
Abstract
Aim:
This study reviews the importance of selecting implant systems with connection designs that ensure better long-term prognosis of the prosthesis, thus placed.
Materials and Methods:
An electronic search on the PubMed database was done using MeSH keywords (“dental implant OR abutment OR connection AND microleakage OR bone loss”) to review English language articles published since the year 2011, which compared the crestal bone levels and microleakage around various implant–abutment connection designs (external hex, internal hex, and Morse taper). The search screened for articles on human trials and in vitro studies to be included within the review.
Results:
Based on the inclusion and exclusion criteria applied to the preliminary search, a total of four articles were included in the review for evaluating the influence of connection type on peri-implant bone loss, while nine articles were included to study the influence on bacterial leakage across the implant–abutment interface.
Conclusion:
Based on the studies reviewed, the conical connection design proved to be the most biologically stable junctional geometry because of the better microbial seal and the lesser micromovement observed in these types of implants during functional loading. Moreover, this review even emphasizes the need for more longitudinal clinical trials to assess the microbial seal of these connection designs within the actual oral environment to evaluate long-term changes in the peri-implant tissues, and subsequently even factor the prognosis of the planned prosthetic intervention.
Introduction
Through the previous decade, implantology has emerged as a notable therapeutic strategy in clinical dentistry, assisting practitioners in improving the quality of life of a significant demographic fraction of patients. While dental implants have proven to be a suitable substitute to conventional treatment strategies, in certain scenarios, it is rendered as a treatment of choice for the rehabilitation of significant functional, anatomical, or aesthetic problems that have become apparent because of missing tooth/teeth. The implant–abutment connection is defined as a point of contiguity between the surgical and prosthetic stages and must be designed to incorporate sufficient joint strength, rotational stability, prosthetic indexing, and resistance to microbial infiltration. 1 Over the years, different connection designs have been developed with the objective to alleviate mechanical stresses on the prosthetic superstructure and on bone–implant interface and also provide sufficient prosthetic stability.
The implant–abutment connection, broadly, is classified as an internal or external connection. 2 These two implant– abutment connections are differentiated by the existence of an extension of a structure above/under the body of the implant. In external connection implants, there is a discernible extension above the body of the implant; while in internal connection implants, the interface is set into the body of the implant. These interfaces can be further classified as being a slip-fit joint, where a minute space intervenes the mating parts and the connection is rendered passive, or as a friction-fit joint, where no such space is discernible between the mating parts that snugly fit in place. 3 The components are further characterized as being a butt joint, made of two perpendicular flat surfaces apposing one another, or a beveled joint, where the interface is angled either internally or externally. The joined surfaces may even include a component of rotational resistance that provides a lateral stabilizing geometry. This geometrically can be further elucidated as octagonal, hexagonal, conical, cylinder hex, and spline. 2
A microgap at the intervening interface permits microbial infiltration near the epithelial attachment, which consequentially leads to peri-implant bone resorption of an approximate 2 mm apical to the junction. 4 Since two-stage implant systems are in conventional use, they inevitably result in a microgap at the implant–abutment junction; this intervening space provides a favorable niche for bacterial colonization and leads to inflammatory process at the implant–abutment interface. 5 The bacterial infiltrate at the interface has been attributed to the location of the connection and their capacity to fasten the interposing surfaces against each other. 6 This article reviews the influence of implant–abutment connection type on the peri-implant crestal bone loss values and microbial leakage across the connection. The correlation between microleakage and crestal bone loss further elucidates the role of the integrity of the connection on the peri-implant inflammatory status and long-term biological stability of implants of different connection types.
