
Abstract
Aim:
To assess the knowledge, attitude, and practices of the patients regarding cross-infection in dental clinics in view of COVID-19, and its economic implications.
Materials and Methods:
The present study is a cross-sectional online survey done using Google Forms tool which was shared amongst 501 participants via e-mail and various social media platforms. It consisted of 42 structured questions regarding sociodemographics (seven questions), knowledge of COVID-19 (seven questions), practices regarding COVID-19 preventive methods (five questions), knowledge regarding cross-infection in dental clinics (nine questions), attitudes toward infection in dental clinics, and increased cost of treatment due to added disinfection protocols (14 questions). All the associations were tested using the chi-square test and with the P-value set at <.05. The significance level was taken as α = 0.05; therefore, a difference or association with P-value <.05 was considered statistically significant. The linear regression model was used to relate demographics with the knowledge attitude practices items, and Pearson’s correlation coefficient was used to evaluate the correlation between knowledge, attitudes, and practices.
Results:
A total of 478 responses were assessed. 92.2% of the respondents had high knowledge regarding COVID-19, and only 48.1% had a high knowledge score regarding infection control in dental clinics. The respondents exhibited high scores for practice related to COVID-19 (83.9%) and attitude toward infection control in dental clinics (91.9%). Using the Pearson’s correlation coefficient, knowledge attitude practices variables showed a significant correlation amongst each other (P < .001). Only 60% responded that extra infection control protocols will increase the treatment charges, and approximately 30% responded that they will not pay or were not sure of paying the extra charges. The proportion of respondents who were agreeing about paying the increase cost were independent of age (P = .226), gender (P = .328), education (P = .085), and profession (P = .121).
Conclusion:
A significant percentage of patients today have a lot of knowledge of COVID-19. Also, they have higher expectations than before from their dental health care providers regarding infection control.
Introduction
The 21st century has witnessed the emergence and reemergence of various highly contagious infections such as severe acute respiratory syndrome (SARS), middle east respiratory syndrome, H1N1 influenza, the Ebola, and currently the COVID-19 outbreak.1–4 Known to be caused by the SARS-COV-2, COVID-19 is the third human coronavirus epidemic after the SARS in 2002, and middle east respiratory syndrome in 2009. It has a much faster spread than the two other coronaviruses. 5 It may transmit through direct contact, i.e., inhalation of droplets produced during coughing or sneezing of an infected person and through indirect contact by touching the surfaces (and subsequently our oral, nasal or conjunctival mucosa) infected by droplets or body fluids from an infected person. 6
This pandemic brought all elective medical health care to a halt, especially the treatments which involve aerosol-generating procedures. The oral health care sector has emerged to be one of the worst-hit, as almost all dental procedures involve aerosol generation. 7 Dental procedures aerosolize saliva and may lead to airborne contamination as the oral cavity harbors bacteria and viruses from the nose, throat, and respiratory tract. 8 Even a simple noninvasive intra-oral examination implicates the risk of airborne infections owing to the proximity to the patient’s open mouth and breathing space. The present outbreak has forced dentists all over the world to defer all treatments except urgent care, not only leaving many patients in much discomfort but also the dentists in a financial crunch. There is a feeling of apprehension and fear in both the dentist and the patient regarding post-COVID-19 dental care. Preventive measures such as social distancing, hand hygiene, disinfection, and correct use of personal protective equipment (PPE) are crucial for preventing transmission in any health care setup. However, it will add to the treatment cost and time.
