
Abstract
Aim:
To compare and evaluate the implant stability quotient (ISQ) measurements by two different radio frequency analysis (RFA) machines, Osstell Mentor and PenguinRFA.
Materials and Methods:
Twenty bone-level implants (3.7 × 10 mm2) were placed on a bovine bone in this in vitro study. The ISQ measurements were performed with the PenguinRFA and Osstell Mentor machines using the multipeg of the Penguin system. The measurements were repeated three times for each direction and an average ISQ value was calculated. The results were averaged (mean ± SD) and the intraclass correlation coefficient (ICC) was calculated to assess the relationship between the measurements.
Result:
The mean ISQ values for the Osstell and Penguin machines were 77.60 + 2.11 and 78.05 + 2.04, respectively. The ICC was 0.958. The ISQ values obtained from the Osstell and Penguin machines were significantly compatible (P < .05).
Conclusion:
Both of the RFA devices provided similar and reliable ISQ measurements.
Introduction
The prerequisites for successful osseointegration have been determined for a long time, such as the biocompatibility of implant material, surface and macro design of the implant, the surgical technique, and an undisturbed healing phase.1,2 Primary stability (which is defined as the stability of the mechanical contact between the alveolar bone and implant at the time of implant placement) is essential for the undisturbed healing. When the criteria for a successful osseointegration are met, the host bone comes in contact with the implant surface and the implant becomes osseointegrated resulting in secondary stability. 3
Methods to evaluate the stability of the implant can be grouped as invasive/destructive or non-invasive/non-destructive methods; however, only the latter can be used in clinical practice. 4 The radio frequency analysis (RFA) is a commonly used non-destructive method. It is a bending test of the bone–implant complex. In RFA, a small force is applied with the help of a transducer, and the amount of displacement is measured. 5 Meredith et al. 6 first evaluated the stability of implants, which were mounted on an aluminum block and observed a relation between the resonance frequency and the stiffness of the surrounding material. Later, they published the RFA measurements of implants in the maxilla and reported that this technique could help in following the changes in the stability of the bone–implant interface. 7 After two generations of RFA machines; the technique was commercialized as Osstell (Osstell AB, Göteborg, Sweden). From the third generation of RFA machine onwards, the result of a measurement of implant stability is presented as an implant stability quotient (ISQ), which ranges from 1 to 100. 8 High ISQ values represent less displacement and, thus, more stiffness of the bone–implant interface. The fourth-generation machine, Osstell Mentor, has a metallic rod with a magnet on top, which can be screwed onto an implant. The magnet is excited by a magnetic pulse from a wireless probe. After excitation, the peg vibrates freely, and the magnet induces an electric voltage in the probe coil. This voltage is the measurement signal sampled by the RFA. This measurement is presented as an ISQ value. 5 Valderrama et al. 9 compared the cabled generation of this machine to the wireless one. The results of this study showed that both generations correlated well in terms of ISQ measurements even though the corresponding ISQ values could not be directly compared with each other but could not be compared directly in terms of ISQ measurements.
The new commercialized RFA machine, PenguinRFA (Integration Diagnostics Sweden AB, Göteborg, Sweden), is available for use. Till date, only few studies had compared the Osstell and the Penguin RFA machines.10,11 In one of these studies, 10 RFA measurements were performed on implants embedded in four different materials with different densities. The other study 11 reported the RFA measurements of 38 implants in 30 patients. Both studies reported a low correlation between the Osstell and Penguin machines.
The aim of our study was to compare the measurements of stability of implants by two RFA machines and evaluate the correlation between the ISQ results. The null hypothesis was that both machines are reliable and there would be no statistical difference in ISQ values between PenguinRFA and Osstell Mentor ISQ systems.
Materials and Methods
Setting and Design
A fresh bovine axis bone specimen was used for this in vitro study due to the similarities to the human bone and convenience to obtain. It was identified as a D2 bone by tactile sense.