Materials and Methods
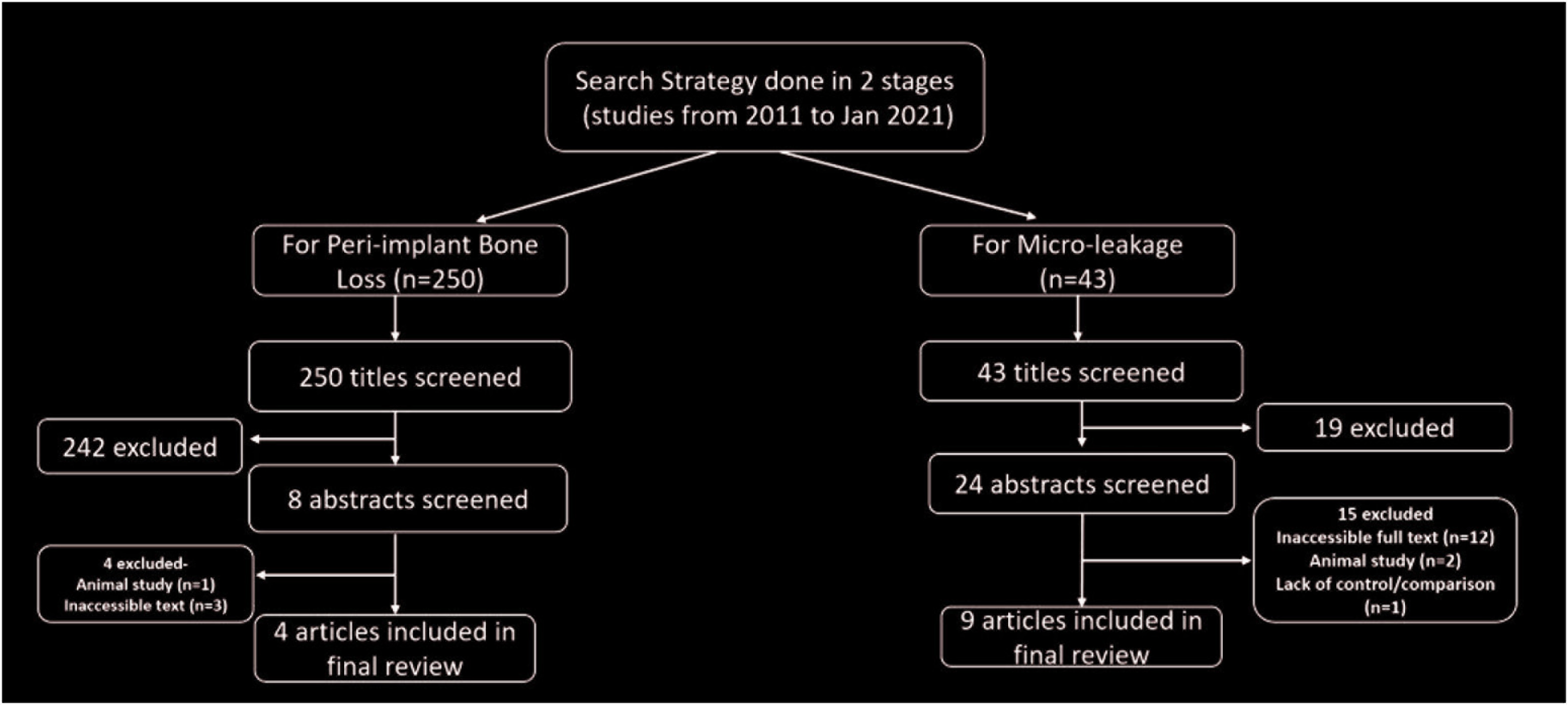
An electronic search was done for English language articles from 2011 to January 2021 in the databases of PubMed/MedLine. The search strategy involved an initial preliminary search for the effect of implant–abutment connection design on the biological stability of the implants using MeSH keywords “dental implant OR abutment OR connection AND microleakage OR bone loss.” Titles and abstracts were searched upon to accurately relate the comparison of different connection designs, i.e., external hex, internal hex, and/or Morse taper (conical connection) based on two distinct parameters—peri-implant crestal bone loss and microleakage/bacterial leakage along the external, internal, and Morse taper connections. The type of studies involved were the studies done on/involving humans only, randomized controlled trials, in vitro studies, and systematic reviews (Figure 1). The studies that were excluded were the ones that did not meet the inclusion criteria and also the animal studies.
Search Strategy for Review
Results
The preliminary search yielded 250 articles when the strategy involved the keywords “dental implant OR abutment OR connection AND bone loss.” Out of them, 242 articles (titles screened) were excluded based on the above-mentioned criteria. Eight abstracts were then screened out of which four fully accessible articles were included in the review. For the strategy involving the keywords “dental implant OR abutment OR connection AND microleakage,” a total of 43 articles were screened. In the initial screening, 19 articles were excluded, while the abstracts of 15 articles were excluded in the secondary screening. Nine fully accessible articles were reviewed to compare the influence of connection type on the bacterial leakage across the implant–abutment connection.
