
Abstract
Aim:
To compare the marginal adaptation of crowns fabricated by using three different resin-ceramic computer-aided design/computer-aided manufacturing (CAD/CAM) materials.
Materials and Methods:
Crowns fabricated from three different resin-ceramic CAD/CAM blocks, applied on a typodont premolar (#14), were tested with regard to marginal adaptation, in this in vitro study. The typodont maxillary first premolar was prepared to serve as the master die and digitized with an intraoral scanner. The same virtual crown design was used to fabricate all specimens. Forty-eight crowns were fabricated from the same virtual crown design using three different CAD/CAM resin-ceramic blocks as follows (n = 16): Lava Ultimate (LU), GC Cerasmart (GC), Vita Enamic (VE). Master die and crowns were scanned with a laboratory scanner and three-dimensional data were transferred into three-matic software. The software calculated the mean of the marginal discrepancy (MD) for each crown in negative and positive values, representing under and over estimation of the crown margin, respectively. A marginal discrepancy index (MDI) was obtained for each group using negative and positive MDs. All data were statistically analyzed using one-way analysis of variance and Tukey’s honest significance test (α = 0.05).
Results:
The analysis of variance showed no statistical differences between materials regarding the negative and positive MDs (P > .05). The MDI for LU was lower than GC and VE (P < .05).
Conclusion:
The marginal adaptation of different resin-ceramic materials was different with regard to MDI values. Nevertheless, the MD values of all groups were within the clinically acceptable range.
Introduction
Since the first appearance of computer-aided design/computer-aided manufacturing (CAD/CAM) in 1985, great improvements in this field have been achieved with advancements in technology.1,2 CAD/CAM systems were derived from the idea of preparing teeth and delivering restoration in the same clinical appointment, which is also regarded as chair-side dental treatment. Especially with the introduction of new CAD/CAM materials, the chair-side dentistry has become a highly demanded and implemented treatment option in daily dental practice. One of the newly introduced CAD/CAM materials of note is resin-based ceramic materials. Resin-ceramic CAD/CAM blocks can be manufactured by the following two techniques: filling a polymer network with nano-ceramic particles or infiltrating a preexisting ceramic network with resin polymers.3–5
Resin-ceramic CAD/CAM blocks are highly preferred in chair-side dentistry in association with their advantages. 3 These advantages include fast and easy production with no need for crystallization or glaze firing after manufacturing,3,6 ease of intraoral repair and polish,5,7 and better machinability because of their low modulus of elasticity.8,9 Additionally, the low hardness values of resin-ceramic materials are found to prevent the wear of opposing dentition, to enable rapid milling and to minimize marginal chipping which is associated with better marginal adaptation.3,7,9–12
The marginal adaptation is of great importance for the longevity of restorations. 13 Poor marginal adaptation was related to cement dissolution, plaque retention, microleakage, plaque accumulation, secondary caries, pulpal pathology, and periodontal disease.14,15 The marginal adaptation of a crown can be affected by the restoration material used.14,16 Manufacturers of new resin-ceramic CAD/CAM blocks have claimed that the improved machinability of these materials enables smoother and better-adapted margins after milling.3,9 However, restorations produced from different resin-ceramic CAD/CAM blocks may vary in terms of marginal adaptation because of the diversity in proportions of resin-ceramic ingredients and network design.
The main objective of the current study, therefore, was to compare the marginal adaptation of crowns fabricated by using different resin-ceramic CAD/CAM blocks with varying microstructure. The null hypothesis of this study was that there would be no difference among CAD/CAM crowns fabricated from different resin-ceramic blocks in terms of marginal adaptation.
Materials and Methods
Setting and Design
The first part of this in vitro study (preparing the study groups and digizing process) was conducted in the Research Laboratory of Ankara University, Faculty of Dentistry, and the second part of the study (data registration into three-matic software and marginal discrepancy [MD] evaluation) OMFS, IMPATH Research Group, Department of Imaging and Pathology, Faculty of Medicine, Leuven University in March to June 2019. This study included resin-based CAD/CAM blocks and three different commercially available CAD/CAM blocks with different contents of resin and ceramic were used for crown fabrication. A power analysis with 80% power and 95% confidence interval was performed based on the results of a pilot study and a sample size of 16 specimen per group was determined, accordingly. Possible reporting bias was prevented by blinding the researchers with group coding.