Sample size calculation was determined by the Biostatistical Department from the Medical Faculty, University of Istanbul Aydin, Turkey. The minimum sample size for the study was statistically analyzed using Minitab 17 Statistical Software (computer software—demo version, State College, PA: Minitab, Inc. [
Study Method
Twenty bone-level implants, 3.7 × 10 mm2 were placed on the bovine axis bone according to the manufacturer’s instructions (Implance, AGS Medical, Istanbul, Turkey). A multipeg of the Penguin system was attached and measurements were performed parallel and perpendicular to the long-axis of the bone with the PenguinRFA (Integration Diagnostics Sweden AB, Göteborg, Sweden machine) (Figure 1).The measurements were repeated three times for each direction and an average ISQ value was calculated. The same measurements were performed by using the Osstell Mentor machine (Osstell AB, Göteborg, Sweden) without changing the multipeg (Figure 2).There is a cross-reference table provided by the PenguinRFA website, 12 which enables to correct the ISQ values obtained when using an Osstell machine together with a multipeg of the Penguin machine. The ISQ values obtained from the Osstell machine were corrected according to this cross-reference table and recorded.
ISQs were Measured after Multipeg was Screwed to the Implants with Penguin RFA
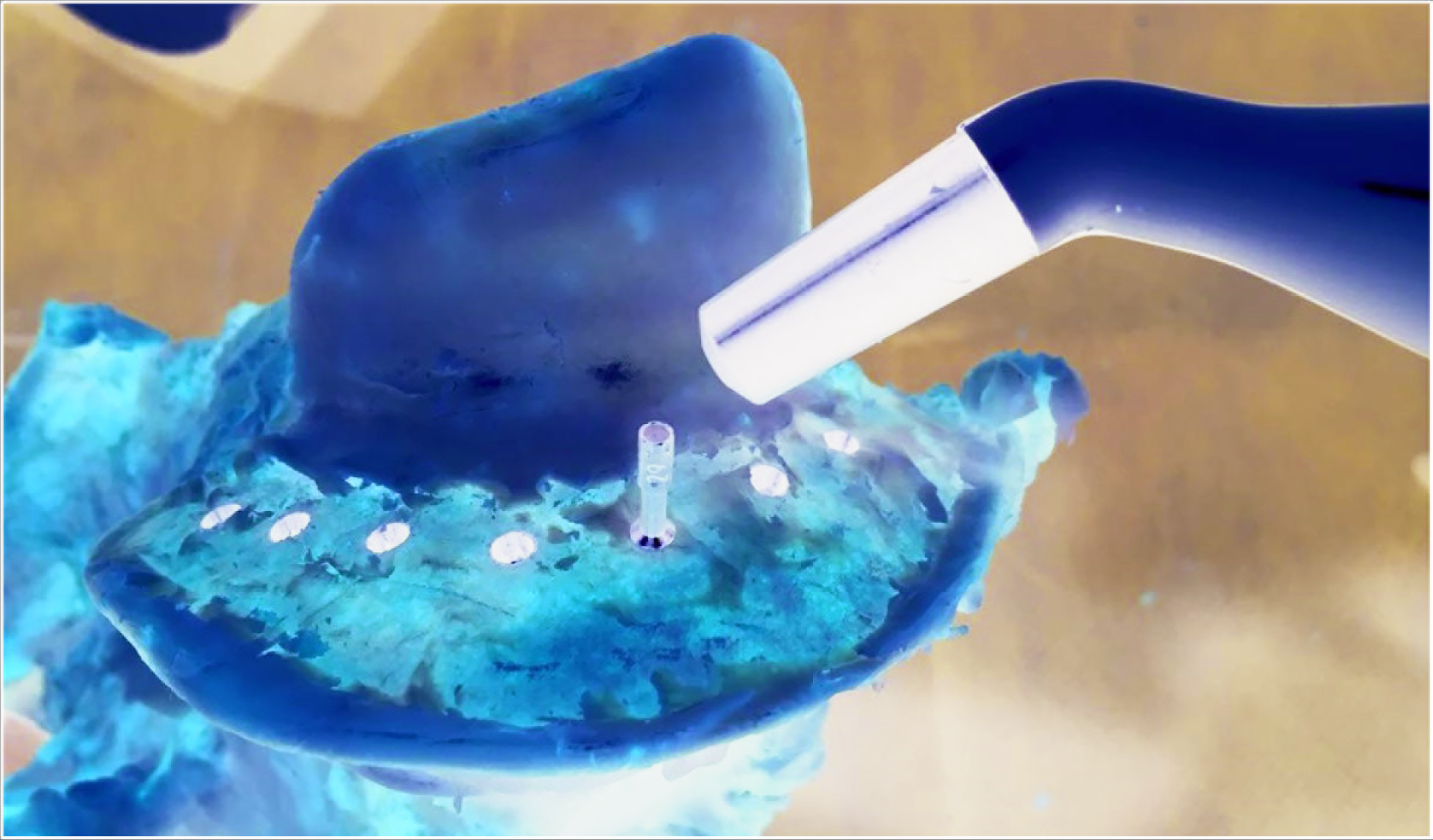
ISQs were Measured after Multipeg was Screwed to the Implants with Ostell Mentor

Statistical Analysis
The statistical analysis was carried out using SPSS v22 for Windows (SPSS Inc., Chicago, IL, USA). The results were averaged (mean ± SD) and the intraclass correlation coefficient (ICC) was calculated to assess the reliability of the measurements. The significance level was set at 5%, P < .05.