Discussion
The Microbial Interface
A two-piece implant system comprises of the endosteal part (implant body) which is embedded in the alveolar bone in the surgical phase and the mucosal superstructure (abutment) which is affixed after integration of the substructure during the prosthetic phase. Placing the abutment over the implant creates a gap at the intervening interface. 7 This microgap has been quantified within a range of 40 to 60 μm; this gap catalyzes into significant micromovement under functional load which amplifies microbial leakage at the interface. Presence of space near the alveolar crest is also held responsible for the approximate 1 mm bone loss during the first year of functional loading. 8
The type of connection used is one of the salient factors influencing microbial adhesion and proliferation; however, other factors must also be taken into consideration. Factors like the microroughness of the implant surface, the preload values, and the dynamic oral microflora have to be given due consideration as well. 9 To bespeak the microbial leakage along the implant–abutment interface, an in vitro study by Piattelli et al. was carried out on different implant–abutment assemblies using blood serum media inoculated with microbes. The media was incubated in anaerobic condition for seven days with the implants partially and completely immersed in it. The microbial flora from the implants were sampled and incubated in blood agar plates in anaerobic conditions. The study concluded the presence of microorganisms in both the assemblies demonstrating evidently the phenomenon of microbial leakage. 10 Although conical connections have proven to demonstrate a relatively better sealing ability, microgap invariably exists at the interface; therefore, it can be stated that no connection has totally eliminated the microgap formation or has led to a pristine environment within the implant connection. 11
Peri-Implant Crestal Bone Loss
The protracted success of an endoosseous implant counts mainly on the preservation of the contiguous bone. Indeed, the preservation of osseointegration and stability in marginal bone levels is imperative to this success. Peri-implant marginal bone loss is influenced by a multitude of factors which might include the surgical technique, implant positioning, tissue thickness, presence of a microgap at the implant–abutment interface, and the implant design. 7 The norms that define success in implant dentistry are under persistent argument, but the attainment and maintenance of osseointegration are recognized as significant constituents, and the marginal bone loss is therefore a crucial consideration.
