
Abstract
Aim:
One of the main steps in a successful endodontic treatment is determining the correct working length (WL) of the root canal. In this regard, electronic apex locators (EAL) have been widely used for measuring the WL. The accuracy of EALs in determining the WL may be influenced by various factors. This study is aimed to evaluate the effects of apical patency, coronal preflaring, and calcium hydroxide on the accuracy of the EAL.
Materials and Methods:
In this in vitro study, 20 central incisor single-rooted human teeth with fully formed apex were considered. Then, samples were randomly divided into two study groups, ten samples in each group. The WL was determined and recorded at 0.5 mm distance to the apex using Root ZX apex locator before and after creating patency, coronal preflaring, and calcium hydroxide administration. All WLs were measured separately for each tooth and reviewed independently by two experienced operators with extensive experience in using EALs. Paired t test and Wilcoxon signed-rank test were applied and the significant level was at .05.
Results:
Statistical analysis of the obtained data showed a significant decline in the WL after apical patency and coronal preflaring (P < .05). Moreover, WL exhibited a significant enhancement after calcium hydroxide application (P < .05).
Conclusion:
Apical patency and coronal preflaring increased the accuracy of apex locators in determining the WL of the teeth. Besides, calcium hydroxide residues in the root canal reduced the accuracy of the apex locator.
Introduction
The exact working length (WL) determination of the root canal is a critical step in a successful root canal treatment. 1 Previous studies have shown that a loss of WL can increase the failure of root canal treatment. 2 Tactile sense, radiographs, and electronic apex locators (EALs) are among the methods used for WL determination. 3 EALs have been widely used for precise root canal measurements. Several studies have indicated that the EALs can offer the best results in determining the WL.4–6
The accuracy of EALs in determining the correct WL in endodontic treatment is under the influence of a large number of factors, including tooth type and the anatomy of the root canal, pulp’s electrical conductivity, obstruction of the root canal, apical patency, location of the apical foramen, apical foramen size, preflaring of the canal, presence or absence of canal irrigation solutions, type and size of the measurement file, and type of experimental medium.7–10 Preflaring of the root canal during endodontic treatment removes cervical dentin interferences, hence allowing the file to easily reach the apical constriction.5,11 Based on some studies, the preflaring procedure improved the accuracy of the WL and file size determination,12,5 whereas other studies reported contrary results.13,14 However, the preflaring of the root canals and determining file characteristics are controversial subjects in the accuracy of the EALs.
Calcium hydroxide has been applied in the treatment of inflammatory root resorption to arrest the inflammatory process of the periodontium. 15 It was suggested that the diffusion of ions from the root canal increases the pH of the dental tissues, thus, interfering with osteoclastic activity and activating alkaline phosphatases. 16 According to previous studies, calcification, stenosis, and calcium hydroxide residues can affect apex locator accuracy. 17 The apical patency is one of the most important phases in endodontic treatment and preparation that requires small manual files. During apical patency, a flexible small file passively passes through the apex end without diluting or removing the apical constriction.
A previous study has shown that the apical foramen blockage has a negative influence on the accuracy of apex locators, 18 on the other hand, the cervical preflaring presented significantly increased accuracy in the electronic measurements. 16 Also, an in vitro study indicated that the residues of Ca(OH)2 adversely affect the accuracy of Root ZX. 19 To the best of author’s knowledge, there is no information to evaluate the effect of apical patency, coronal preflaring, and calcium hydroxide on EALs. Thus, the aim of this study was to evaluate the effects of apical patency, coronal preflaring, and calcium hydroxide on the accuracy of the Root ZX apex locator for WL determination.
Materials and Methods
Setting and Design
This study was approved by the Ethics Committee of Kermanshah University of Medical Sciences (Code: KUMS.REC.1397.769).
