
Abstract
Root resorption is largely pathologic and known to be initiated by several factors, including pulpal necrosis, trauma, periodontal treatment, orthodontic treatment, and bleaching agents. Incorrect diagnosis can lead to improper management and tooth loss. The treatment should involve the complete suppression of all the resorptive factors and the reconstruction of the defect using a suitable restorative material. The resorptive defect is often detected by the routine radiographic examination. A characteristic radiopaque line generally separates the image of the lesion from that of the root canal because the pulp remains protected by a thin layer of predentin until late in the process. Histopathologically, the lesions contain fibrovascular tissue with resorbing clastic cells adjacent to the dentin surface. Advanced lesions may also display fibro-osseous characteristics with deposition of ectopic bone-like calcifications. This case report presents extensive root resorption in the maxillary left lateral incisor and left canine in a 35-year-old patient. The defect was identified during the routine radiographic examination. The patient revealed a history of trauma 15 years back. Following the examination, the teeth were found to be vital and associated with the moderately deep periodontal pocket in the interdental region. The teeth were managed endodontically, and the resorption defect was restored with a biocompatible material after surgically elevating a flap. Periodontal management was also performed simultaneously by the surgical debridement of the area. Six-month postoperative radiograph revealed an arrest of the resorption and healing of the periodontal defect. Hence, an interdisciplinary management involving endodontic as well as periodontal treatment was performed that helped in saving the teeth with poor prognosis.
Introduction
Root resorption often occurs as a result of pulpal necrosis, dental trauma, periapical and periodontal infections, cysts, tumors, impacted teeth, and iatrogenic causes such as orthodontic treatment, endodontic treatment, replantation, and bleaching. It is a condition associated with either physiologic or a pathologic process, resulting in the loss of dentin, cementum, or bone. 1 The mechanism of resorption is clear, but the etiology is still not fully understood. The persistence of the ongoing inflammatory process is indeed a challenge in managing such cases.
The outer and inner walls of the dental root in a healthy tooth are protected by a thin antiresorption barrier. 1 The outer wall is protected by the precementum and the inner wall of root dentin is protected by the odontoblasts. Resorptive cells can, under no circumstances, colonize on the nonmineralized surface. 1 The premature mineralization of these protective barriers may be induced by multiple factors, thereby initiating the process of resorption.
The transformation of precursors into clastic cells is induced by cytokines of which the interleukin1 β plays a crucial role. 2 This can result in root and bone resorption and formation of granulation tissue, which harbors the inflammatory infiltrates, including polymorphonuclear leukocytes, lymphocytes, macrophages, and plasma cells. Multinucleated giant cells will resorb the tooth surface while the stimulus persists. The presence of either necrotic pulp rests or bacteria within the dentinal tubules attracts a large number of osteoclasts thus initiating the resorption process. 3
Root resorption types may be broadly classified into internal and external resorptions. The new version of the classification system separates dental-related root resorption from those that have medical-associated origins. 4 Furthermore, trauma-related root resorption, pressure root resorption, and idiopathic root resorption are further subdivided into etiologic and morphologic characteristics to assist clinicians in deciding the appropriate treatment options. 4
The use of dental-operating microscopes has enhanced the ability of clinicians to assess pathological changes more precisely and minimize the tissue damage. 5 Modern endodontic techniques such as optical aids and ultrasonic, thermoplastic obturation techniques have helped in achieving remarkable outcomes. Various bioceramic materials are being used to create a fluid-tight seal at the apical third, thereby assisting in healing. The resorption can be controlled by performing a proper endodontic treatment, which aims to remove all the pulp tissue to achieve a better seal. It is also necessary to use bioactive materials such as Biodentine to induce remineralization and healing. The use of bioactive materials such as mineral trioxide aggregate (MTA) and Biodentine induces remineralization and helps in healing, thereby playing a pivotal role in the rehabilitation of the resorbed teeth. 6
This case report describes the use of Biodentine for the treatment of external root resorptions along with endodontic and periodontal treatment of maxillary incisors with a history of trauma.