Master Die Preparation and Digitization
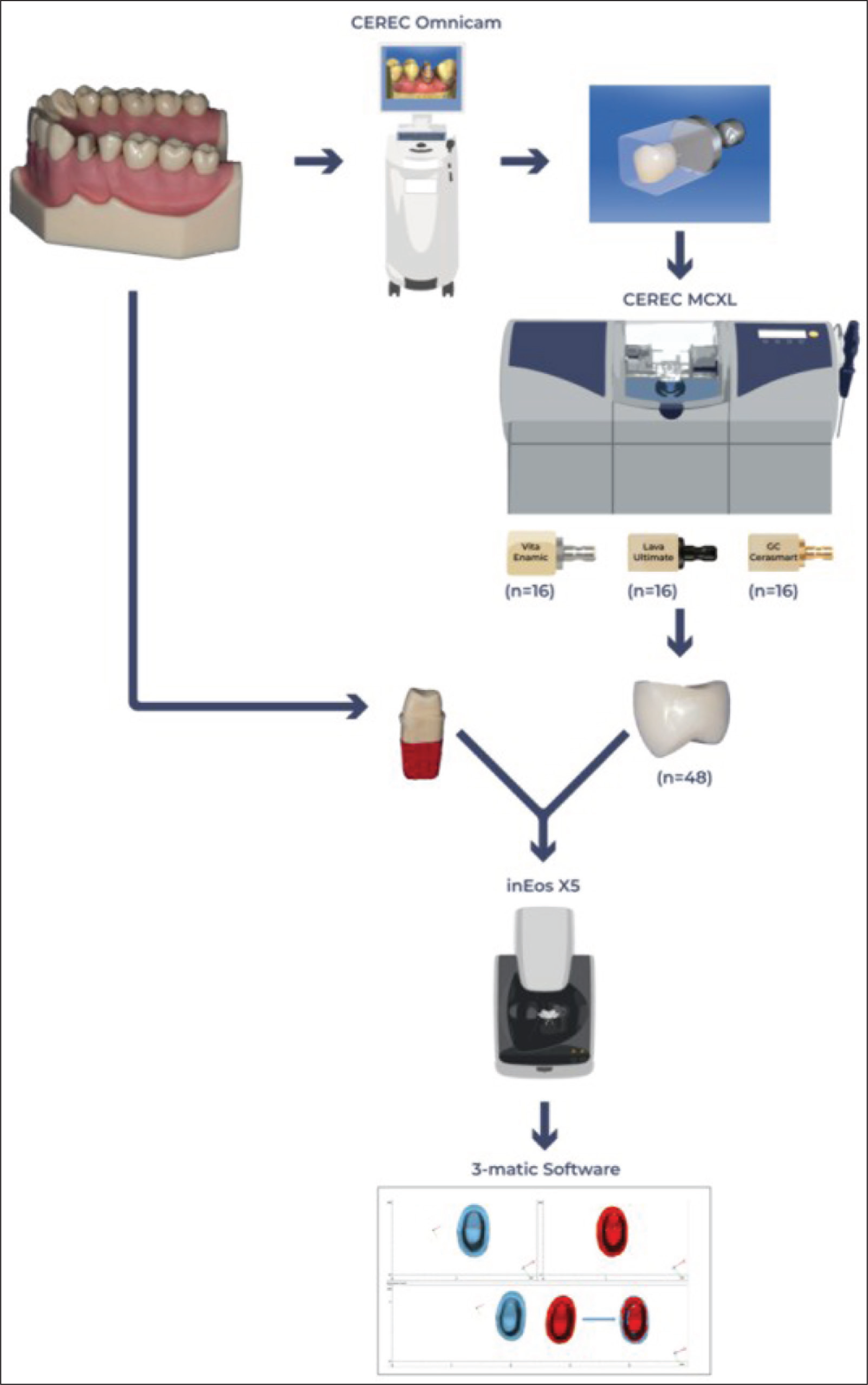
The schematic workflow of the present study was shown in Figure 1. A typodont maxillary first premolar placed on a model (Frasaco Dental Model, Frasaco, Tettnang, Germany) was prepared with tapering axial walls by 12 degrees, 4 mm crown height, and 1 mm circumferential supragingival shoulder finish line with rounded internal angles. The prepared master die was digitized by using an intraoral scanner (CEREC Omnicam, Dentsply Sirona, New York, USA). The “automatic margin finder” tool was used to draw preparation margin, and irregularities were corrected manually. The completed margin line was verified by two operators (E.İ.O and M.E.O). The die spacer parameter was set as 80 µm and a virtual crown was designed automatically by using the CEREC software (CEREC SW 4.6., Dentsply Sirona, New York, USA).
