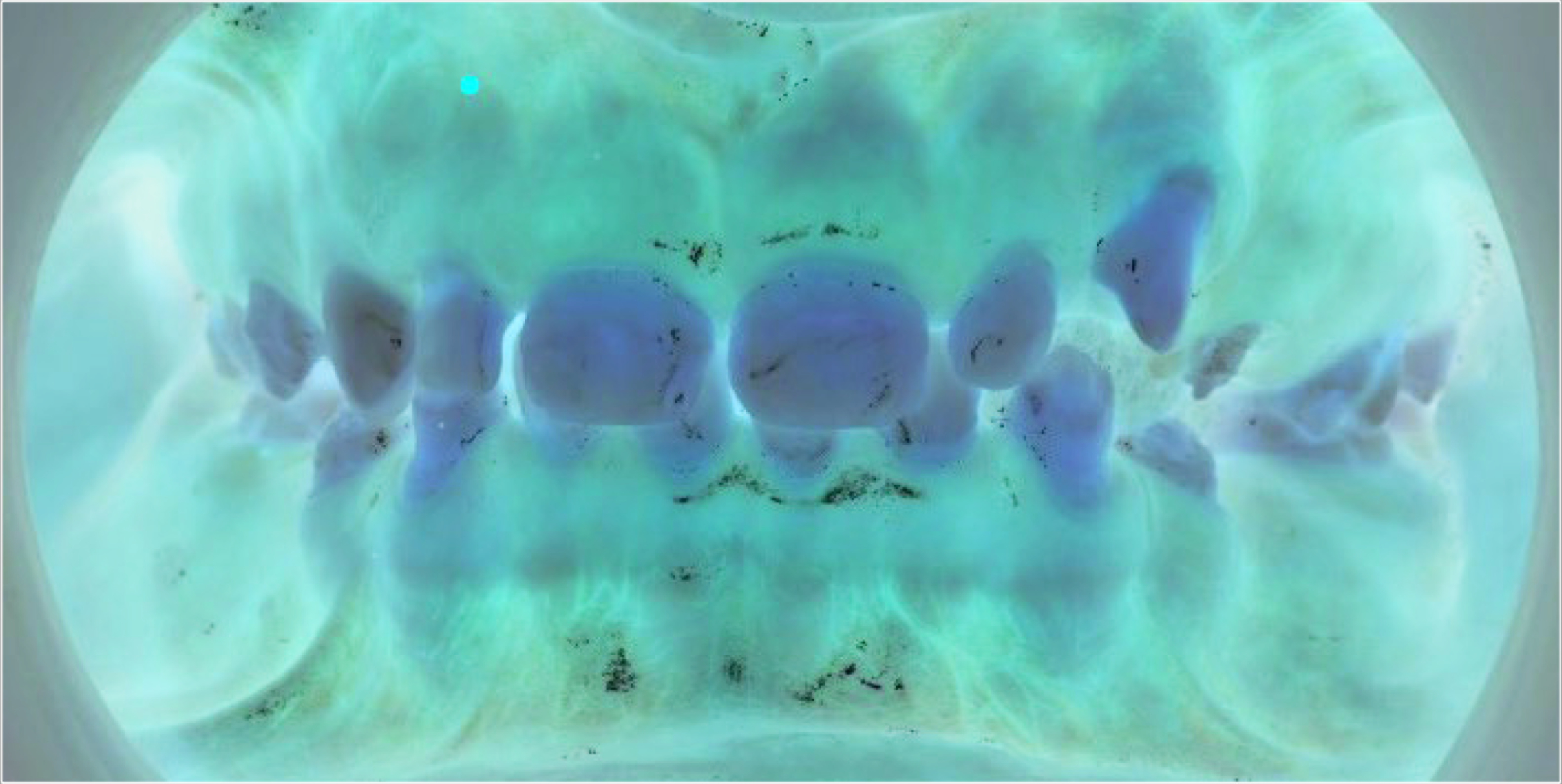
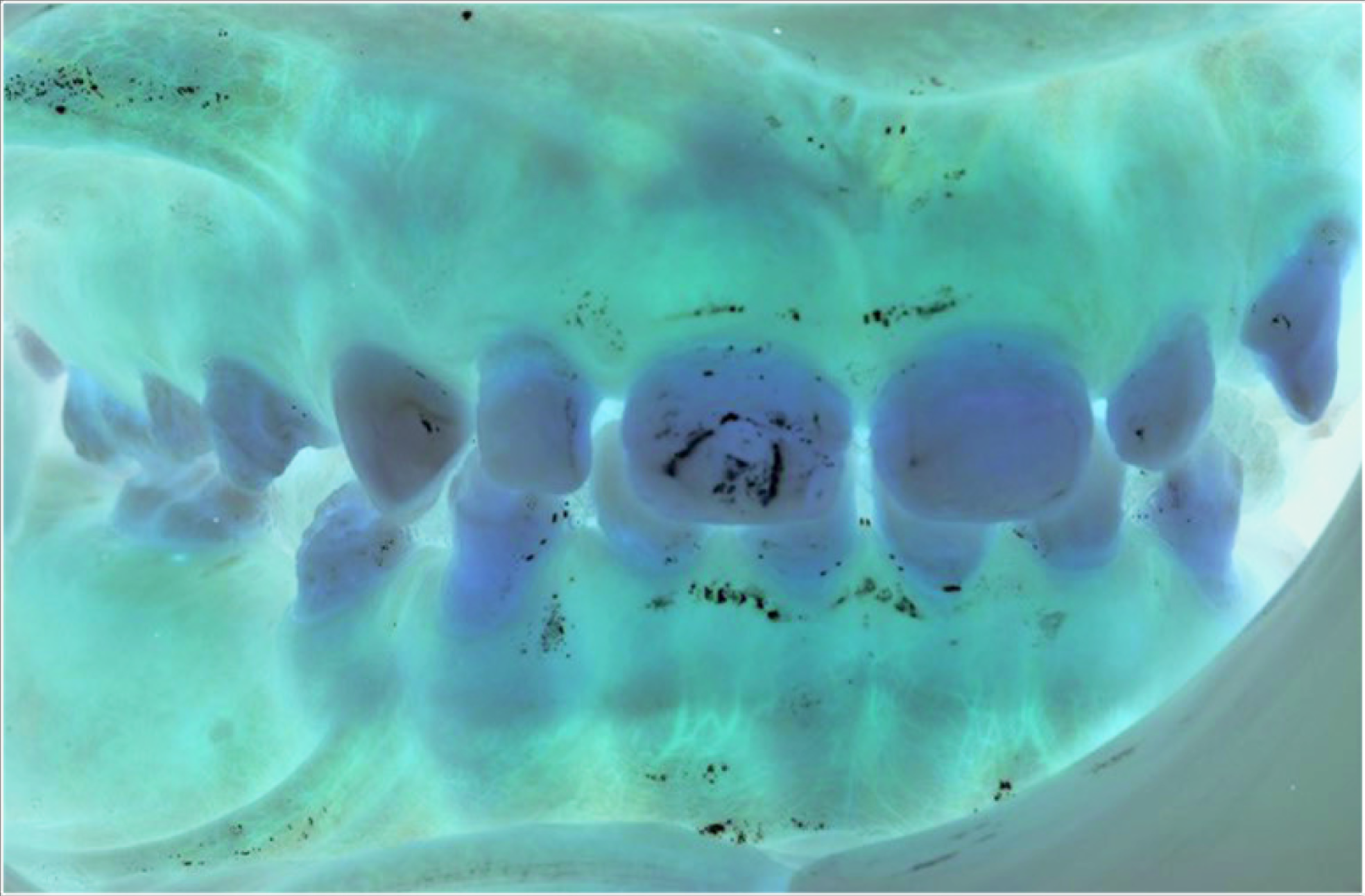
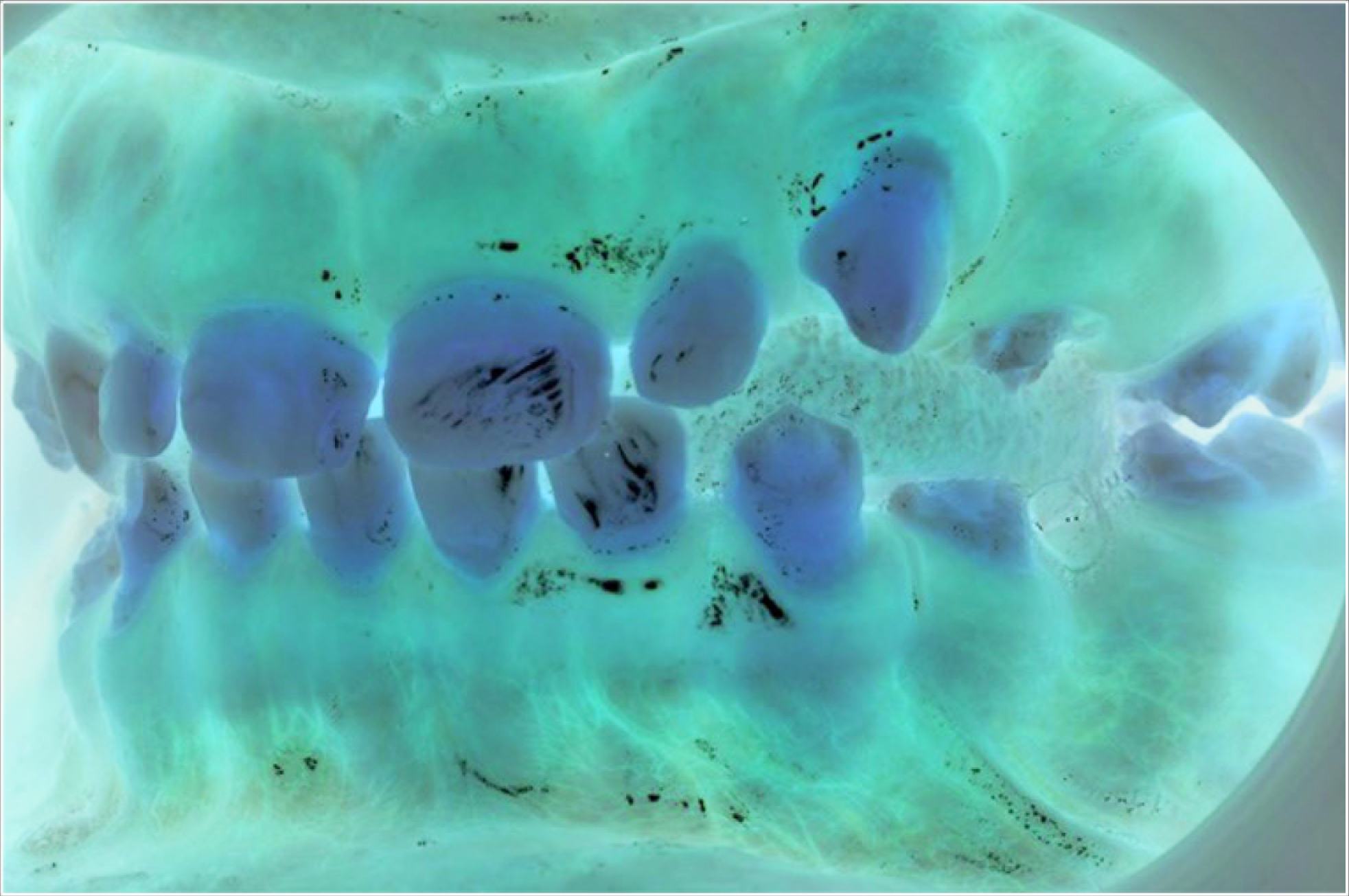
Extraoral examination revealed sparse hair and generalized hyperpigmentation. Intraoral examination showed the patient was in the late mixed dentition. There was generalized enamel hypoplasia, with reduced enamel thickness (Figure 1). A band of macroscopically unaffected enamel was seen around the cervical half of the permanent molar crowns (Figure 2A and B). Upper right 3 was unerupted but palpable buccally, while the upper left 3 was partially erupted. Oral hygiene was suboptimal with plaque retention on roughened enamel surfaces. Diagnoses included chronological hypoplasia, high caries risk, unerupted Upper right 3, and retained Upper right C.
