
Abstract
Aim:
To determine the prevalence of orofacial mesenchymal neoplasms and classify them using the WHO criteria while appraising its applicability.
Materials and Methods:
This was a retrospective study involving a total sample of 192 entries diagnosed as mesenchymal tumors for the period 1990-2018 at the Oral Pathology Department, University College Hospital, Ibadan. The histopathology records were examined and clinicopathological data were obtained. Hematoxylin and Eosin slides of the cases were assessed to confirm the diagnosis. Tumors were classified using the WHO 2013 classification. Data were analyzed and presented using descriptive statistics.
Results:
Orofacial mesenchymal tumors constituted 7.9% of 2402 biopsies. There were 26 diagnoses in 161 tumors of the WHO classification. Male-to-female ratio was 1.1:1. Peak age group was in the third decade. Soft tissue tumors were 61.5%, while bone tumors were 38.5%. Benign tumors constituted 49.5%, while sarcomas and intermediate tumors were 45.8% and 4.7%, respectively. The mandibular region (29.7%) was the most commonly affected site. Adipocytic and osteogenic tumors were the most prevalent tumors in the soft tissue and osteoarticular series, respectively, representing 19.8% and 32.3% of all cases, while orofacial sarcomas constituted 3.6% of all lesions seen.
Conclusion:
The findings in this study are in line with those of previous studies. However, the WHO classification may not be suited for the orofacial region. Crafting of a classification system for mesenchymal tumors of the orofacial region would thus be necessary.
Introduction
The mesoderm gives rise to the connective tissue which forms the supporting structure of the body. From the mesoderm, benign and malignant soft tissue and osteoarticular tumors arise.1–3 These largely include soft tissue tumors (STTs) of tissues like adipose tissue, muscle, neural tissue, fibrous tissue, blood vessels, as well as those of bone or cartilage. The etiology of STTs is unknown but is postulated to arise from pluripotent mesenchymal stem cells following genetic mutations. Various factors, including the following, have been linked with sarcomas: radiation, chemicals, familial cancer syndromes, immunosuppression, and viral infections. 4 Overall, STTs have a large preponderance of benign lesions over malignancies. 5 Also, amongst the malignant group, 80% arise from soft tissues, while osteoarticular sarcomas constitute the remainder. 6
By and large, soft tissue sarcomas (STSs) are rare and heterogeneous with over 100 subtypes. 7 They are characterized by aggressive behavior as well as a tendency for distant spread, which is typically present as an enlarging soft tissue mass in the affected site. 8 The limbs are most commonly affected, 9 while the trunk and the head and neck region are less commonly affected. 8 Despite the rarity of STSs, they constitute about 1% of all malignancies8,10 and, like most malignancies, constitute a high burden on health care because of the aggressive treatment required. 8
Although all ages are affected, STSs have a tri-modal age distribution (depending on the histologic type) with peaks in less than 10 years of age, between 11 and 40 years, and over 40 years age groups. 8 Nonetheless, head and neck STTs are relatively uncommon among STTs generally, but head and neck STSs constitute 5% to 15% of all sarcomas.4,11 Also, depending on the review series, variations exist in the clinicopathologic parameters. However, a slight male preponderance has been reported. 12 Likewise, symptoms are dependent on the site affected. 8 Most commonly described symptoms for sarcomas in the head and neck region include a painless mass, while bone sarcomas are frequently associated with pain. 13 Visual disturbance, epistaxis, chronic sinusitis, otalgia, sensory, and/or motor disturbances are other presenting symptoms. 14
Generally, definitive diagnosis of STTs is by histological examination and precise histopathological diagnosis is essential for appropriate therapy. 15 Nonetheless, immunohistochemistry has considerably aided histological interpretation, 16 but most STTs lack specific immunohistochemical markers. 15 In addition, special stains, electron microscopy, and cytogenetic/molecular methods have greatly increased diagnostic accuracy. 17
Principally, histology is used for classification of STTs, based mainly on tumor histogenesis and biological behavior. 7 The WHO classification is recommended and widely used primarily for the trunk and extremities. In addition, it offers a suitable basis for typifying STTs of the orofacial region.
However, this classification has not been applied much in the orofacial region. Thus, the aim of this study is to determine the prevalence of mesenchymal neoplasms of the orofacial region diagnosed in the Oral Pathology Department of the University College Hospital, Ibadan. Also, the objective is to classify them using the WHO 2013 classification of soft tissue and bone tumors while appraising the applicability of the WHO 2013 classification to the orofacial region.
Materials and Methods
Setting and Design
This retrospective study was performed at the Oral Pathology Department of the University College Hospital, Ibadan. The reports of all biopsies submitted at the Oral Pathology laboratory for the period 1990 to 2018 were reviewed from June 2019 to August 2019. Ethical approval for this study was obtained from the University of Ibadan/University College Hospital Ibadan Research Ethics Committee, Ibadan, Nigeria (UI/EC/19/0267).
Sampling Criteria
The histopathology records were examined and all entries with primary diagnosis of a neoplasm involving soft tissue and/or bone of mesenchymal origin, according to the WHO classification of tumors of soft tissue and bone, 7 were identified. The inclusion criteria were cases whose records had complete information, while those with inadequate information were excluded from the study.