Schematic Workflow of the Study
Crown Fabrication and 3D Scanning
The same virtual crown design and clinical type milling unit (CEREC MC XL, Dentsply Sirona, New York, USA) were used to fabricate 48 identical crowns from three different resin-ceramic CAD/CAM blocks (n = 16): Lava Ultimate (LU, 3M ESPE, St. Paul, US), GC Cerasmart (GC, GC Dental Products, Tokyo, Japan), and Vita Enamic (VE, Vita Zahnfabrik, Bad Säckingen, Germany). Two 64-micron grit diamond burs (12 s step bur and 12 s pointed cylinder bur) of the milling chamber were changed with the new ones before the milling of each group. After the manufacturing process, the master die and the inner surfaces of all crowns were scanned with a laboratory scanner (inEos X5, Dentsply Sirona, New York, USA), outputting a standard tessellation language (STL) file for each scan. The STL files of different groups were coded with letters to blind the operators.
Superimposing the STL Images of Master Die and Crowns
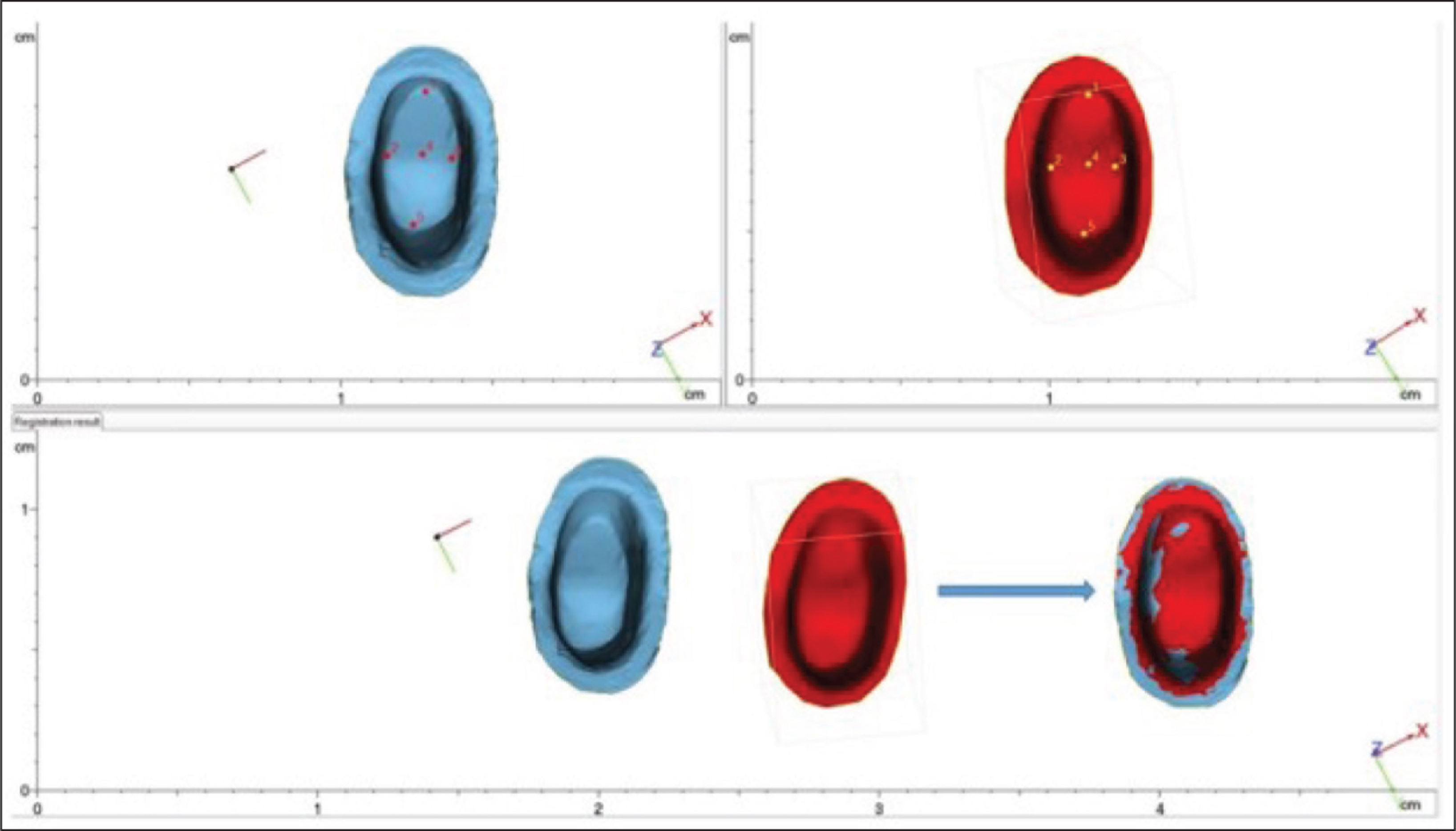
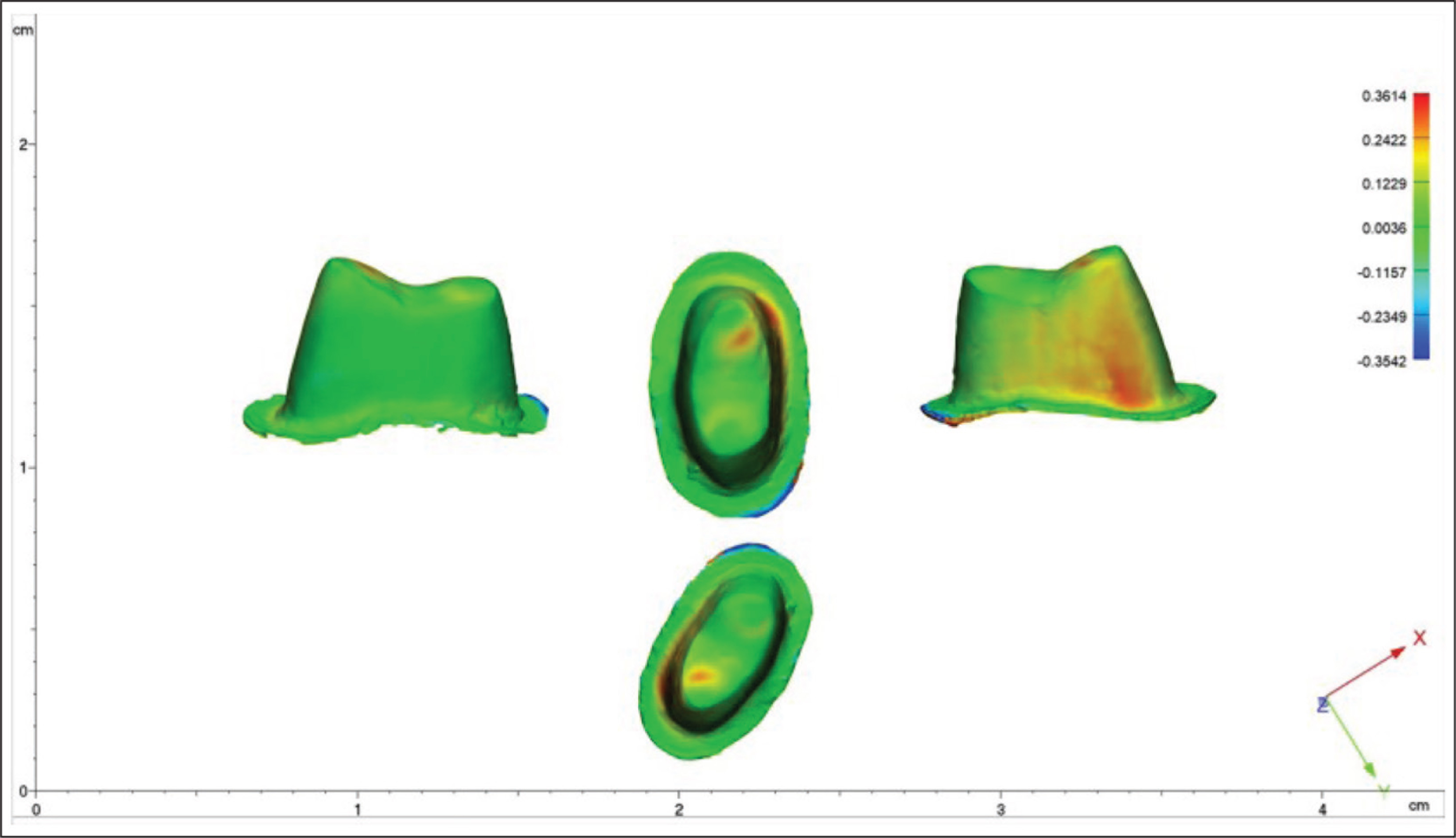
The generated STL files were imported into three-matic software (Version Medical 13, Materialise). The point-based registration was utilized by applying the predetermined corresponding reference points (n = 5) on both the master die and inner aspect of the crowns (Figure 2). This step allowed a close alignment of matched data in the same three-dimensional (3D) space. Following the point-based registration, a global registration was applied, which further refined the point registration. The global registration algorithm automatically assessed and assembled the vertexes of the master die and crowns, and fine-tuned the registration by providing the best fit of both geometries. The digital registration was verified by two operators (K.O. and S.S.). The software demonstrated a color map for each specimen that was superimposed with the master die. Color maps visualized the deviations in the ideal fit of the crown (Figure 3).
Representative Image of Reference Points (1–5) Used to Superimpose the Standard Tessellation Language Files of Master die (in Blue) and Crown (in Red)
Representative Image of a Color Map of Deviation Obtained After the Superimposition of a Crown on the Master Die
Positive, Negative Marginal Discrepancy (MD) and Marginal Discrepancy Index (MDI)
The three-matic program calculated the means of positive and negative MD values at every possible point for each sample. A positive value showed overestimation and a negative value showed underestimation of the crown margin. The MDI of each group was calculated by using the negative (- MD) and positive MD values (+MD) as MDI = - MD/+MD.
Statistical Analysis
The statistical program R v.3.5.3 (Microsoft Corporation, Washington, USA) was used to perform all analyzes (α = 0.05). The data were analyzed by using one-way analysis of variance and Tukey’s multiple comparison tests.
Results
The negative MDs, positive MDs, and MDIs are presented in Table 1. The lowest mean negative MD was obtained for LU (20.31 ± 36.62 µm) and the highest was obtained for GC (47.41 ± 50.24 µm). However, the difference among the test groups for negative MD was not statistically significant (f = 1.559, P = .222). The minimum standard error of the mean (SE) for the negative MD was obtained for LU (9.15) and maximum SE was obtained for GC (12.56).
The Mean and Standard Deviation (SD) Values of Negative Marginal Discrepancy (in µm), Positive Marginal Discrepancy (in µm), and Marginal Discrepancy Index

The LU group showed the lowest mean value for positive MD, although mean positive MDs in the three groups did not differ significantly (f = 0.870, P = .426). The LU group also showed the lowest SE of positive MD (19.64) and VE showed the highest (30.58).