Initial Presentation at the Joint Pediatric Dentistry-Restorative Dentistry Clinic
Right and Left Buccal Images Demonstrating the Generalized Enamel Hypoplasia
Treatment
In the first instance, a preventative regime was adopted. Oral hygiene instruction, application of 5% topical fluoride varnish, and resin fissure sealants (Helioseal, Ivoclar Vivadent) were placed on the first permanent molars. Existing composites were removed (upper right 2, upper right 1, upper left 1, upper left 2, lower right 2, lower right 1, lower left 1, and lower left 2) (Composite restorations were placed using crown formers (3M), including lower right 4, lower left 4, upper left 5, upper right 5, lower left 5 and lower right 5. LR5. Composite restorations (Filtek 3M) on lower right 2, lower right 1, lower left 1 and lower left 2 were initially replaced using a laboratory-made stent; however, the patient was not happy with the esthetics. Once the composites were replaced using crown formers, esthetics were greatly improved, and the patient was happy with the appearance. The upper right 3 was monitored and eventually erupted in a buccal position and mesially angulated (Figure 3). It was clear from a periapical radiograph that the upper right C required extraction. Consultation was required with the patient’s endocrinology team regarding precautions to take prior to extraction. The upper right C was extracted with additional steroid cover prescribed by the endocrinology consultant. An upper removable appliance was provided by the orthodontic team to maintain the space for the upper right 3 and encourage spontaneous eruption. As the upper right 3 erupted, the enamel was also found to be hypoplastic with a roughened surface. Once the tooth had fully erupted, composite restorations were placed on upper right 3 and upper left 3 using crown formers.
It is well documented that adhesion of orthodontic brackets to hypoplastic enamel can be challenging. The bond strength achieved is often poor and can result in multiple bracket failures and prolonged treatment times or compromised outcomes. 28 Moreover, there is also a risk of causing enamel damage on removal of the brackets. Following orthodontic consultation, it was decided that treatment of the patients’ malocclusion would therefore best be managed using Invisalign treatment. This approach also helped avoid damage to the composite restorations that had already been provided. The aim of treatment was to improve the alignment of the dentition in the upper and lower arch, accepting some residual space around the lower right 3 and lower left 3. The Invisalign treatment took a total of 15 months and involved the use of 26 upper and 13 lower aligners together with a number of small composite attachments. Following the completion of the orthodontic phase of treatment, the patient was fitted with upper and lower vacuum formed retainers and instructed to wear these on a nightly basis. Figure 4 shows the patient after treatment. Because of the reduced size of the patient’s teeth, bonding was compromised because of the decreased surface area, therefore continuous maintenance of composite restorations was required.