Dental treatment carries the risk of cross-infection from infection-causing pathogens between the patient and the oral health care provider. The generation of splatter and aerosols during dental procedures and proximity between patient and health worker pose a risk of airborne respiratory infections. 9 Similarly, handling of sharps and contact with the patient’s blood and saliva can transmit blood/saliva borne infections. Considering the risk of airborne transmission of SARS CoV-2 through aerosols, the risk of cross-infection through dental treatment is potentially high. Although studies have been conducted regarding cross-infection and infection control in dental clinics among dentists and dental students, 10 very few have evaluated this knowledge among the patients.11,12
Few recent studies have evaluated the knowledge, attitude, and practices of the population regarding the COVID-19 outbreak among Chinese and Iranian population.13,14 However, none have yet assessed the patient’s perspective regarding dental treatment in the view of COVID-19. The present study aims to get an insight into the patient’s viewpoint regarding the knowledge of CIVD-19 and its transmission, cross-infection in dental clinics, and the economic implications of the present outbreak on dental treatment.
Materials and Methods
Setting and Design
The period of study was from April 24, 2020, to May 3, 2020. The instrument for collecting data was Google form, which can be accessed at
The first section of the form was a declaration explaining the purpose and confidentiality of the survey. The participant’s choice to click the submit button at first page marked his or her consent to participate in the study. The study was designed to keep the anonymity of the respondents in mind, and no identification markers like name or e-mail address were required. Both convenience sampling (researchers themselves contacted respondents to participate in the study) and snowball sampling (the participating respondents were asked to forward the questionnaire to their contacts) were used to ensure maximum participation.
Questionnaire Method
The survey was shared amongst participants who were Indian nationals, via e-mail and various social media platforms such as Facebook and WhatsApp. The questionnaire consisted of 42 structured, closed-ended questions regarding sociodemographics, age/gender, educational background, nature of employment, medical status (seven questions); knowledge of COVID-19, its epidemiology and routes of transmission (seven questions); practices regarding COVID-19 preventive methods, like hand hygiene, social distancing, use of face masks (five questions); knowledge regarding cross-infection in dental clinics, aerosol, the spread of infection through saliva and blood (nine questions); attitudes toward infection in dental clinics, increased cost of treatment due to added disinfection protocols (14 questions).
The survey questionnaire was pilot tested (n = 25) to ensure practicability, validity, and interpretability of answers and was slightly modified based on the results of the pilot study.
The responses of the Google form survey were converted into an Excel sheet format for data analysis. The items of knowledge attitude practices (KAP) questionnaire were scored as 0 and 1 for incorrect and correct responses, respectively, in case of knowledge and practice items. In contrast, attitude items were scored as 0, 1, and 2 for the responses disagreed, neutral, and agreed, respectively. Scores obtained were recorded from 0% to 49.9% as low, 50% to 74.9% as moderate, ≥75% as high. Data were summarized as proportions and percentages (%).
Statistical Analysis
Statistical analyses were performed using SPSS version 19.0 (SPSS Inc., Chicago, IL, USA). All the associations were tested using the chi-square test and the P-value was set at <.05. The significance level was taken as α = 0.05; therefore, a difference or association with P-value <.05 was considered statistically significant. Linear regression model was used to relate demographics with the KAP items, and Pearson’s correlation coefficient was used to evaluate the correlation between the knowledge, attitudes, and practices.
Results
A total of 501 responses were collected. Forms that were incomplete or duplicates were excluded. Finally, a total of 478 forms were assessed with a response rate of 95.4%.
Demographics
In the study, the maximum respondents were of the age 18 to 30 years (55.1%), females were relatively more than males (55.5% vs. 44.5%), 41.7% were graduates, 34.3% were postgraduates, and 29.3% had academic qualification less than graduation. By profession, maximum were non-health care related (50.4%).