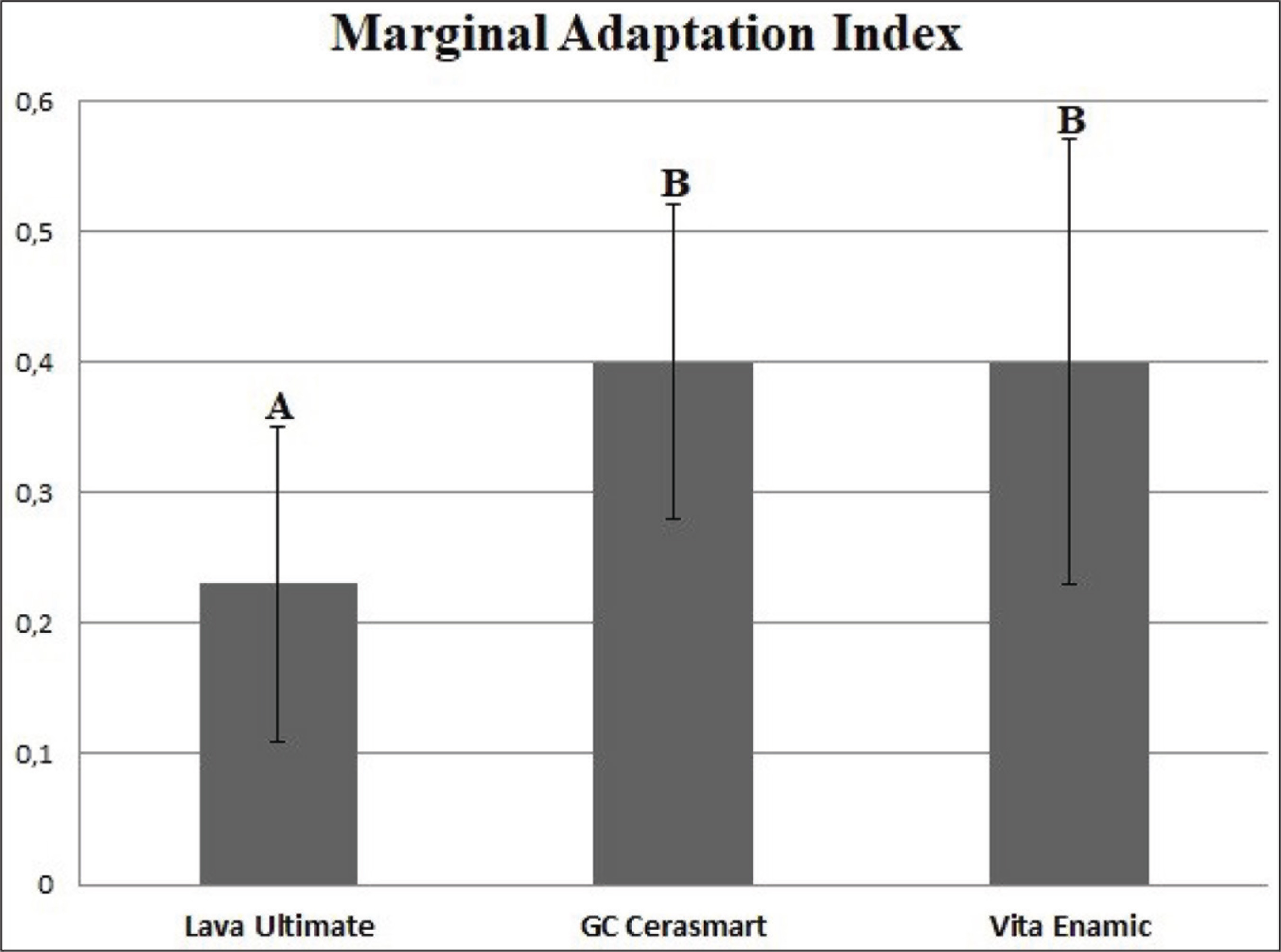
On the other hand, the one-way analysis of variance indicated significant differences among the MDIs (P = .001). The post-hoc Tukey’s test showed that MDI for LU was lower than that of the other groups (P < .05), whereas GC and VE were comparable (P = .45; Figure 4).
Comparison of Marginal Discrepancy Indexes Obtained for Each Group
Discussion
The marginal adaptation of a CAD/CAM crown may vary depending on the material type used to fabricate the restoration.13,17 This in vitro study aimed to compare the marginal adaptation of crowns fabricated by using different resin-ceramic CAD/CAM blocks. The mean MD values of all test groups were similar; however, the MDI for LU differed from other groups. Therefore, the null hypothesis should be partly rejected.
The study design utilized in the present study provided a standardized comparison of the marginal adaptation. As such, all crowns were produced using the same STL data and a precise CAD/CAM system was implemented to eliminate the manual errors, burs of milling chamber were changed in each group, and the MD measurements were performed using the same master die. Accordingly, it can be assumed that the consistency of results was ensured with standardized test conditions.