Study Method
A data collection form was used to obtain information such as age, gender, site of lesion, and histopathological diagnosis from the histopathology reports. Furthermore, the hematoxylin and eosin stained histopathological slides of the selected cases were retrieved and examined by two of the authors (Akindayo Olufunto Akinyamoju and Bukola Folasade Adeyemi) to verify the diagnosis as stated in the histopathology records.
Statistical Analysis
All data were analyzed using the Statistical Package for Social Sciences (SPSS) software version 20 (IBM Corporation, Armonk, NY, USA). The data were presented using summary statistics such as frequency tables, charts, rates, means, and standard deviation.
Results
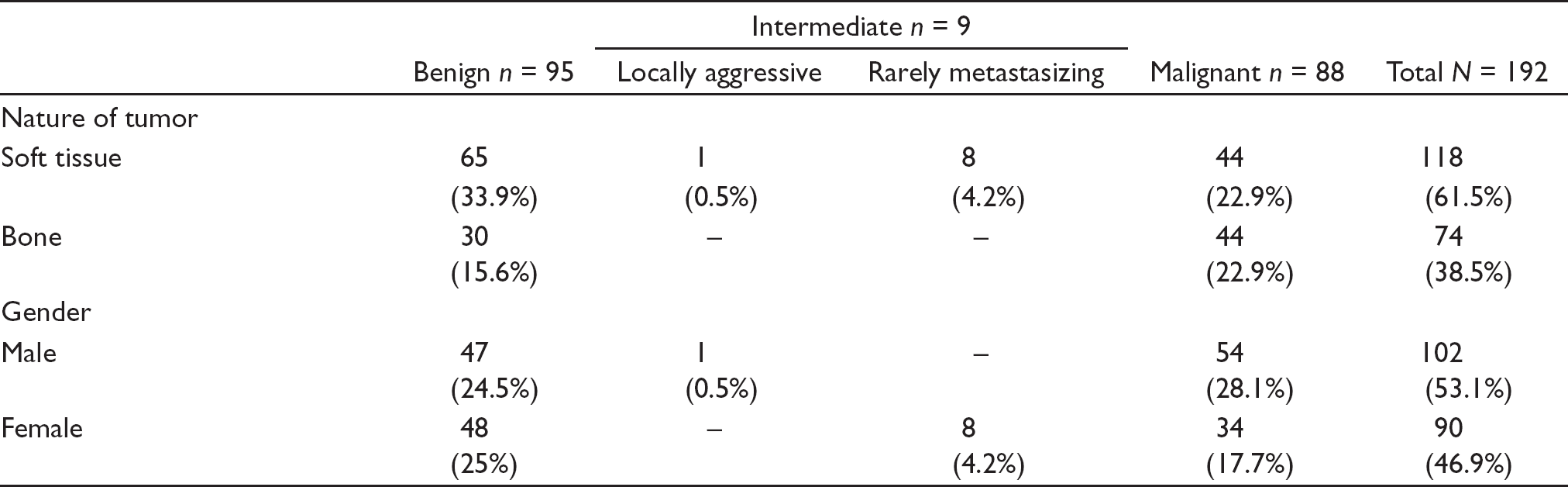
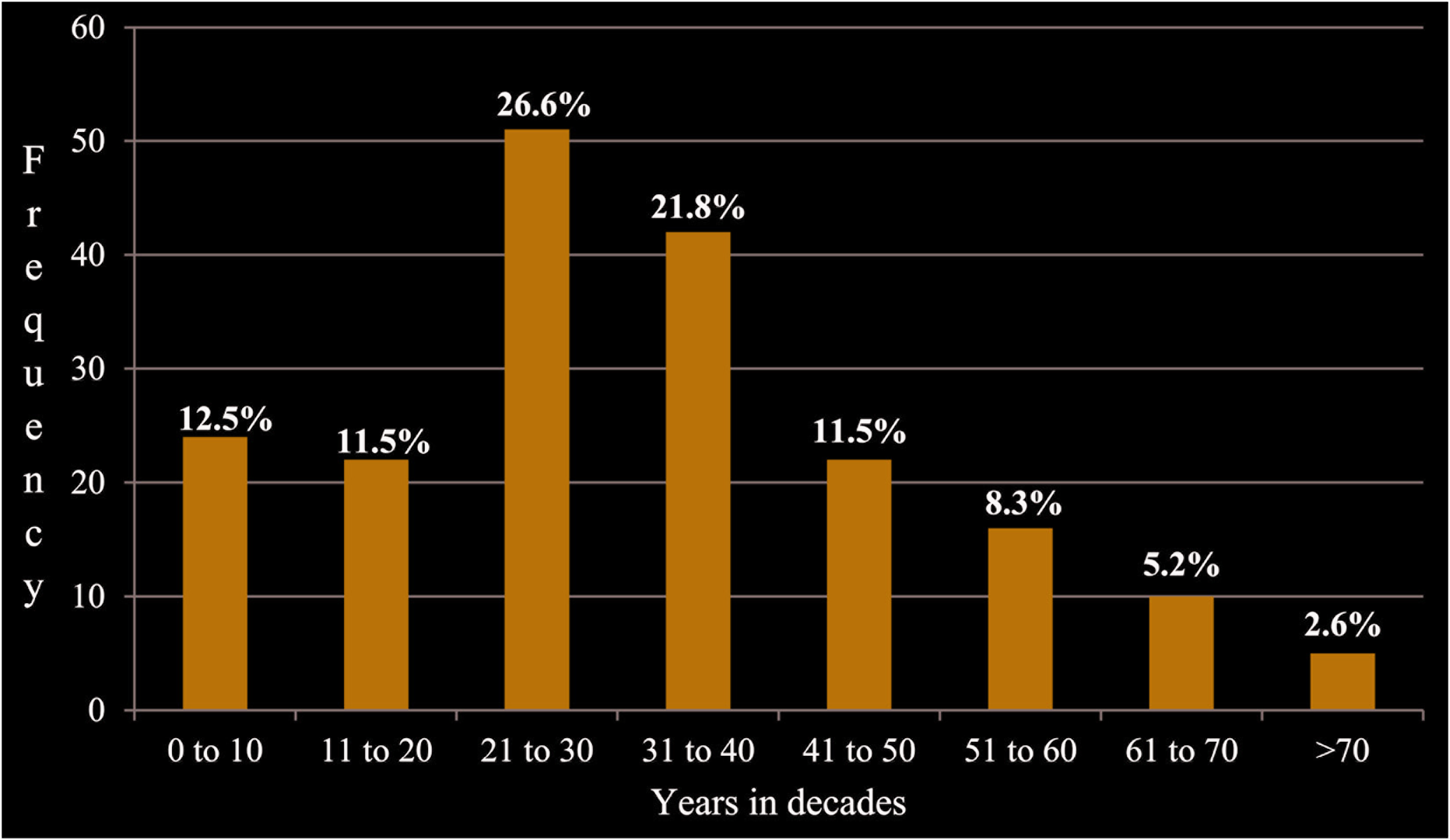