KAP Summary of Respondents (Table 1)
Knowledge Attitude Practices Summary of the Respondents
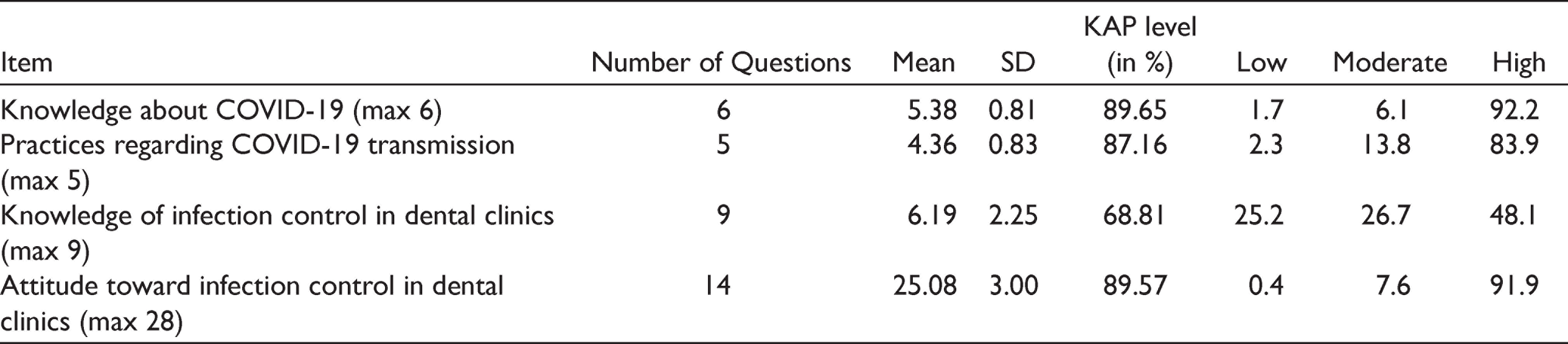
Although 92.2% of the respondents had a high knowledge regarding COVID-19, only 48.1% had a high knowledge score regarding infection control in dental clinics. The respondents exhibited high scores for practice related to the prevention of COVID-19 (83.9%), and attitude toward infection control in dental clinics (91.9%). Approximately 97% patients were familiar with the term COVID-19, and same percentages of patients were also aware of the symptoms associated with this disease. Similarly, they exhibited high knowledge about its mode of transmission and role of hand washing in preventing it. However, only 53% of the patients knew that the disease is caused by SARS-COV-2.
A good percentage of respondents (75%) were familiar with the term aerosol, and 71.3% of them knew that respiratory diseases like COVID-19 could be transmitted through aerosol. Likewise, they were highly knowledgeable about the importance of history taking and role of saliva in