This is an in vitro study performed in the School of Dentistry of Kermanshah University of Medical Sciences between August and November 2018. The sampling method was available and 20 central incisor single-rooted human teeth with fully formed apex were randomly assigned to two study groups. Sample size was determined with an error level of .05 and the power of 0.9. In this study, permanent human single central canal teeth were extracted because orthodontics reasons were eligible. Teeth with open apex, teeth with lesions, calcification or cavities in the root canal, history of previous endodontic treatment, and teeth with severe curvature or obstruction along the root canal were excluded.
Study Methods
For the measurements of the WL, the teeth were mounted in normal saline, then K-file size 10 (Mani, Inc., Tochigi, Japan) was inserted into the root canal, and the WL was determined and recorded at 0.5 mm distance to the apex using Root ZX apex locator (OLYMPUS, J Morita, Suita-shi, Japan). All WLs were measured separately for each tooth and reviewed independently by two experienced operators with extensive experience in using EALs.
To create patency, the teeth were removed from the mount and K-file size 8 was inserted into the root canal and gently over the apex. After creating patency, the teeth were remounted and K-file size 10 was inserted into the canal and the WL was determined by the apex locator.
The teeth were then removed from the mount. Under the stereomicroscope, the K-file size 10 was inserted into the root canal until reaching and extruding apical foramen. The WL was determined at the 0.5 mm distance from the apical foramen. The WL of the tooth canals was measured before and after the preflaring using an apex locator and microscope.
In the next step, a paste made of calcium hydroxide powder (pH = 12.8, pro analysi, Merck, Darmstadt, Germany) was inserted into the canal by a lentulo spiral and a temporary restoration was placed into the access cavity. The teeth were mounted in jelly for ten days. Finally, after washing the canal with 1% sodium hypochlorite solution (NaOCl) and slight filling, the teeth were mounted in saline to determine the WL. In this study, the ranges of ±1.0 and ±0.5 of WL were used as measures to assess the accuracy of the EAL.
Statistical Analysis