Upper right 3 Partially Erupted in a High Buccal Position
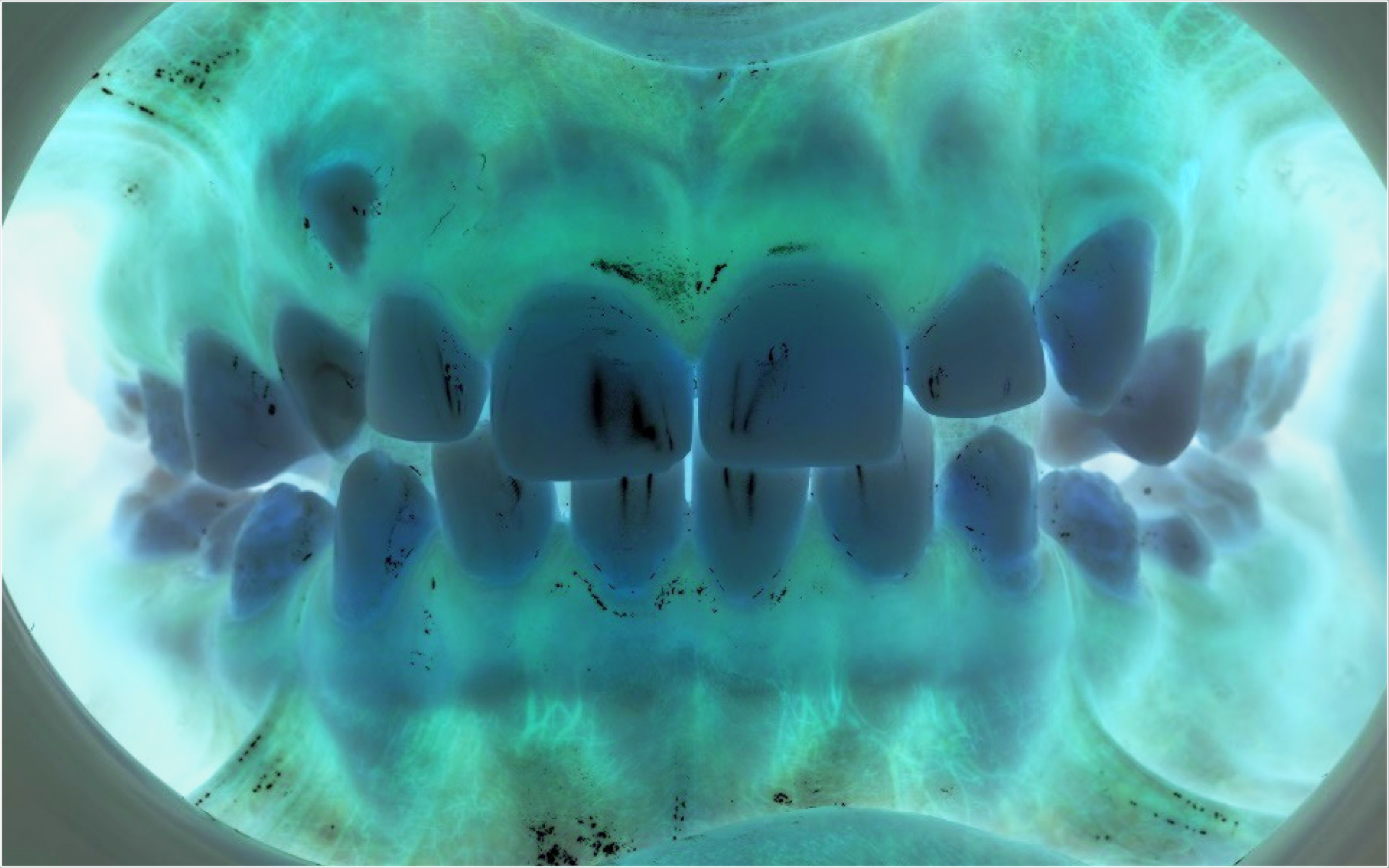
The Patient on Completion of Treatment
Discussion
The case study described above effectively illustrates a number of the complexities involved in the provision of dental care for a child with APECED. As previously reported by McGovern et al, APECED patients are found to experience overall poorer oral health as compared to healthy controls. 12 In the case study described above, a rigorous preventative regime was employed immediately because of the increased risk of caries development, periodontal disease, and erosive tooth surface loss.