The ever-present resorption of up to 2 mm of bone around the implant neck during the first year after functional loading has widely been considered sustainable by the dental fraternity and has even been considered a successful outcome in some classifications and consensus statements. 12 However, osseous stability is anticipated at one year after placement, and a loss of more than 0.2 mm per year is considered unwelcome. 12 Other authors have claimed that in the first year, a marginal bone loss of 1.5 mm, 13 1.8 mm, 14 or 1.5 to 2 mm 15 represents a favorable outcome. A crestal bone loss of less than three threads has also been advanced as a successful criterion,16,17 despite the variance in pitch values among different implant systems.
The platform-switch strategy demonstrated a mitigated epithelial component of the biological width, thus resulting in a conservation of marginal bone levels in both animal and human study models. 18 Consequentially, the implant–abutment connection type, the size of the machined neck, the size of the microgap at the implant–abutment interface, and its insertion relative to the alveolar crest may subscribe to the incessant bone remodeling after implant placement. 19
Biological Review Comparing Various Implant– Abutment Interfaces
Microbial Review of Various Connection Designs—Microleakage/Sealing Capability (Table 1)
Studies Involved in Reviewing Microleakage Along Different Connection Types
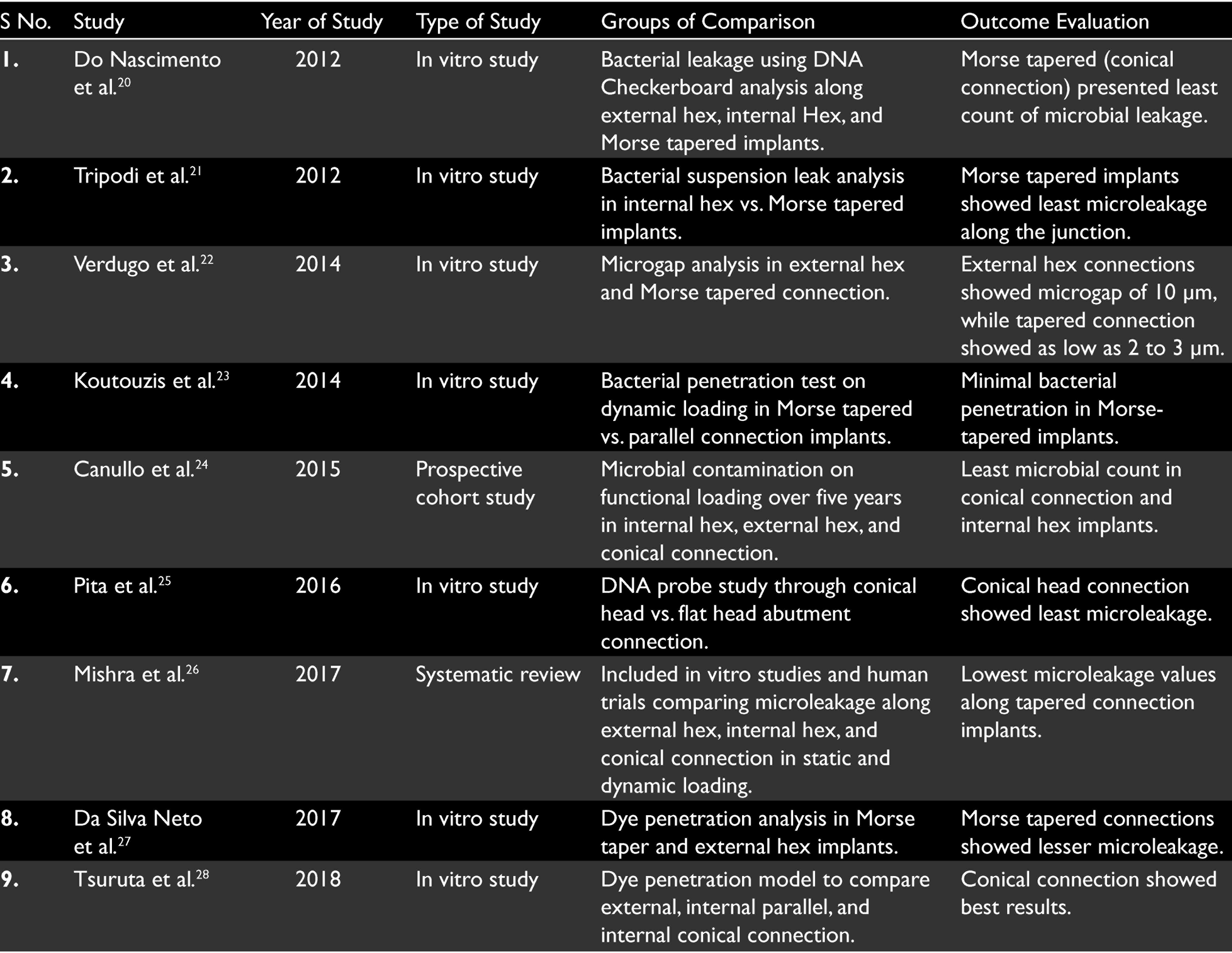
Do Nascimento et al. in 2012 performed an in vitro study to evaluate bacterial leakage from human saliva to the internal part of the implants along the implant–abutment interface under loaded and unloaded conditions using DNA Checkerboard in internal hex, external hex, and Morse tapered implants. In their study, the Morse cone connection presented the lowest count of microorganisms in both the unloaded and loaded groups. Loaded implants presented with higher counts of microorganisms than unloaded implants for external- and internal-hex connections. 20 Tripodi et al. in 2012 evaluated, in vitro, the leakage observed in internal hexagon and Morse taper implant–abutment connections through bacterial suspension technique to observe turbidity in the reactive broth. They concluded that the Morse taper connection showed significantly lesser microbial leakage along the junctional interface. 21 Verdugo et al. in 2014 used external connection implant and conical internal connection (Morse taper) implants in their study. The results of the study showed that less microleakage was shown by Morse taper connection implants then external connection implants. A gap of 10 μm was presented by external connection implant which was more than Morse taper implants with a gap of 2 to 3 μm. When 30-Ncm torque was applied to tighten the abutments, there was decrease in microleakage. The findings were attributed to the lack of creation of a perfect seal at external connections and a friction-lock mechanism at the connection of Morse taper implants. Morse taper implant–abutment connections have a unique design with an internal joint design between two conical structures. The internally tapered design creates high propensity of parallelism between the two structures within the joint space and provides significant amount of friction. 