Case Report
A 35-year-old male patient was referred to the Department of Endodontics, Yenepoya Dental College, Mangalore, India. The patient was referred from a nearby dental clinic after being identified with a deep radiolucent defect in the maxillary left central and lateral incisors in the routine radiographic examination. The patient was asymptomatic with no history of pain or sensitivity. On detailed examination, he revealed a history of trauma 15 years ago and avulsion of upper front teeth. The patient was systemically healthy.
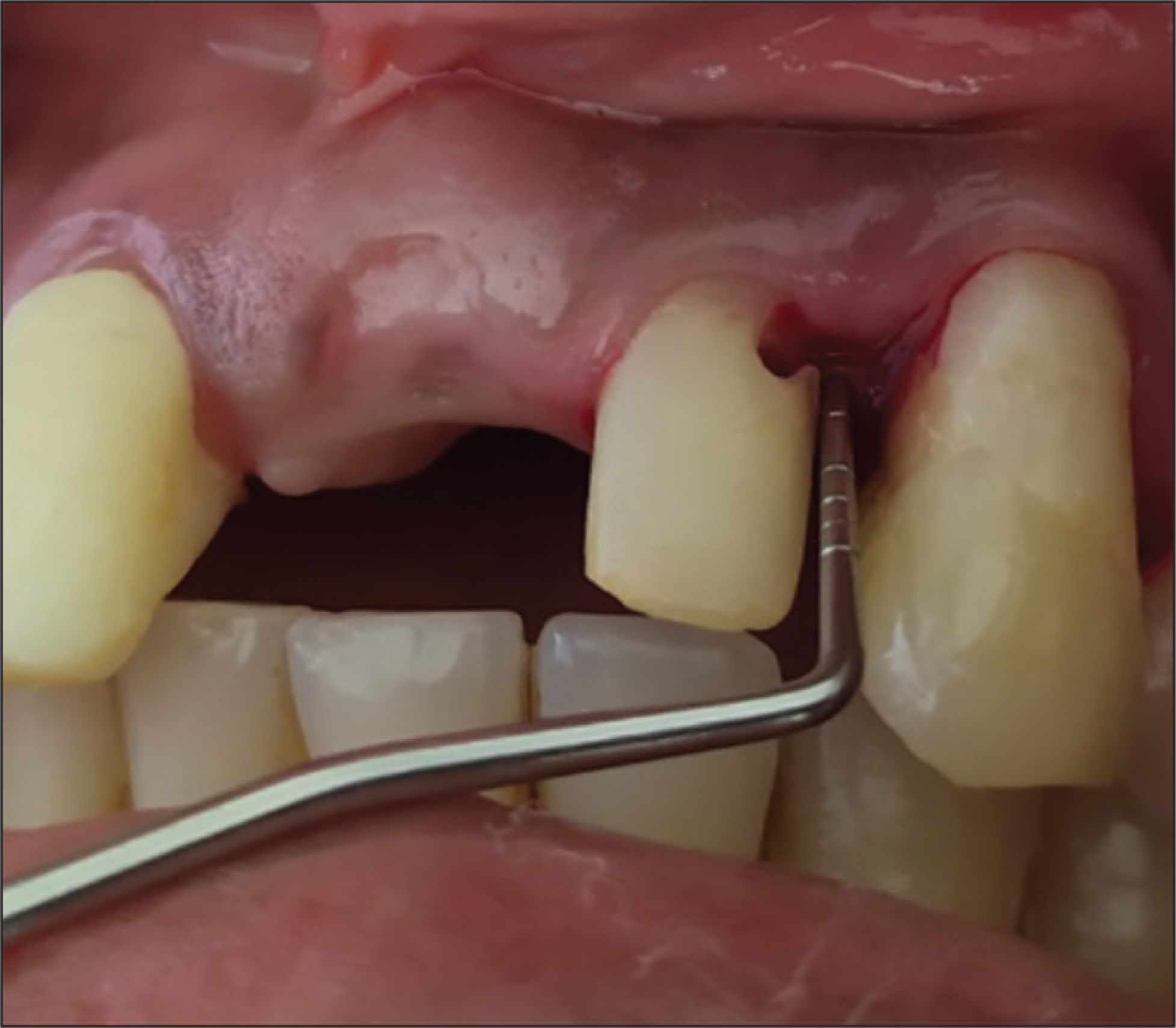
On clinical examination, the defects were identified in the upper-left quadrant’s incisor 22 and the canine 23, close to the cementoenamel junction, extending the apical to the gingival margin. These defects were covered by soft tissue. On exploring with a probe, ragged and irregular margins were found, and no soft or discolored dentin was detected. Hence, it was more suggestive of a resorptive defect than caries. The patient also had a missing central incisor 21 (Figure 1). A periodontal pocket of 5 mm was recorded mesial to 23 and distal to 22 using the Williams periodontal probe (Hu-Friedy, Chicago, IL, USA). The pulp vitality test using an electric pulp tester (Parkell Inc., Edgewood, NY, USA) gave an early response (Figure 2).