Within the period of study, 192 orofacial tumors were diagnosed as soft tissue and bone tumors of mesenchymal origin, constituting 7.9% of 2402 biopsies. There were 26 histological diagnoses in 32 groups of orofacial mesenchymal tumors in a total of 161 tumors present in 52 groups of neoplasms in the WHO 2013 classification of soft tissue and bone tumors. There was a slight male preponderance with a ratio of 1.1:1 (Table 1). The peak age group at presentation was in the third decade with 51(26.6%) cases, followed by the fourth decade with 42(21.9%) cases. Also, the first decade recorded 22 cases, representing 12.5% (Figure 1). The mean age of patients in this study was 31.9±18.5 years. However, the mean age of men was 29.6±18.1 years, while for women it was 34.8±18.7 years. There was no statistically significant difference between these mean ages (t = –1.976, degree of freedom = 190, P = .05).
Clinicopathologic Features of Orofacial Mesenchymal Tumors
Age Group Distribution of Orofacial Mesenchymal Tumors
In addition, there were more STTs, representing 118 (61.5%) cases, while bone tumors constituted 74 (38.5%) cases (Table 1). The tumors were distributed according to type as benign, intermediate (locally aggressive and rarely metastasizing subtypes), and malignant. Overall, benign tumors constituted 95(49.5%) cases, while sarcomas and intermediate tumors constituted 88(45.8%) and 9(4.7%) cases, respectively. Benign STTs were the most prevalent in the distribution constituting 65(33.9%) cases, followed by sarcomas of soft tissue and bone each constituting 44(22.9%) cases (Table 1).
Furthermore, sarcomas constituted 3.6% of all reports and 14.4% of orofacial malignancies over the study period. The age range for orofacial sarcoma was 77 years, with a minimum age of 3 years and a maximum of 80 years. The peak age of presentation of orofacial sarcomas were in the third decade of life with 25(28.4%) cases, followed by the fourth decade with 21(23.9%) cases.