It is possible to measure the MD by several in vitro techniques such as the direct sectioning of the crown on a die, 18 measuring the images of the margin with a stereo-microscope, 19 and the silicone replica technique.12,20 Recently, with the advancements in the field of computer analysis systems, a new measurement method has been known to be available to science, 3D scanning and superimposing the STL files of the crown and die by reverse engineering software. 14 The present study implemented the 3D scanning and best fit alignment following the point-based registration method to measure the MD by three-matic program. Unlike the other 3D modeling software and in vitro methods that provide limited measurements, three-matic calculates the mean of every possible discrepancy measurement in negative and positive values. Therefore, a generalized MD measurement was enabled.
In the present study, the MD values of different resin-ceramic materials were similar. This finding can be supported by the results of previous studies carried out in the related field.4,12 However, Bankoglu et al. 21 found a higher MD value for GC than for LU and VE crowns. This study used the replica technique and a limited number of measurement locations to evaluate the marginal adaptation; therefore, it differs from the present study in terms of methodology and measurement technique applied.
In the present study, both negative and positive MD values of all groups were less than 120 μm, which is accepted by most of the authors as the maximum MD value.14,22,23 Therefore, the marginal adaptation of all resin-ceramic crowns can be considered as clinically acceptable. These results correspond with some researches,4,24 but are contrary to some other studies.12,13,21 The differences in these results can be attributed to the methodological differences considering that the MD values may vary depending on the production process, restoration type, measurement technique, and number of observations.21,25,26
The negative MD indicates the underestimation of the crown margin, whereas positive discrepancy indicates the overestimation of the crown margin. For an ideal marginal adaptation, both positive and negative values should be as close to zero as possible. In the present study, a new modality, called MDI, was employed to evaluate the characteristics of the marginal adaptation. A MDI greater than 1 indicates that the rate of underestimated crown margin is higher than the overestimated margin and an MDI lower than 1 indicates vice-versa. The MDIs recorded for all tested materials were lower than 1; however, it was significantly lower for LU than the other two resin-ceramic blocks tested. Different resin-ceramic materials exhibit variations in the proportions of resin and ceramic, resin matrix composition, size, and type of the filler particles.3,12 The Lava Ultimate is a resin nano-ceramic containing 80% by weight silica and zirconia clusters in a resin matrix. 27 GC Cerasmart is a hybrid nano-ceramic, composed of 71% by weight silica and barium glass nano-hybrid fillers and 29% by weight resin matrix. 28 Vita Enamic, also regarded as the polymer infiltrated ceramic network, consists of a porous ceramic network 86% by weight and an interpenetrating polymer network 14% by weight. 29 The differences in MDI may be a consequence of this diversity in the structural composition of resin-ceramics. The null hypothesis of the present study suggested no difference for the marginal adaptation of different resin-ceramic CAD/CAM crowns; however, MDI for LU differed significantly. Therefore, according to the results of the present study, it can be suggested that the resin and ceramic content of the CAD/CAM block used may alter the marginal adaptation of the crown fabricated.
Considering that the marginal adaptation of the restorations produced by using different scanners and milling units may vary,30,31 the use of a single scanner and milling device should be considered as a limitation of this research. Another limitation was that only three resin-ceramic CAD/CAM blocks were evaluated. An intraoral scanner was used to digitize the master die in in vitro conditions; however, the saliva, temperature, and individual variables relating to intraoral conditions may affect the digital impressions. Therefore, the present results should be interpreted cautiously.
Conclusion
Within the limitations of this in vitro study, the following conclusions were drawn:
Marginal adaptation of CAD/CAM crowns fabricated by using different resin-ceramic blocks was within the clinically acceptable range. The negative and positive MD values of LU, GC, and VE were similar. All-tested resin-ceramic groups had an MDI value below 1. The MDI value of LU was significantly lower than that of GC and VE.
Footnotes
Future Scope
The next step in research would be to include several CAD/CAM blocks, scanners, and milling units to assess the effect of different variables on marginal adaptation. The present study also indicates that in vivo research regarding marginal adaptation of the restorations is needed.
Acknowledgements
The authors thank Professor Dr Ensar Başpınar for his assistance as the statistical analyzer, Mr Şenol Deniz for the academic editing of the article, and Mr Çağlayan Güneş for the graphical images.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The equipment used in this research was supplied by Ankara University Scientific Research Projects Coordination Unit. Project Number: 14A0234001.