Preoperative Photograph which Shows the Small Resorptive Defect in the Upper Lateral Incisor

Periodontal Pocket of 5 mm Distal to 21
On radiographic examination, no periapical radiolucency was detected. A second radiograph was taken in different angulation to confirm whether the defect was communicating to the pulp. The resorptive defects were clearly visible in the intra-oral periapical radiograph with a substantial amount of tooth substance loss. Deep resorptive defects were found in both mesial to canine and distal to lateral incisor, almost approaching the pulp. A crestal bone loss was identified between 22 and 23. The bone loss was horizontal in nature. Periodontal ligament space widening was also detected in relation to the teeth (Figure 3).
As the defect was clinically accessible and clearly visible in the radiograph, it was not prudent to unnecessarily subject the patient to cone beam computed tomography (CBCT) considering the additional expense to the patient. Moreover, a CBCT should be used only when the patient’s history and clinical examination demonstrate that the benefits to the patient outweigh the potential risks.
Considering the clinical and radiographic examination, a provisional diagnosis of external root resorption was confirmed. Treatment was planned in such a manner that the tooth was managed both endodontically and periodontally along with the restoration of the defect with a biocompatible material.
Preoperative Radiograph

Treatment
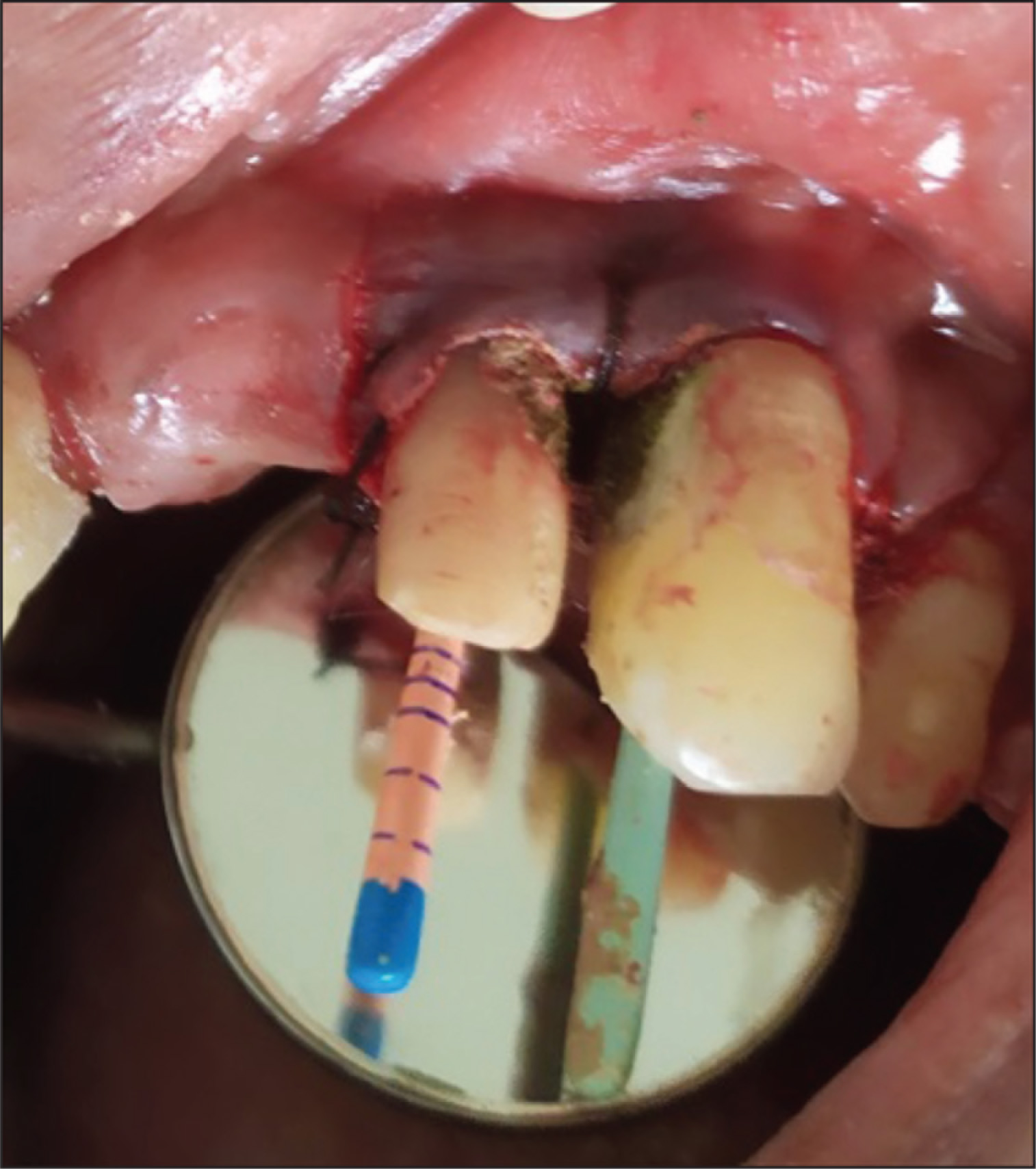
Before starting the treatment, the patient was explained about the various procedures to be performed, and an informed consent was taken from the patient. The area was anesthetized by the nasopalatine nerve block and infiltration with lignocaine hydrochloride and adrenaline 1:80,000 (Lignox 2%A, INDOCO Remedies, Bengaluru, India). After anesthetizing the area, a crevicular incision was made that extended from the mesial of 22 to distal of 23 using BP blade#15 C (Swann Morton, Sheffield, England). Two vertical releasing incisions were placed. A mucoperiosteal buccal flap was elevated using Glickman’s periosteal elevator (Hu-Friedy, Chicago, IL). The defect was visualized and was found to be occupied