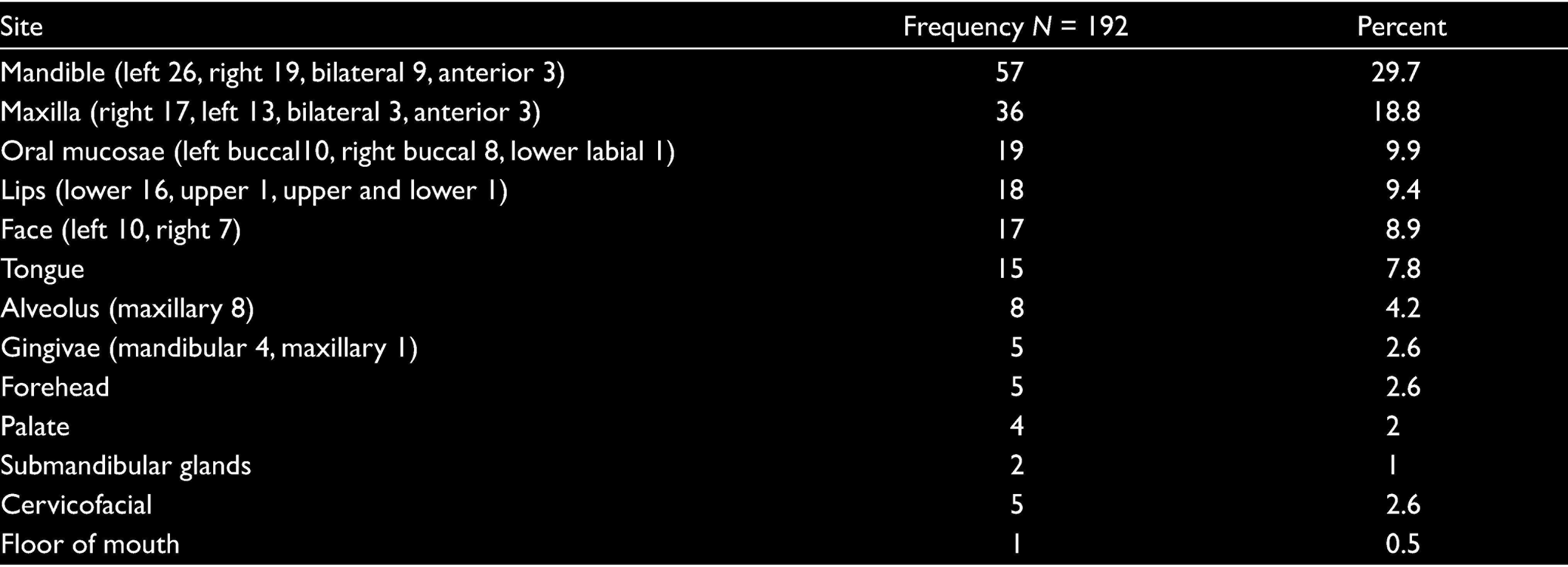
The mean age of presentation of benign mesenchymal tumors was 34.7±20.4 years, which was higher than 28.9±14.9 years recorded for sarcomas. Also, the mean duration of symptoms before presentation for all cases was 34.9±53.9 months. As expected, the mean duration for benign tumors was the lengthiest—54.6±64.7 months, while those of intermediate and malignant tumors were 5.5±3.5 and 14.9±28.4 months, respectively. Similarly, the mean duration of symptoms for soft tissue and bone tumors was 33.8±52.1 and 37.2±57.8 months, respectively. As well, the most commonly affected sites in this study were the mandibular (57/29.7%) and maxillary (36/18.9%) regions (Table 2), which also reflected on the sarcomas that recorded the highest occurrence in the mandible with 43(48.9%) cases and 23(26.1%) cases in the maxilla, respectively.