Generalized enamel hypoplasia is a relatively common finding in APECED and is reportedly related to both the onset of hypoparathyroidism, and alternatively, because of an autoimmune attack on the enamel organ, known as the autoimmune theory.5,12,15 The horizontal pattern of enamel defects in APECED patients could be compared to chronological hypoplasia. Chronological hypoplasia is a specific type of hypoplasia occurring because of environmental insult, rather than occurring because of a genetic component. 28
As discussed in the above-mentioned case report, the gingival third of the first permanent molars has a band of normal appearance enamel. This band of enamel was formed prior to the environmental insult and fits with the clinical history. It has been proposed that enamel hypoplasia may represent the first component of APECED. However, because of deciduous teeth being unaffected, the lesions are visible following the eruption of permanent teeth. Often time, other components of APECED have become evident. 5 Further studies are required to ascertain the exact pathogenesis of enamel defects in APECED patients. 16
Oral manifestations of the disease were evident in the case above. They included hyperpigmentation of the oral mucosa, a common feature of Addison’s disease that can often lead to a prompt diagnosis. Spacing of the dentition and delayed eruption were also observed, both of which can be features of the dentition seen in patients with hypoparathyroidism. 7 Interestingly, the patient did not present with chronic mucocutaneous candidiasis which is one of the most common manifestations of APECED. However, further review and vigilant examination are required to identify such lesions and provide prompt treatment. This is paired with the fact that APECED patients are at increased risk of developing oral cancer. 13 The patient and parent/guardians should be aware of this increased risk.
As discussed previously, APECED patients are predisposed to developing Addison’s disease and often require steroid cover for invasive treatment. 9 In the case described above, the patient required steroid cover for the extraction of the URC. This involved careful liaison with the patient’s endocrinology team. For this reason and many others, it may not be appropriate for the patient to receive dental treatment in primary care, as this condition often requires specialized care and close liaison with associated medical colleagues. However, even for noninvasive, preventative treatment in these patients, dental professionals should be aware of specific complications and be compliant with mandatory continuing professional development regarding the management of medical emergencies.
Reflecting on the treatment provided, it was considered whether earlier interceptive extraction of URC may have led to a more favorable outcome. While there are a number of studies that have shown that interceptive orthodontics have high levels of success, there is still a limited body of evidence to support this. 28 Additionally, it may have also been more appropriate to delay the definitive composite restorations until orthodontic treatment had been completed. This would then have meant that the patient could undergo conventional fixed orthodontic treatment, rather than Invisalign, avoiding the financial implications that this treatment presents. However, as esthetics were the patients’ primary concern, delaying the provision of composite restorations may have had a negative impact on the patient’s oral health-related quality of life.
In the case described above, regular contact was maintained with the patient’s general dental practitioner. The importance of regular correspondence is clear and should be maintained to ensure that regular recall can be conducted alongside any treatment required in a hospital setting. As this condition poses a significant detriment to the oral health of an individual throughout their lives, dental professionals’ awareness of the condition, and the related risks and difficulties, it poses to maintaining oral health and providing routine dental treatment should be prioritized. This is especially important for pediatric dentists, given that the first symptoms to present in this condition may relate to the oral cavity and occur at a young age.
This narrative review was limited in that there is some literature that may have been omitted, and the included studies may have been at risk of bias or lacking in quality. Nonetheless, a broad, accessible, and informative narrative review was considered preferable to a more specific systematic review.
Conclusion
APECED encompasses a range of associated conditions, each with varying impacts on the general and oral health of children and young people. Clinicians should be aware of the complexities of APECED when providing dental care to pediatric patients to ensure the appropriate management is employed.
Footnotes
Acknowledgements
The authors would like to thank the patient whose care is outlined in this case study and her parents for their help in clarifying details regarding her medical history, and for allowing us to publish details of her care.
Author Contributions
H.J.R. conceived the idea for the paper, provided treatment for the patient described in the case study (excluding orthodontic treatment) and contributed to the development of the manuscript. H.J. and M.S. provided orthodontic treatment for the patient described in the case study and contributed to the manuscript. A.G. conducted the literature review and led the writing of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.