by granulation tissue. A thorough debridement of the defect was done with the removal of granulation tissue using Gracey Curettes (Hu-Friedy 5,6; curettes specified for interproximal areas of anteriors and premolars). There was tooth structure loss, leading to a defect of 4 mm × 2.5 mm on the distal surface of 22 and 5 mm × 3 mm defect on the mesial surface of 23 with communication to the pulpal space in both the teeth. A thorough root planing was done to remove the residual embedded calculus and altered cementum (Figure 4).
As the resorption defect was extending subgingivally, the presence of an edentulous space in relation to 21 made it difficult to use a rubber dam for isolation. Hence, cotton roll isolation with high vacuum suction was used. In the same visit, access opening was done using an endo access bur (Dentsply Sirona, Bengaluru, India) followed by shaping withprotapernext (Dentsply Sirona, Bengaluru). Using the crown-down technique, the quadrant’s incisor 22 was enlarged to X2 and the canine tooth 23 was enlarged to X3 files. Considering the communication of the pulp space with the defect 1% NaOCl was used as an irrigant followed by normal saline (Figures 5 and 6). Obturation was completed using the 6% Gutta Percha and Sealapex sealer (Kerr Corporation, Brea, CA, USA) by warm vertical compaction. The unsupported tooth margins were removed using an ultrasonic tip (Start X tips#1; Dentsply Sirona, Bengaluru). The resorption defect was dried thoroughly after the bleeding stopped and restored with Biodentine. The material was allowed to set. Flaps were approximated and sutured with the braided black silk 3–0 using simple interrupted sutures. The patient was recalled after a week for suture removal. It was found that the coronal part of Biodentine restoration was discolored and under contoured. Hence, a top-up restoration with glass ionomer cement (GIC, Type IX) was placed. After a month, temporary prostheses were given. The patient was recalled after six months for review and permanent prosthesis. Clinical and radiographic examinations revealed reduction in the pocket depth, along with bone fill and intact restorative material. No new resorptive defect was detected (Figure 7 and 8).