The Shapiro–Wilk W test was applied to test the normality of the data. If normal, paired samples t-test was used. If the data are not normal, the Wilcoxon signed-rank test was used. The significant level was .05. All the analysis was performed with SPSS software version 21.0 (IBM-SPSS Inc. Chicago, IL, USA). All data have been presented as mean ± SEM, and the significance level of .05 was considered in this study.
Results
The Effect of Apical Patency on the Accuracy of EAL
The normality of the data distribution was analyzed using the Shapiro–Wilk W test. Regarding the normality of the data distribution, the data were analyzed by paired t-test. The results demonstrated a significant difference in WL before and after apical patency (P < .05).
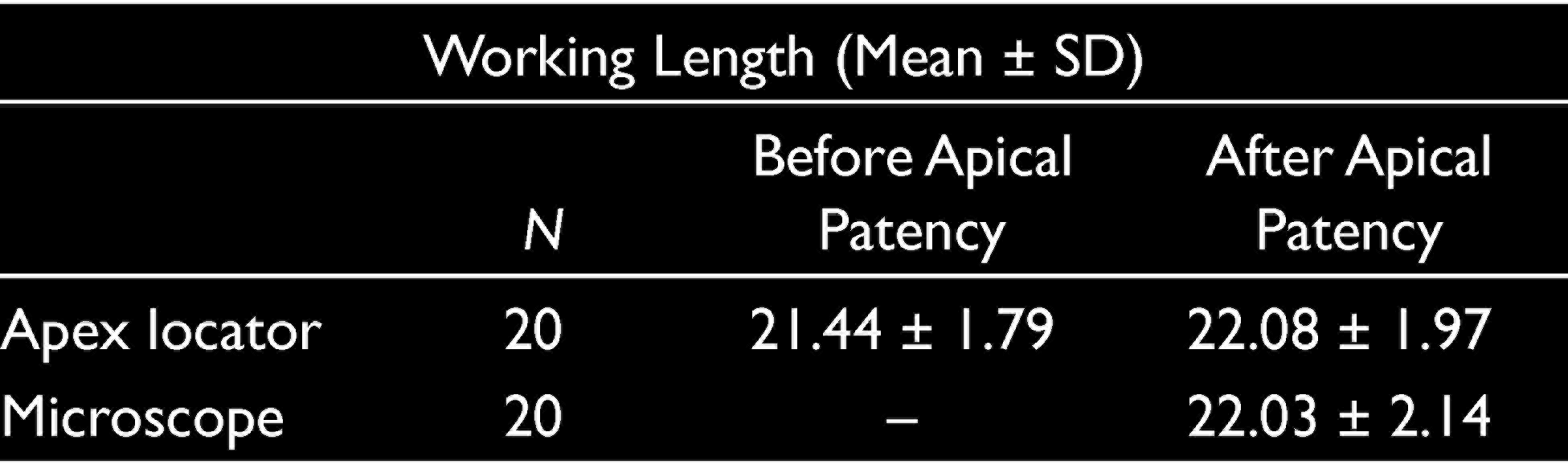
The WL measurement by apex locator before apical patency significantly increased (0.59 mm) as compared to those measured by microscope (P < .05). Under these conditions, the accuracy of the apex locator was 0% in distance 0 to ±0.5 mm, implying that in 0% of the cases, the difference between measurements was less than 0.5 mm. On the other hand, the accuracy of the apex locator was 75% at distances ranging from 0 to ±1 mm. In other words, in 75% of the cases, the difference between measurements was less than 1 mm. The results also revealed no significant differences between WL measured by apex locator and microscope after apical patency (P > .05).
Under the mentioned conditions, the accuracy of the apex locator was 75% in the distance range of 0 to ±0.5 mm. In other words, in 75% of the cases, the difference between measurements was less than 0.5 mm. On the other hand, the accuracy of the apex locator was 100% in the distance range of 0 to ±1mm, implying that the difference between measurements was less than 1 mm in 100% of the cases. Accordingly, apical patency enhanced the accuracy of the apex locator. The data are summarized in Table 1.
Working Length (Mean ± SD) Before and After Apical Patency
The Effect of Coronal Preflaring on the Accuracy of EAL
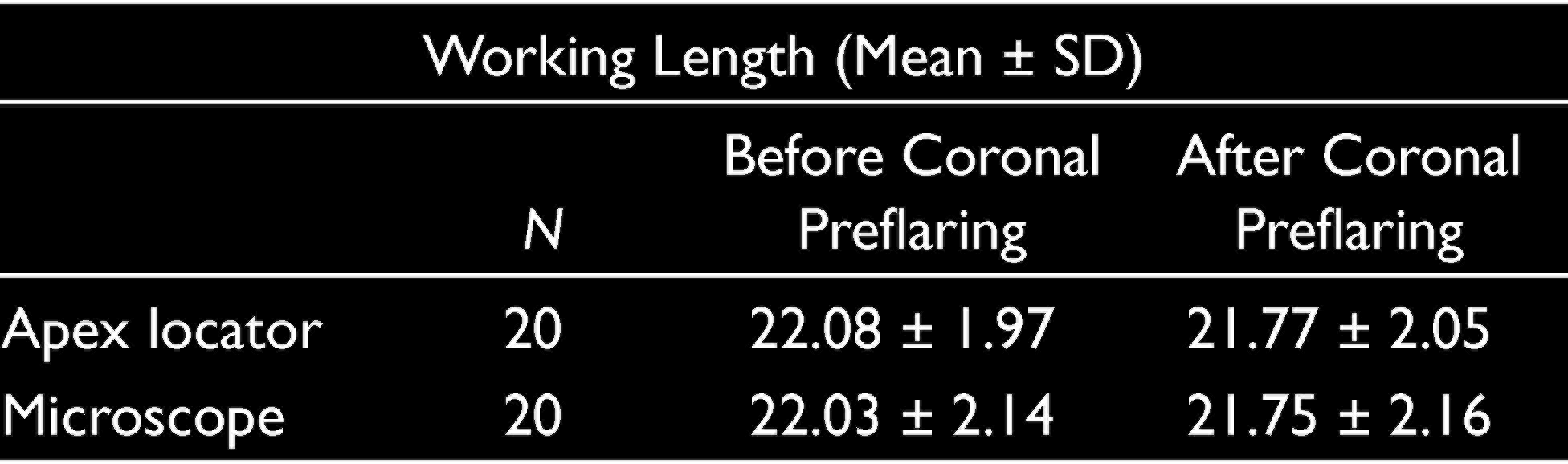
The normality of the data distribution was analyzed using the Shapiro–Wilk W test. Accordingly, the data were not normally distributed, thus they were analyzed by Wilcox sign. The results of WL measurement by microscope and apex locator clarified a drastic decline in the WL after coronal preflaring (P < .05). Conversely, there was no significant difference between WLs measured by microscope and apex locator after coronal preflaring (P > .05).