Results
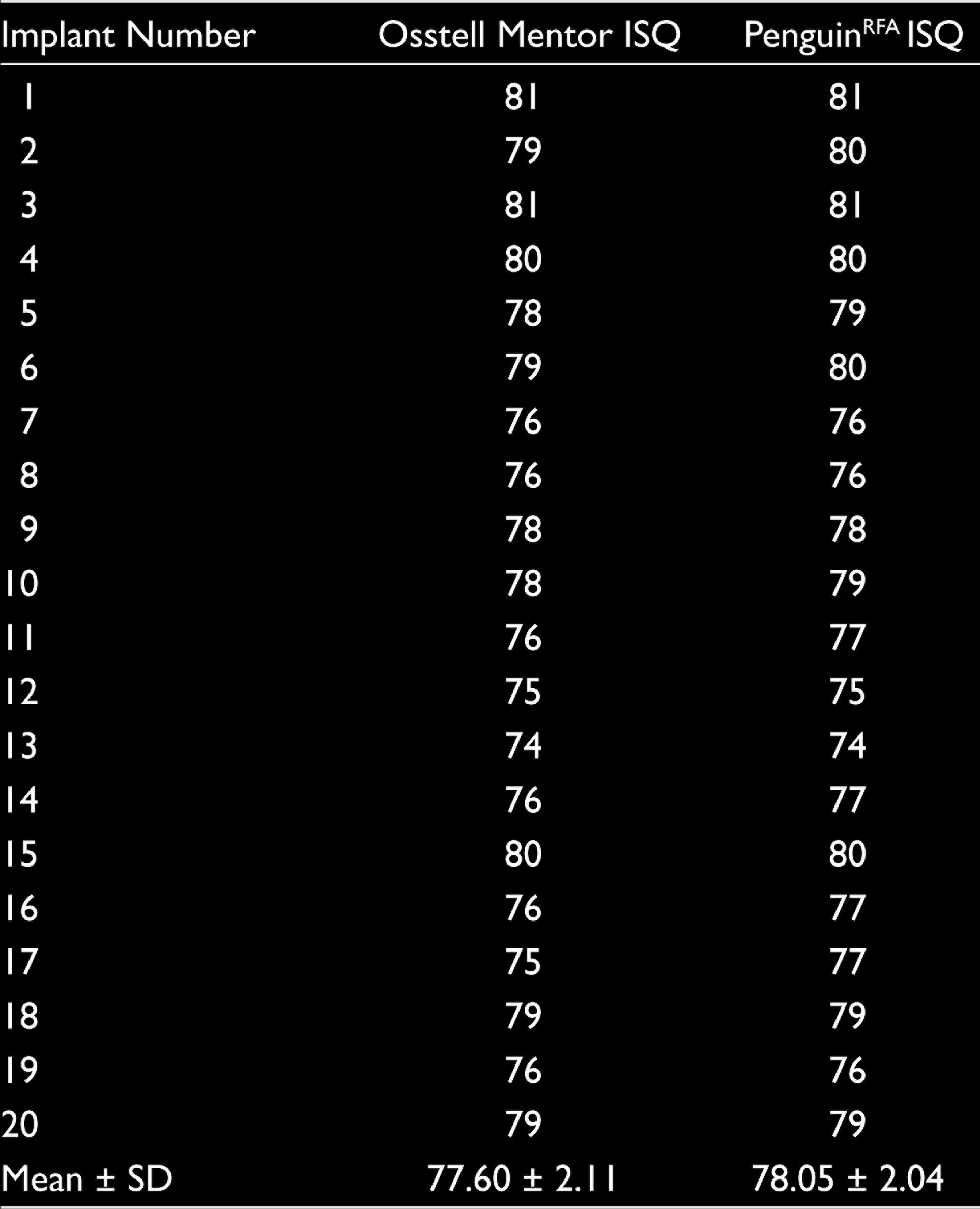
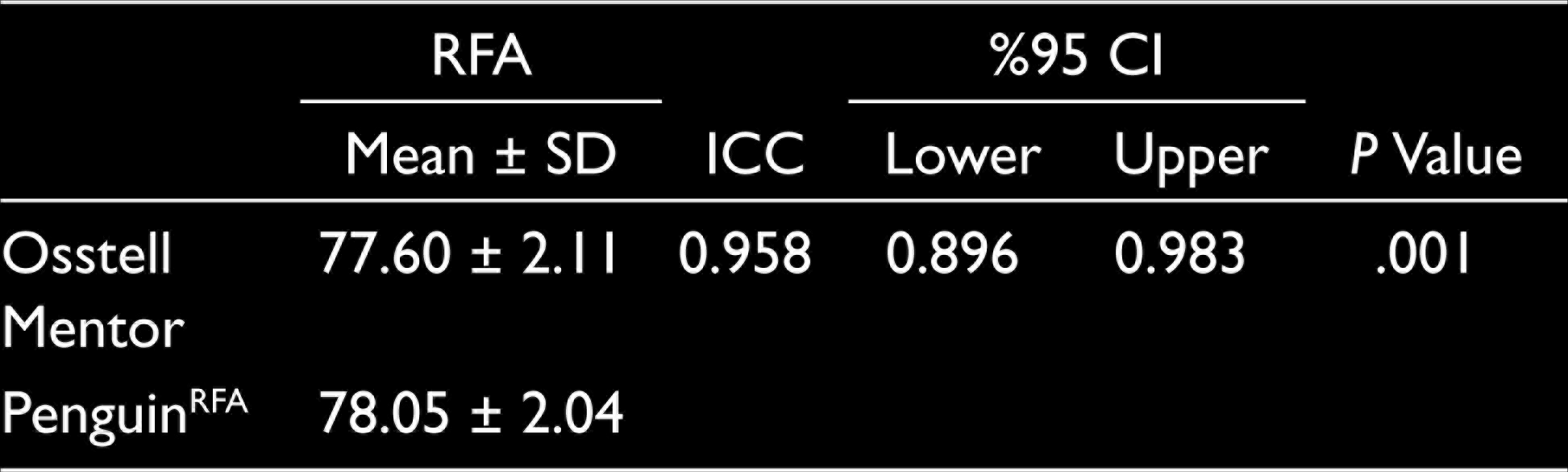
The ISQ measurements from both systems are shown in Table 1. The mean ISQ values for the Osstell Mentor and PenguinRFA machines were 77.60 + 2.11 and 78.05 + 2.04, respectively. The ICC was 0.958 (95% confidence interval: 0.896–0.983). The ISQ values obtained from the Osstell Mentor and PenguinRFA machines were significantly compatible (P = .001 and P < .05, respectively) (Table 2).