Site Distribution of Orofacial Mesenchymal Tumors
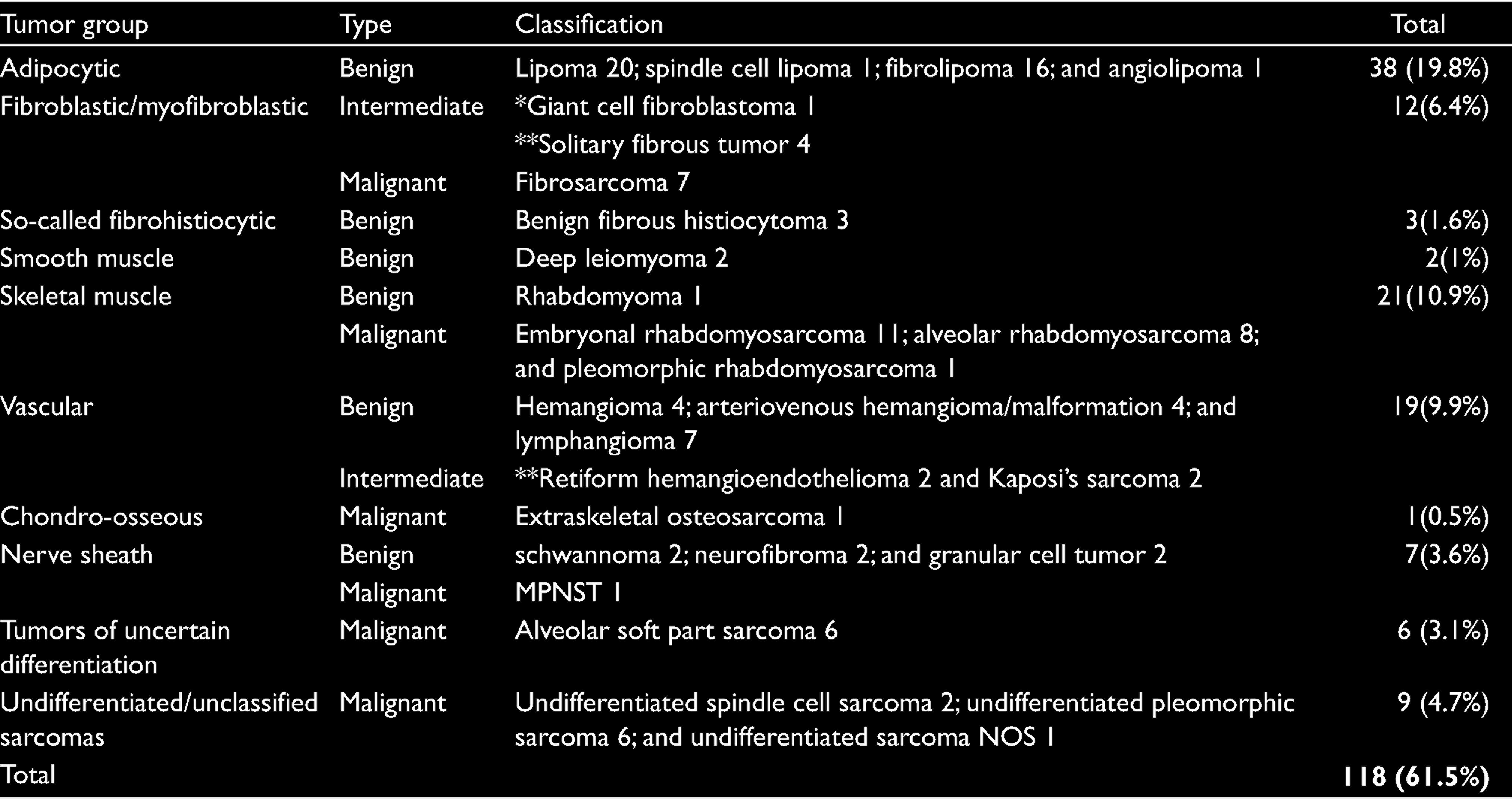
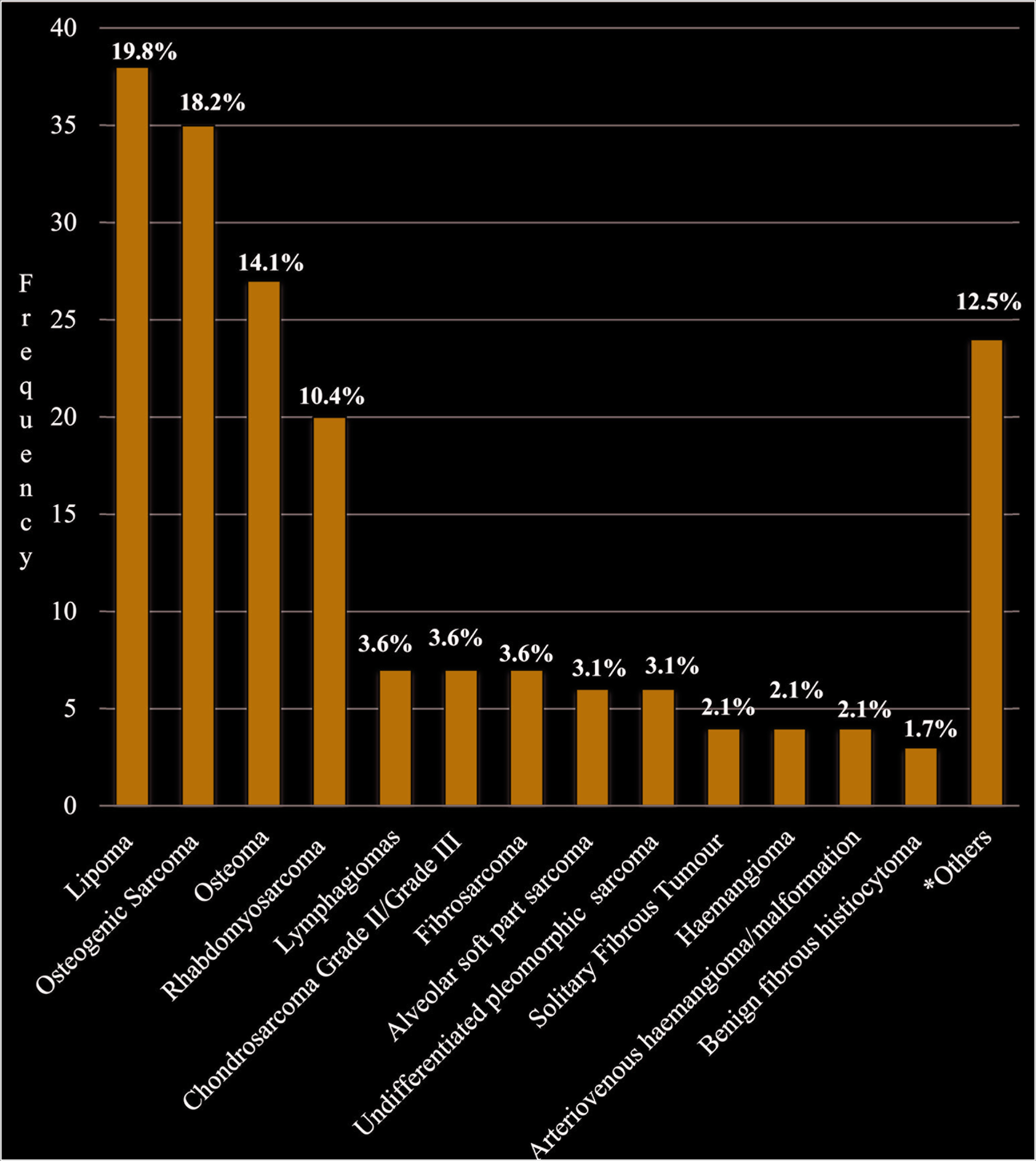
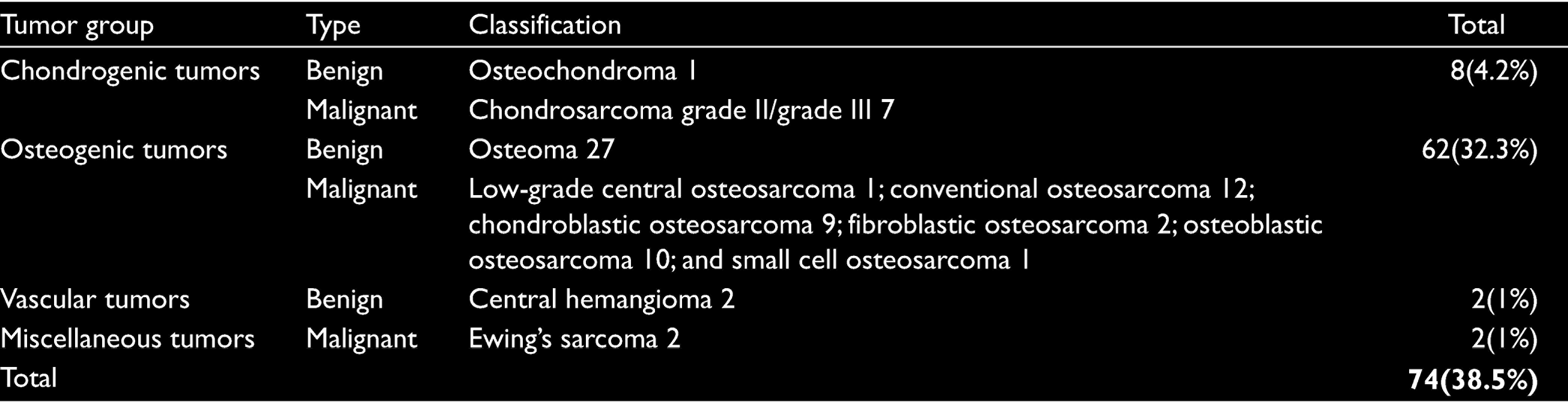
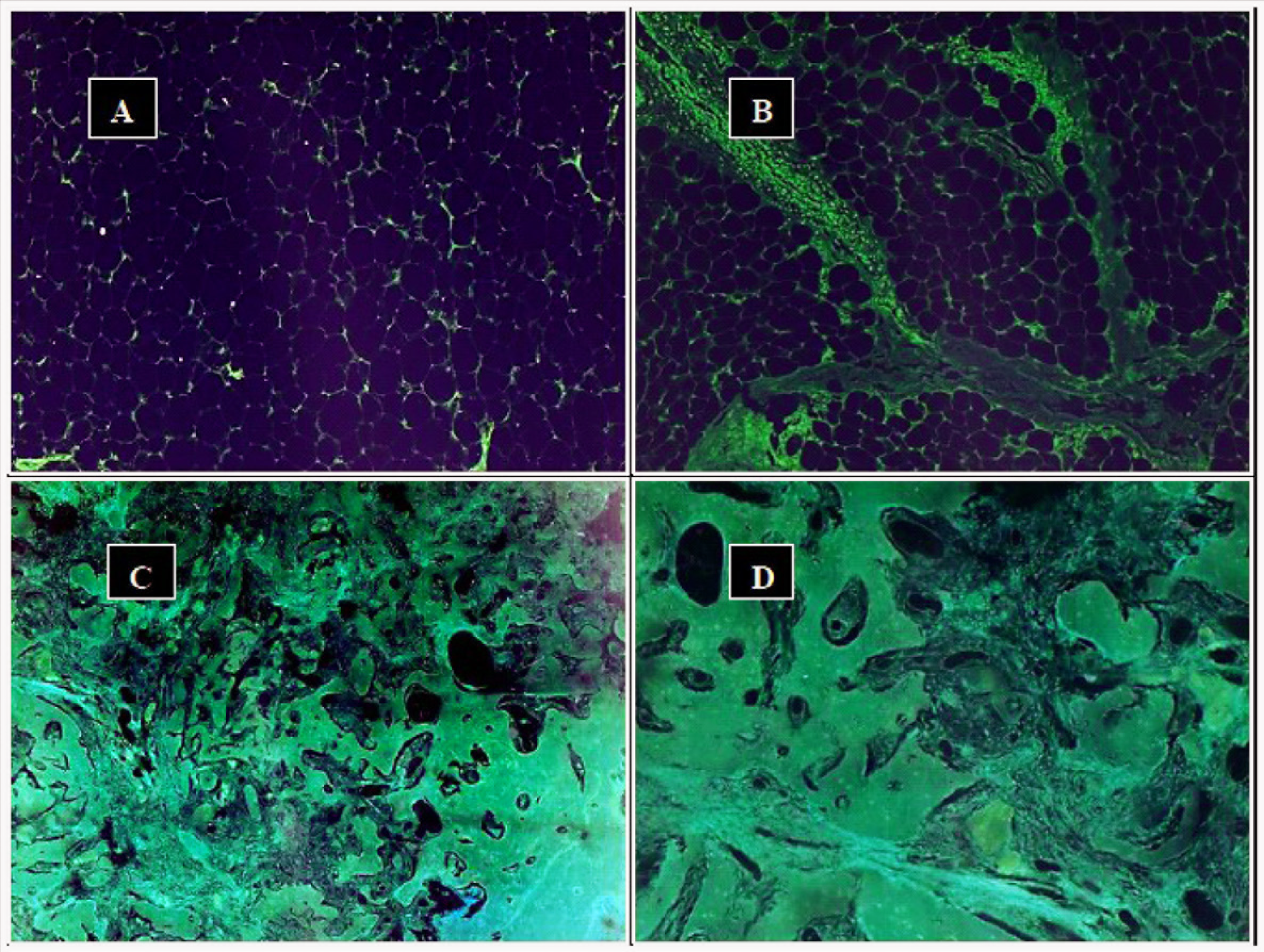
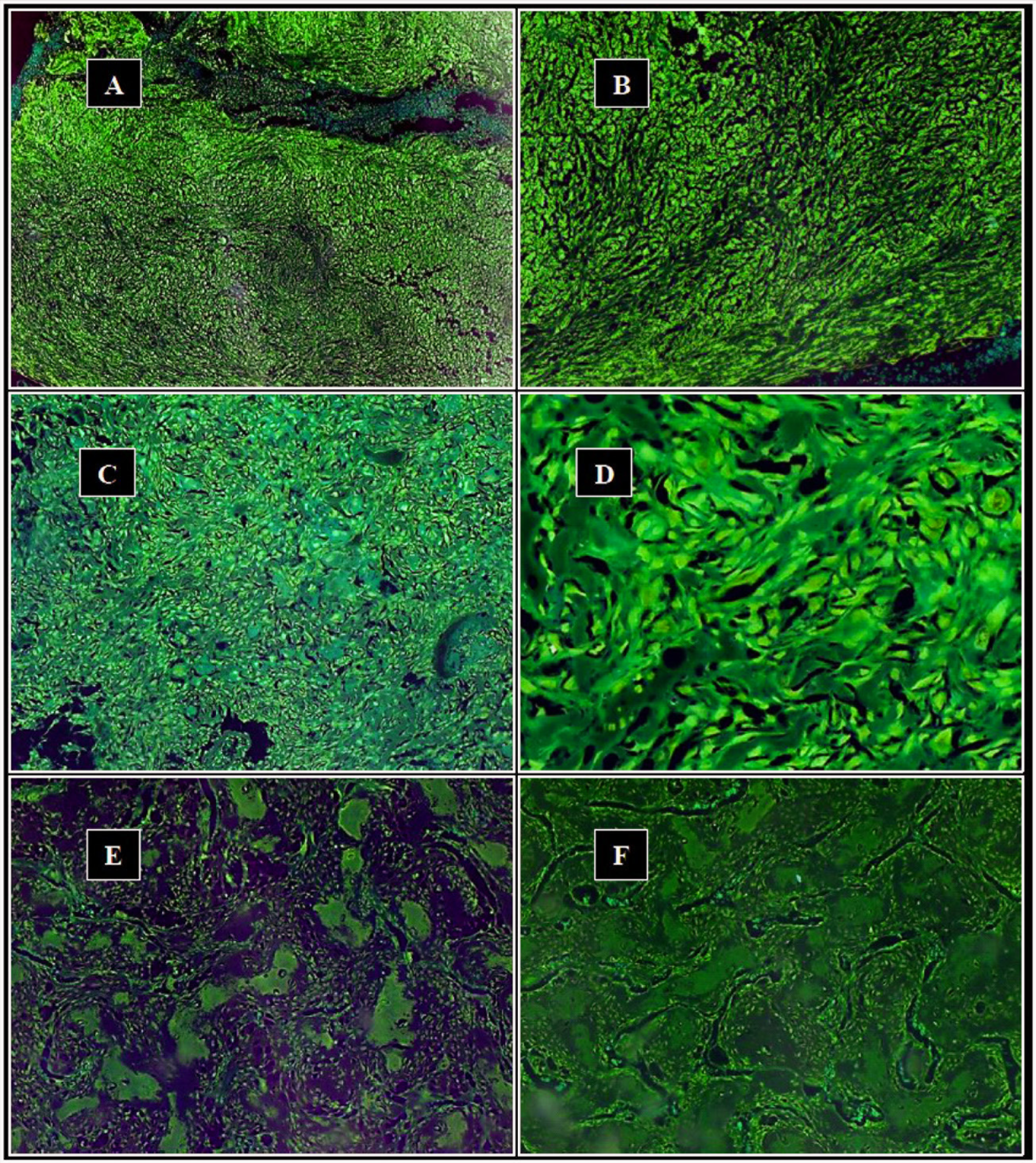
Adipocytic tumors, consisting of lipoma and its variants, were the most prevalent tumors in the soft tissue series recording 38(19.8%) cases, while rhabdomyosarcomas constituted majority of skeletal muscle tumors with 20(10.4%) cases (Table 3, Figure 2). For the osteoarticular series as well as in the entire study, osteogenic tumors were the most prevalent tumors representing 62(32.3%) of all cases (Table 4). These comprised of 35(18.2%) cases of osteogenic sarcoma (making it the most prevalent sarcoma in this study) and 27(14.1%) cases of osteoma (Table 4, Figure 2). Photomicrographs of some mesenchymal tumors are shown in Figures 3 and 4.
Prevalence of Mesenchymal Soft Tissue Tumors According to the WHO 2013 Criteria
Prevalence of Mesenchymal Bone Tumors According to the WHO 2013 Criteria
Discussion
Mesenchymal tissues of the orofacial region either of soft tissue or bone are rarely reported conjointly. Disparities in terminologies used to describe neoplasms arising from mesoderm poised a challenge in the literature search, which limited comparison of the findings in this study with those of previous studies. Also, some of the studies available on mesenchymal tumors involved the head and neck region or the maxillofacial region, which are closely related to the orofacial region, though not synonymous. Notwithstanding, some findings in this study are comparable with those of previous studies.