the transmission of disease. However, only 44% of the respondents were familiar with the term nosocomial infection and 50% could tell that autoclaving is the best method for sterilization.
A very high percentage of respondents replied that they wear mask and practice social distancing every time they step out of their homes (98.1%). However, only 65.7% of them replied that they would continue wearing masks after the outbreak was over. The patients were also highly aware of the disinfection protocols to be followed in the dental clinics in view of COVID-19 and had a high expectation from their oral health care providers regarding the same, although approximately 30% of the respondents said that they would not pay for the added cost for PPE or other disinfection protocols.
Association of Knowledge About COVID-19 and Infection Control With Demographic Characteristics (Table 2)
Association of Knowledge About COVID-19 With Demographic Characteristics
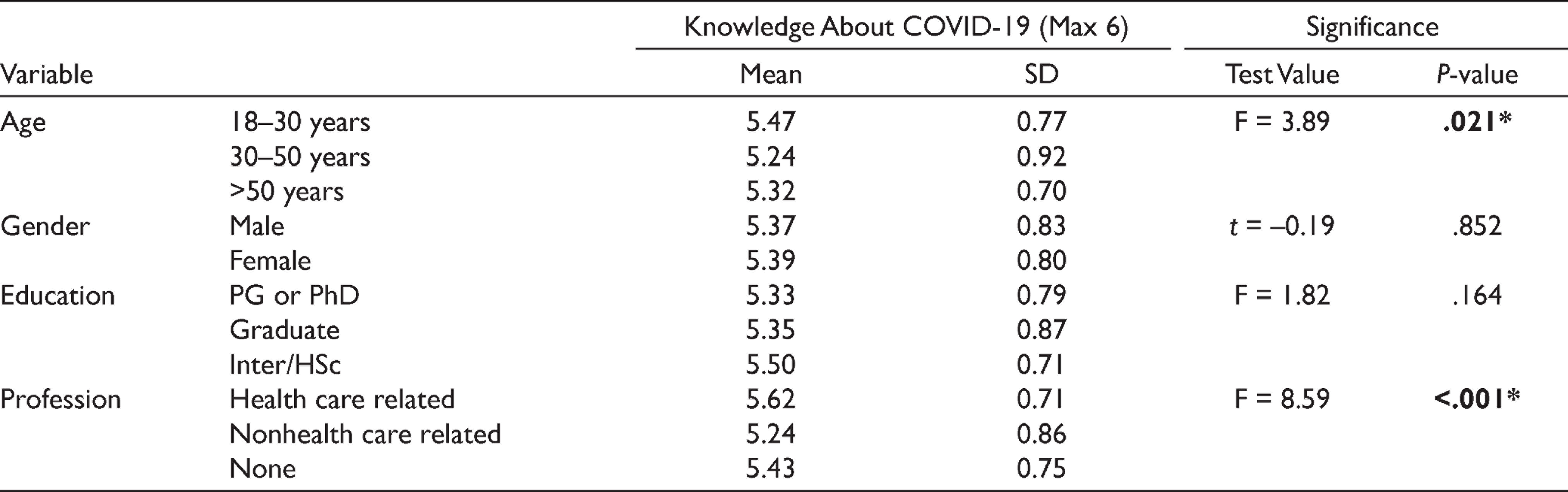