22 Koutouzis et al. in 2014 evaluated microleakage of internal Morse taper connection and found that there was minimal penetration of bacteria down to the implant–abutment interface. Dynamic loading increased the penetration of bacteria as there was micromovement at the interface, which was postulated to cause a pumping effect and subsequently detrimental effects on the marginal bone stability. 23 Canullo et al. in 2015 conducted a five-year follow-up study on humans for different implant connections under functional loading. The results demonstrated that microbial contamination was seen in all the connections. Internal hex and conical connection implants showed less leakage of microbial flora at the peri-implant sulcus and inside the connection than external hexagon implants. 24 Pita et al. in 2016, in their study, tested both conventional flat-head and conical-head abutment screws, in external hex and trichannel internal platform implants, under unloaded condition with 38 microbial species. In both the connections, large populations of microbial species penetrated across the implant–abutment interface. Implants attached with conical head abutment screws showed fewer microbial floras in comparison to conventional flat-head screws. 25 Mishra et al. in 2017, in their systematic review, concluded that external hexagon implants completely failed to prevent microleakage in both static and dynamic loading conditions of implants. Internal hexagon implants mainly internal conical (Morse taper) implants are very promising in case of static loading and showed less microleakage in dynamic loading conditions. They also suggested that the torque recommended by the manufacturer should be followed strictly to get a better seal at the abutment–implant interface. 26 In 2017, Da-Silva Neto et al. compared microleakage across external hex and Morse taper implants in loaded and unloaded conditions using dyepenetration tests in an in vitro environment and concluded the Morse taper connections to have superior microbial seal along the implant–abutment junction. 27 Tsuruta et al. in 2018 conducted an in vitro study comparing external, internal parallel, and internal conical connection for microleakage using a dye-penetration model. They concluded that the conical connection was stable even after the loading in the reverse torque values of abutment screw and it prevented leakage across the microgap between the implant body and the abutment, among the three tested connections. 28
Review Comparing Peri-Implant Crestal Bone Loss Amongst Various Connection Designs (Table 2)
Studies Involved in Reviewing Crestal Bone Loss Amongst Different Connection Types
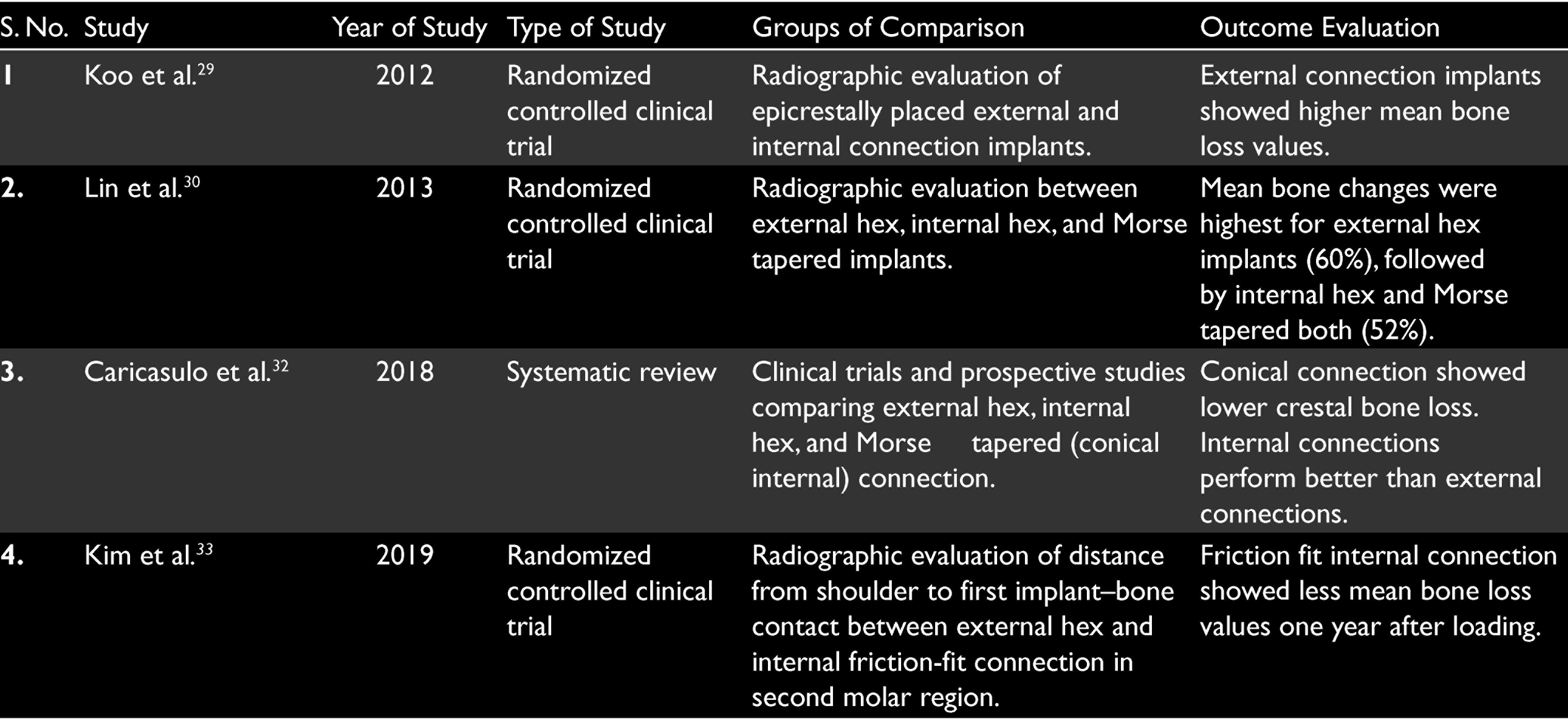