This study recorded a higher prevalence of soft tissue neoplasms (61.5%) over bone tumors (38.9%), which was consistent with the findings in a previous study in the head and neck region. 13 However, higher ratios of 80:20 for soft tissue over bone tumors were recorded in the previous study suggesting that the orofacial region may have more osteoarticular tumors over STTs relative to other regions. Also, benign soft tumors in general have been reported to far outnumber sarcomas,18,19 but this study did not record such a wide variation, probably because STSs in the head and neck region are relatively more common when compared with other parts of the body. 12
Furthermore, orofacial sarcomas recorded in this study were equally distributed between STSs and bone sarcomas. This is in contrast to previous studies in the head and neck region as well as the maxillofacial and orofacial regions that predominantly recorded more STSs compared to bone/jaw sarcomas.20–23 This difference can be attributed to the inclusion criteria for head and neck sarcomas, which may have a wider surface area for tumors of soft tissue nature over those of bone in the orofacial region.
According to this study, lipomas along with its variants were the predominant histological type of benign STTs, which is in agreement with previous reports that consider it to be the most prevalent benign mesenchymal tumor in general and in the head and neck region as well.3,24–26 Also, rhabdomyosarcoma was the predominant soft tissue malignancy seen in this study, similar to the findings in a previous study in the orofacial region by Fomete et al., 27 and in the maxillofacial region by Agbara et al. 28 These findings, however, differed from other previous studies which recorded undifferentiated pleomorphic sarcoma, 29 unclassified sarcomas, 20 synovial cell sarcoma, 21 and malignant fibrous histiocytoma 30 as the predominant STSs in their studies.
Also, the prevalent benign bone neoplasm in this study was osteoma, but its prevalence amongst mesenchymal tumors is rarely reported. However, osteosarcoma was the most common bone malignancy seen in this study, similar to findings in previous studies.20,28 When considering orofacial sarcomas in all, osteosarcoma was the most prevalent orofacial sarcoma in this study, similar to the findings in some previous studies which reported same.28,31,32 However, other studies have reported otherwise with rhabdomyosarcoma, 33 Kaposi’s sarcoma,23,34,35 and malignant fibrous histiocytoma 30 being the predominant sarcomas in these studies. This variation may partly be because of study population as exemplified by the increased prevalence of Kaposi’s sarcoma in human immunodeficiency virus/acquired immunodeficiency syndrome patients.32,34,36
Overall, orofacial sarcomas seen in this study constituted 3.6% of all lesions seen over the study period. This finding was similar to 3% recorded by Ajayi et al., 37 but contrasted with other previous studies that recorded higher values for sarcomas among all biopsies received.22,23 Also, sarcomas constituted 14.4% of orofacial malignancies seen in this study. This differed from 18% recorded by Ajayi et al. 37 and 17.6% recorded by Fakuade et al. 38 Also in this study, a male predilection was observed for orofacial sarcoma, which is similar to the findings in previous studies on STSs either of the head and neck or of the maxillofacial/orofacial region.33,35,39 Conversely, this finding differed from other reports that found a female predominance,22,23 while another study found no gender predilection. 30
The peak age group of sarcomas in this study was third decade of life. This was in agreement with the findings of Kamulegeya 22 and Hammas et al., 33 but differed from the report of Okoh et al. 30 which recorded a peak age group of second decade for orofacial sarcomas. Also, the mean age at presentation of sarcomas in this study was found to be lesser than the findings in most previous studies.22,23,30,33
With regards to the site of occurrence of orofacial sarcomas, this study was in agreement with a few studies, mainly because these studies were in the orofacial region, similarly recording the mandible as the most prevalent site of affectation.28,30,35
The WHO classification of soft tissue and bone tumors is used primarily for trunk and extremities, but has also been applied to the head and neck region. However, its applicability in the orofacial region is unknown. This study attempted to do this and recorded 26 diagnoses in a total of 161 tumors in 32 groups of neoplasms out of 52 groups present in the WHO 2013 classification. The anatomical/histological differences in dissimilar areas of the body may account for nonrepresentation of some tumors in certain areas. Also, some entities which are not considered primarily as tumors of mesenchymal/connective tissue origin were excluded from this study. For instance, giant cell tumors, even though they are bone tumors, are primarily because of the proliferation of giant cells and not of mesenchymal/ connective tissue origin, justifying their exclusion from this study. Also, some tumors represented in the WHO classification already have well-defined classifications in the orofacial region/jaws (e.g., aneurysmal bone cyst) and thus should not be considered to be of connective tissue origin. Therefore, judging by our observation in this study, a basis to consider crafting a classification system for orofacial mesenchymal tumors, which would comprise only of entities seen in this region and primarily of mesenchymal origin, is being made. The merits or demerits of including odontogenic sarcomas, carcinosarcomas, and sarcomatoid tumors among orofacial sarcomatous lesions should also be considered.
Conclusion
The clinicopathologic features of orofacial mesenchymal tumors in this study are largely in line with those of previous studies. However, the WHO 2013 classification primarily used for the trunk and extremities may not be suited for use in the orofacial region because of the number of tumors present in the WHO classification that are alien to this region. Also, entities that are not primarily considered to be of mesenchymal origin in the orofacial region but are present in the classification may pose misperceptions in its use. Crafting of a classification system for mesenchymal tumors of the orofacial region would thus be necessary.
Footnotes
Acknowledgements
We are grateful to the staff of the Oral Pathology Department, UCH, Ibadan, for their valuable contribution in combing the archival records for the cases used in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.