Age and profession showed a significant association with knowledge about COVID-19. A high knowledge score was seen among youngsters, while health care-related showed more knowledge score than non-health care related. Students, too, showed a high knowledge score.
Similarly, age, education, and profession showed a significant association with knowledge of infection control in dental clinics. A high knowledge score was seen among youngsters and elderly age groups compared to the middle age group. Graduates showed minimum practice scores while health care-related showed more practice scores than non-health care related and others.
Correlations Between Various KAP Aspects (Table 3)
Correlations Between Various Knowledge Attitudes Practices Aspects

The knowledge about COVID-19 showed a significant positive correlation with the knowledge of infection control (P < .001) and attitude toward infection control in dental clinics (P < .001). Further, practice regarding COVID-19 transmissions showed a significant positive correlation with the knowledge of infection control (P < .001) and attitude toward infection control in dental clinics (P < .001). The knowledge of infection control also showed a significant positive correlation with the attitude toward infection control in dental clinics (P < .001).
Multivariate Linear Regression of Association Between Demographic Characteristics With KAP Aspects (Tables 4 and 5)
Multivariate Linear Regression of Association Between Demographic Characteristics With Knowledge Attitudes Practices Aspects
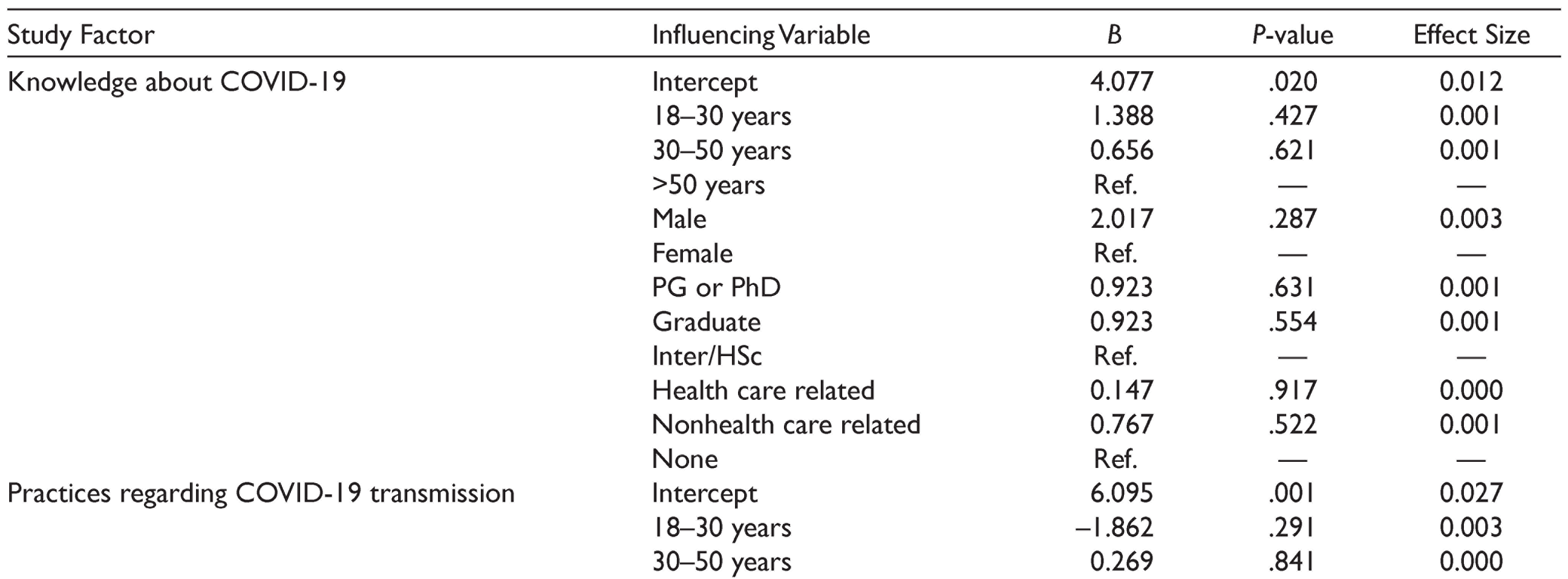
Model-Fitting Estimates of the Linear Regression Model
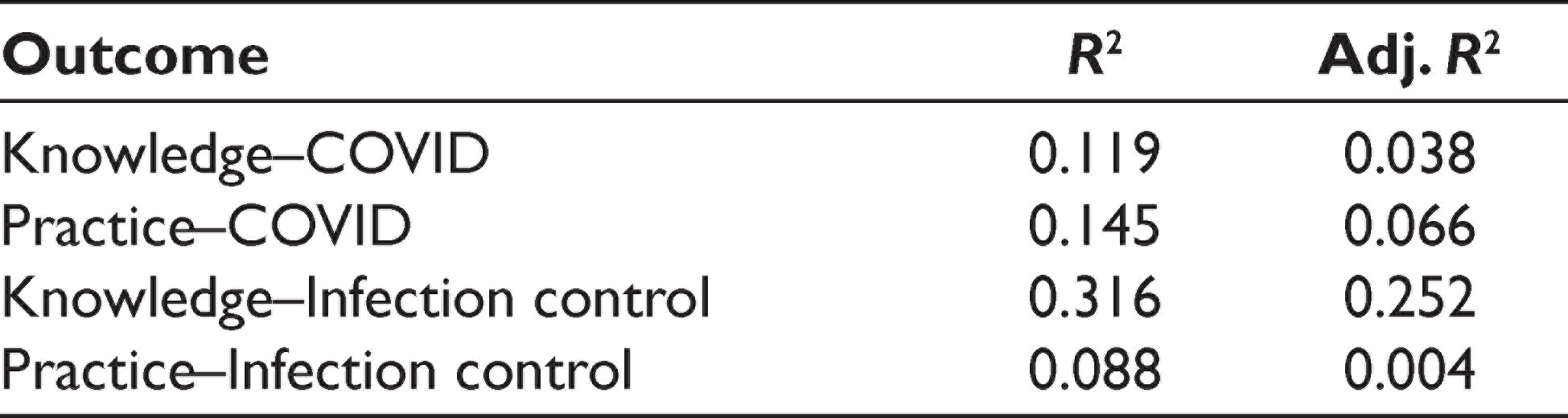
For the multivariate regression table, the following variables were taken as predictor and outcome variables:
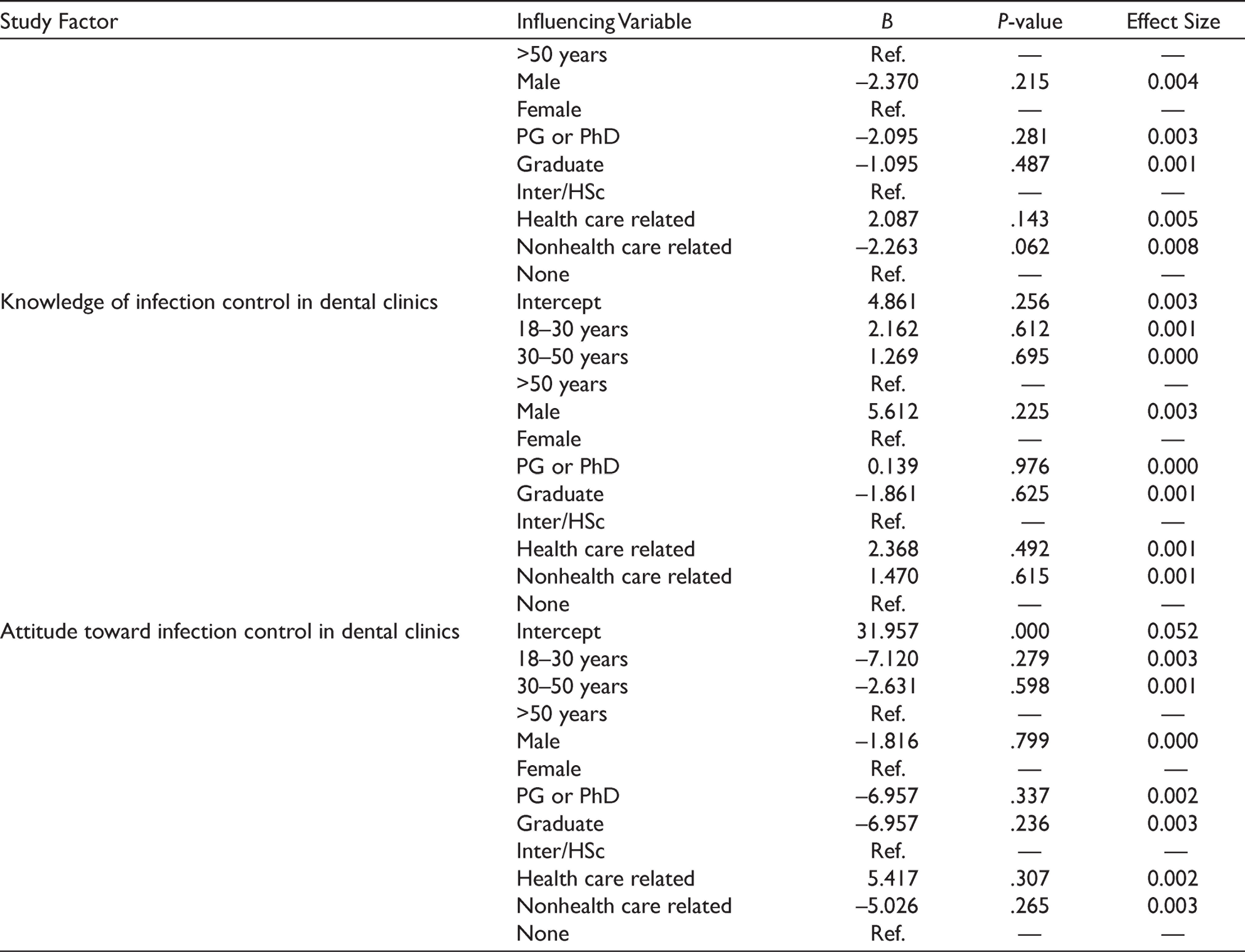
All the β-coefficients showed nonsignificance in the estimation of KAP parameters. This implies that none of the demographic variables is more important than others in estimating the knowledge, attitude, and practice levels of individuals. But estimators of effect sizes show that profession has more importance over other variables for estimating the study variable “Practices regarding COVID-19 transmission” (maximum effect size = 0.008).