The accuracy of the apex locator was 85% in the distance range of 0 to ±0.5. Moreover, in 85% of the cases, the difference between measurements was less than 0.5 mm. The accuracy of the apex locator was 95% in the distance range of 0 to ±1. In other words, the difference between measurements was less than 1 mm in 95% of the cases (Table 2). Therefore, coronal preflaring improved the accuracy of the apex locator.
Working Length (Mean ± SD) Before and After Coronal Preflaring
The Effect of Calcium Hydroxide on the Accuracy of the Electronic Apex Locator
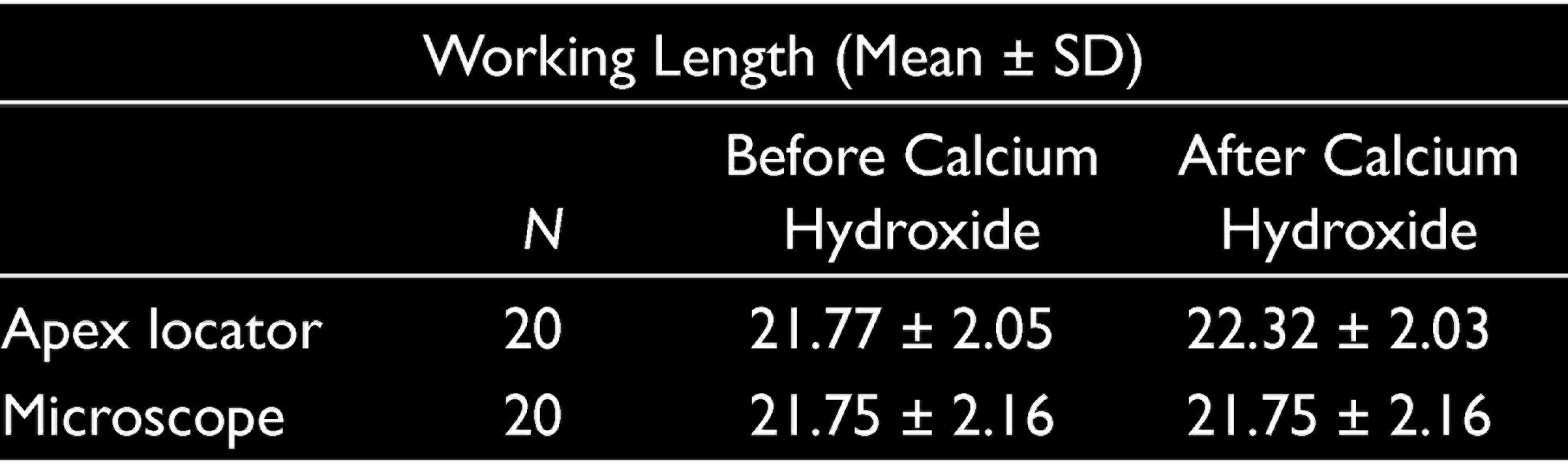
The statistical analysis of WL data showed a significant enhancement in WL after the application of calcium hydroxide (P < .05). Under these conditions, the accuracy of the apex locator was 45% in the distance range of 0 to ±0.5, implying that the difference between pre- and postmeasurements was less than 0.5 mm in 45% of the cases.