In a comparative clinical trial by Koo et al. in 2012, epicrestally inserted root-form implants (acid-etched surface, microthreads in the neck area, length: 8.5 to 13 mm, outer diameter 4.3 mm) exhibiting either an external or internal implant–abutment connections (20 implants from each group) were followed up for peri-implant crestal bone loss. Radiographic evaluation of linear and angular bone changes after one year revealed significantly higher mean crestal bone loss values for the external connection, when compared with the internal abutment connection. 29 Lin et al. in 2013 [ 30 in their retrospective study comparing bone changes amongst external hex, internal octagon, and conical connections demonstrated that the crestal bone change in the first six months after loading to be within the success criteria as proposed by Albrektsson et al. in 1986, 31 i.e., bone loss <1.5 mm in the first year. The mean changes were in fact, less than 1 mm even after one year for all implants. Crestal bone loss did not differ significantly amongst the groups. Slightly greater changes—60% for external hex and 52% for both internal octagon and internal Morse taper—during the healing phase (before occlusal loading) rather than during the loading phases (three and six months after occlusal loading) were demonstrated. 30 In a systematic review conducted by Caricasulo et al. in 2018, they concluded peri-implant bone loss generally being lower in the short-medium term when internal types of interface are in use. In particular, conical connections were proved to be more advantageous, guaranteeing better seal performances and stability of the implant–abutment interface, and this fact was validated especially by in vitro studies or in vivo works with a follow-up. 32 In a randomized controlled study by Kim et al. in 2019 comparing the influence of implant–abutment connections on the peri-implant crestal bone loss, the authors observed a mean distance from implant shoulder to first bone–implant contact for external connection implants at 0.59 mm while for internal friction fit connections at 0.01 mm. The readings were observed one-year postloading in implants placed to replace mandibular second molars. 33
Conclusion
From the evidence perspective, the influence of implant–abutment connection type on the peri-implant bone loss needs to be further substantiated by more controlled human trials over a longitudinal basis. Under the literary limitations, we have reviewed the various connections available and their influence on the above-mentioned aspects and may unanimously conclude the friction-fit tapered connection to be of biomechanical superiority followed by the internal and the external connections in a descending order, respectively. The review clearly delineates the kind of studies involved in this horizon of implantology and demands for conducting longitudinal human trials to better apply the results in the dynamic oral environment. The homogeneity of the systematic reviews conducted over the years has also upheld the Morse taper concept to be amongst the more acceptable connection on all perspectives. The fact that these results, correlate with the excellent sealing capabilities of the conical connection, bring about a positive correlation between the chances of peri-implant disease in connections with poor peri-implant seal ability.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.