Resorption Defects on the Distal Surface of 22 and 23 Mesial Surface

Placement of Biodentine and Endodontic Treatment
Top-up Restoration with GIC

Six-Month Postoperative Radiograph

Two-Year Postoperative Picture with the Prostheses and Restored 23

Discussion
Root resorption occurs when natural protection of predentin and odontoblasts in the root canal is damaged. Multinucleated giant cells initiate and activate the resorption process at the internal aspect of the root canal. 7
The problem detection at the beginning of this development, the exact removal of the resorption tissue, endodontic treatment when indicated, and the restoration of the defects with an adequate isolation of the operating field determine the prognosis of the affected tooth. 8
The treatment of external cervical resorption involves the removal of all granulation tissue from the resorptive defect followed by restoration with a biocompatible material.
Laux et al. 9 conducted a study that associated the clinical finding of root resorption with the histological examination. Biodentine has been promoted as a favorable repair material due to its bioactivity and biocompatibility. Biodentine has a setting time of less than 12 minutes and high mechanical properties with excellent sealing ability. Its property to release calcium ion and enhance the alkaline environment makes Biodentine more conducive for osteoblastic action.
Takumi et al. 10 recently reported that multiple root resorption could be a new manifestation of systemic sclerosis. Kqiku et al. 11 treated two cases of invasive cervical resorption with the sandwich technique using MTA which showed favorable clinical outcome. The present case was hence managed appropriately using Biodentine as the root repair material for the resorption defect and the periodontal defect managed by open flap debridement. Since the periodontal defect showed horizontal bone loss, osseous grafts were not placed. The patient was under observation for a month after which the prostheses was fabricated. 6 Months postoperatively, the patient was reviewed again, and oral hygiene instructions were reinforced.
Lima et al. 12 managed similar defects using thermoplasticized gutta-percha. Since the defects were noncommunicating, stable results were observed. Mehra et al. 6 reported three cases of root resorption, which were diagnosed using CBCT and successfully managed using three techniques, thermoplasticized gutta-percha, MTA, and Biodentine. Eftekhar et al. 13 also reported a case in which the mandibular canine with invasive cervical resorption was managed successfully using Biodentine. Dastpak et al. 14 reported a case where permanent immature tooth with external root resorption was successfully managed by revascularization treatment. The tooth was treated by the protocol suggested by the American Association of Endodontics (AAE), consisting of disinfecting the root canal system, filling it with blood clot and sealing the root canal with MTA followed by bonded resin restoration. The symptoms disappeared and size of the periapical lesion reduced at 12 months follow up.
To improve the predictability of the results, advanced radiographic aids such as CBCT could have been used which would have given a three-dimensional image of the lesion and the treatment done, but according to the AAE and American Academy of Oral and Maxillofacial Radiology joint position statement, CBCT should be used only when the patient’s history and a clinical examination demonstrate that the benefits to the patient outweigh the potential risks and should not be used routinely for endodontic diagnosis or for screening purposes in the absence of clinical signs and symptoms. 15
Conclusion
In order to stop the resorption process, an early diagnosis and treatment is crucial. The commencement of endodontic treatment at the earliest is imperative to arrest the progression of the resorptive process to prevent further weakening of tooth structure. Success in management of a case of external resorption attributed to the history of trauma depends on early detection, appropriate treatment planning, removal of inflammatory pulp tissue, reinforcement of weaker tooth structure, and a three-dimensional obturation. The choice of restorative material also plays an important role. Biodentine has proved to be a favorable restorative material due to its high mechanical properties and excellent sealing ability.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.