The proportion of respondents who were agreeing about pay to increase cost were independent of age (P = .226), gender (P = .328), education (P = .085), and profession (P = .121).
Discussion
To our best knowledge, this is the first study to evaluate the knowledge, attitude, and practices of the population toward dental treatment in the view of COVID-19. The population was systemically healthy and well educated, with a majority of respondents being graduates. The study evaluated knowledge not only about COVID-19 but also infection about control in dental clinics and economic implications of COVID-19 on dental treatment.
The mean score of knowledge about COVID-19 was found to be 5.38 ± 0.81, which shows an overall 89.65% knowledge level, and a 92% high score level. A high level of knowledge can be explained by the fact that there is continuous and readily available information regarding COVID-19 on electronic and print media, various social platforms, and certain unique COVID-19 dedicated apps. Almost all respondents (97%) had heard the term “COVID-19,” and especially high-level knowledge was observed for questions such as diagnostic symptoms of COVID-19, routes of transmission of COVID-19, and role of hand washing in the prevention of COVID-19, though only 53% knew that SARS-CoV-2 causes COVID-19. The scoring percentage of knowledge regarding COVID-19 is comparable to a recent online survey among the Chinese population by Zhong et al., 13 where overall knowledge regarding COVID-19 was 90%. A similar high score of 90% was reported by Erfani et al. 14 among the Iranian population and in the range of 60% to 98.7% in a survey by Asaf et al., 15 among the Nepalese population.
The respondents showed high practice levels (87.16%) regarding COVID-19 transmission. Over 98% of the respondents responded that they wore a mask and practiced social distancing when they step out of their homes, and over 96% responded that they would continue to practice hand hygiene even when the outbreak is over. However, only 65.7% responded that they would continue wearing masks after the end of the outbreak. The recent guidelines by the center for disease control and the address to the nation by the prime minister upheld the importance of facemasks by the general public. Many states have made it mandatory to wear a facemask when stepping out of homes and in offices, even if it is made up of a three-layered cloth. However, a significant concern is proper disposal and maintenance (in the case of reusable cloth masks). Also, people find it uncomfortable to wear them throughout the day. This may be the reason they do not want to continue with this practice after lockdown is over. Hand hygiene is a straightforward, proven, and effective method of preventing transmission of infections. Regular reenforcement of this practice is made print/electronic media; social media and even the school-going children are now well versed in the seven steps of hand hygiene. Majority of the respondents in the present study were of a high educational and socioeconomic background; thus, information is readily available to them. However, studies have shown poor compliance with hand-hygiene practices in not so privileged populations. 16 In a study conducted by Agarwal et al. 17 in a slum area of India, a lack in hand-hygiene and sanitation practices was observed and only 42% of the study population reported using soap for washing hands after defecation. Only 48.1% of respondents scored high regarding infection control in dental clinics. These scores were much higher than a similar study by Ibrahim et al. 11 regarding patient’s knowledge of cross-infection in dental clinics, where only 21% of respondents had adequate knowledge. In another study by Elhoufery et al. 18 majorities of the study population had poor perception and low knowledge about reasons of hand washing (53%), the need of changing gloves (44%) between patients, or the use of masks (89%) by the dental health care providers. In the present study, a very high percentage of them knew that certain diseases could spread through blood and saliva (94.1%), and the importance of taking medical history before dental treatment. Interestingly, a decent percentage of them knew about aerosols (75%) and their role in transmitting respiratory diseases like COVID-19 (71%). Less than 50% of the respondents agreed that Hepatitis B or HIV could transmit through dental treatment. Although a dental patient must be aware of the risks of cross-infection in dental clinics as this understanding will make them more honest about sharing their medical history and more compliant with personal hygiene and self-care practices, this may also instill fear in them regarding acquiring infection from a dental clinic.