Under these conditions, the accuracy of the apex locator was 85% in the distance range of 0 to ±1. In other words, in 85% of the cases, the difference between the pre- and postmeasurements was less than 1 mm (Table 3). This means that calcium hydroxide reduced the accuracy of the apex locator.
Working Length (Mean ± SD) Before and After Calcium Hydroxide
Discussion
The WL is defined as the distance from a coronal reference point to the point at which canal preparation and filling should be terminated. 20 Previous studies clarified the usefulness and accuracy of Root ZX in determining root canal length. Commercially available modern EALs measure the impedance between the file tip and the root canal at different frequencies.21,22
One of the objectives of this study was to examine the effect of apical patency on the WL measurement by apex locator. Apical patency involves the repeated insertion or passing of a small handheld file through the apical foramen during canal preparation. 23 This study indicated that apical patency improved the accuracy of the apex locator in determining the WL. Tsesis et al. showed that apical patency had no significant effect on the determination of the WL. 24
Coronal preflaring is essential in endodontic treatment to eliminate cervical dentin interventions. Subsequently, it permits the file to easily reach the apical constriction and avoid changes in the WL. 11 Therefore, in the second phase of this study, the effect of coronal preflaring on the accuracy of WL determination by the apex locator was evaluated.
The results indicated that after preflaring of the root canal, the accuracy of the apex locator increased as compared to its value before preflaring of the root canal. This is in line with previous findings stating that this procedure can increase the accuracy of the Root ZX device.5,13
In agreement with the present result, Iqbal et al. reported an enhancement in the accuracy of the apex locator upon using coronal preflaring. 25 In contrast, Stabholz et al. (1995) stated that coronal preflaring has no significant effect on the accuracy of the apex locator. 11 Coronal preflaring reduced the file resistance, thus, facilitating the file insertion into the root canal toward the apex of the tooth. 26
Application of calcium hydroxide in the root canal is an approach to arrest inflammatory cervical resorption. 27 The study conducted by Tronstad et al. showed an increase in the dentin pH upon placing calcium hydroxide in the root canal. They deduced that the alkaline pH in the local environment of the resorption area may interfere with osteoclastic activity; it may also activate alkaline phosphatase, which plays an important role in hard tissue formation. 18 Ustun et al. examined the effect of calcium hydroxide residues on apex locator accuracy and indicated a decrease in the accuracy of apex locator with increasing calcium hydroxide residues. 17 Consequently, in another phase of this study, the influence of calcium hydroxide insertion on apex locator accuracy was assessed.
The results of the current study showed that the application of calcium hydroxide into the root canal decreased the accuracy of the apex locator in determining the WL of the teeth.
On the basis of the results of this study, it can be concluded that the apex locator exhibited better accuracy in determining the WL of the teeth after apical patency and coronal preflaring as compared with the cases before apical patency and coronal preflaring. On the other hand, calcium hydroxide residues in the root canal declined the accuracy of the apex locator in measuring the WL of the teeth. Therefore, it is recommended to completely remove calcium hydroxide from the canal prior to using the apex locator.
Footnotes
Acknowledgements
The authors would like to acknowledge the Kermanshah University of Medical Sciences for supporting this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was performed with funds from the Kermanshah University of Medical Sciences, Kermanshah, Iran (Grant No. 96662).
Ethic Approval
The protocol of the clinical trial was conduct-ed according to the ethical principles of Declaration of Helsinki (version 2002) and approved by the Ethics Committee of Kermanshah University of Medical Sciences (Code: KUMS.REC.1397.769).