The respondents exhibited a very positive attitude toward infection control in dental clinics. A very high percentage of them agreed that the dentist should always wear masks and gloves while treating a patient (99.4%), changing gloves for every patient (97.4%), maintaining social distancing in the waiting area (96.4%), and providing hand sanitizers to them by the clinics (94.9%). 85% of them agreed that dentists should wear advanced PPE such as N-95 masks, impermeable gowns, and face shields while performing aerosol-generating procedures to protect themselves from COVID-19. A significant number of them (92%) expected their dentist and his/her assistant to wear a new PPE for every patient and 71% of them wanted their dentists to disinfect the operatory after each patient. Most of them (88.3%) agreed that PPE and disinfection protocols protect the patient too. Over 92% of patients responded that they would refuse treatment if the dentist is not wearing proper PPE, and 92% of them agreed that they would ask their dentist to wear a mask or glove if they are not wearing it. Previous studies of this nature have also shown that patients believe that dentists should always use gloves and masks while providing dental treatment and that they should not work on more than one patient with the same pair of gloves. 19
Approximately 60.3% of respondents agreed that the addition of PPE and disinfection protocols for COVID-19 would increase the procedures’ treatment cost. At the end of the questionnaire, the following question was asked: Would the patient agree to pay for the increased cost of treatment because of the compulsory donning of advanced PPE or other disinfection protocols? 12.2% of patients refused to this, 19.7% were of neutral opinion, and only 68.1% of them agreed to pay for the added cost. When asked for the reason to not pay for the added cost, only a few gave an explanation. Most of the respondents felt that PPE is a part of routine work protocol, and patients should not be burdened for it. Few respondents also stated that the government should provide PPE to the dentists or should subsidize it so that treatment expense is reduced. Also, some respondents mentioned that during the present crisis, the earning sources have diminished, and so it would not be possible for patients to bear this burden. Most of the respondents felt that dental treatment is already expensive and, therefore, the dentists should not charge extra.
Like many other professions, health care services have also faced a financial crunch since the time lockdowns were imposed to stop the spread of the SARS-CoV-2. Among the various medical services, the oral health care sector is particularly affected, as even simple oral examination cannot be conducted unless the clinician comes in close proximity to the patient. The PPE, such as N-95 masks and impervious double-layered gowns, are expensive and not affordable by many, because not only the doctors have to use them but also require to provide them to their dental assistants too. According to a recent survey conducted by the American Dental Association Health Policy Institute (HPI) across dentists in the USA, 76% of dentists surveyed had closed their offices to all but emergency patients during the COVID-19 pandemic (refer to
The present study was an attempt to assess the knowledge and perception of only a select population. Larger sample size with a wider geographical distribution would be more useful to come to a definite conclusion about the KAP of the population regarding COVID-19, and its implications in dental care. Although the survey was without any identification markers and respondents were assured of the results’ confidentiality, most of the questions were not related to one’s behavior; still, social desirability bias is a limitation of survey studies. Also, another limitation of a survey study is that it solely depends on the respondent’s compliance with answering the questions honestly.
Conclusion
The results of the present study suggest that dental patients in India today are highly aware of the present health crisis as well as of the measures that need to be taken to prevent disease transmission. Also, the patients have higher expectations than before from their dental health care providers regarding infection control, though a considerable percentage of them is not ready to bear the added cost.
Although infection control has always been a part of routine dental care, in the current scenario, it demands the use of advanced PPE, and rigorous disinfection and sanitization protocols. Thus, there is a need to look into, and cater for, both the exposure risk and monetary implications that the current COVID-19 outbreak has on the dental health care services.
Future Scope
Present times demand a tremendous change in infrastructure, logistics, and work-culture at a dental clinic. Both the dentists and their patients are vulnerable to acquiring transmitting airborne infections. As protection comes with an added cost, there is a need to look into, and cater for, both the exposure risk and monetary implications that the current COVID-19 outbreak has on the dental health care services.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.