Measurement of Implants’ RFA Values with Osstell Mentor and PenguinRFA Machines
Comparison Between the Measurements of Osstell Mentor and PenguinRFA Machines
Discussion
This study compared Osstell Mentor and PenguinRFA systems in terms of the measured ISQ values of the implants placed on a fresh bovine axis bone. The bovine bone can easily be obtained and is frequently used in in-vitro studies. In this study, one bone allowed the placement of 20 implants ensuring that all implants were placed in a bone with similar density. In this study, the bovine bone was felt as D2 bone by tactile sense. Trisi and Rao 13 reported that hand-felt perception could distinguish a D4 bone from all other types. A study by Rokn et al. 14 reported that the tactile sense of the surgeon during surgery could clearly distinguish D1, D2, and D3 bones from each other but failed to differentiate a D3 bone from a D4 bone. The mean ISQ values in the Osstell group in our study were almost the same as those in the study by Herekar et al., 15 which reported a mean ISQ value of 77.35 + 3.26 for D2 bone. To evaluate the effect of different bone densities on the ISQ values, this study should be conducted with CT scan evaluation of bones as well. 16
It has been known for a long time that implant movement up to 150 microns during healing does not affect the anchorage of the bone to the implant unlike movements of more than 150 microns, which could prevent osseointegration.17,18 The study by Leucht et al. 19 showed the positive effect of mechanical stimuli on skeletal regeneration around implants and Ziebart et al. 20 showed an increase in the metabolic activity of osteoblasts at micromotions of 25 microns. On the other hand, Stadelmann et al. 21 showed that microstimulation (100 microns) at the bone–implant interface upregulates the osteoclast activation pathways. It has been proved that micromobility beyond 100–150 microns could result in fibrous encapsulation. Therefore, it is important to measure the baseline stability of the implants especially that are planned to be loaded immediately. Stability measurements can help the clinician to decide about the loading time.
RFA method has been used in studies on dental implant stability for a long time22–27; however, the reliability of the method is still being debated. In a clinical study, Nedir et al. 28 reported that the RFA method was not reliable in identifying mobile implants. Another clinical study by Huwiler et al. 29 also demonstrated that RFA was a specific but not a sensitive biomechanical test to assess implant stability and it did not provide predictive information about the loss of implant stability. Veltri et al. 30 investigated the relationship between the damping of osseointegrated implants and the fractal dimension of peri-implant bone. Their results also suggested that RFA measurements indicated the general stiffness of the bone–implant interface rather than its complex anatomy, and a non-invasive method to assess the biomechanical competence of the bone at the implant surface must be developed.
In an animal study, Abrahamsson et al. 31 could not find a relationship between the histological parameters of osseointegration and ISQ values and stated that the value of RFA to predict implant stability has to be questioned. An in vitro study by Çavusloğlu et al. 32 evaluated the efficacy of RFA and the results demonstrated that RFA was not a reliable method for the assessment of the initial contact loss around the implant. On the other hand, Cho et al. 33 defined the RFA method was as an objective, reliable, and useful method for clinical practice. Although there is controversy in the reports about the reliability of the RFA method, it is the most commonly used technique in clinical practice. It must be kept in mind that the RFA alone may not be a reliable indicator for the clinical assessment of primary stability 34 ; however, the ISQ measurement by RFA can be used as an additional parameter for the assessment of implant stability and decision making during implant treatment and follow-up. 35 New methods using inductive sensors 36 or measuring torsion frequency37,38 are under trial and claim better sensitivity and specificity in terms of implant stability measurements.
In the study by Buyukguclu et al., 10 the reliability and repeatability of Osstell and Penguin RFA machines were evaluated. Forty implants were embedded in different materials having different densities and the RFA measurements were performed three times with each machine. They concluded that both machines were sensitive to the density of the surrounding material and generated higher ISQ values when placed in dense materials. The reliability of both machines also increased with an increase in the density of the surrounding material and they concluded that the Osstell machine was more reliable than the Penguin machine. For implants embedded in self-curing acrylic resin, they recorded ISQ values of 81.3 + 1.77 and 83.43 + 6.02 from the Osstell and Penguin machines, respectively. The recordings by the Penguin machine were higher than those by the Osstell machine similar to the results of our study; however, the statistical significance of the difference between these measurements was unclear. Becker et al. 11 compared these two machines based on the ISQ measurements from patients. Thirty-eight implants in 30 patients were evaluated. The baseline ISQ recordings by Osstell and Penguin machines were 73.5 and 75.7, respectively. The recordings by the Penguin machine were higher than those by the Osstell machine and the difference was statistically significant. They also stated that the results of their study did not clearly delineate which instrument registered the ISQ recordings most accurately. In a recent study, 39 findings were similar with our study results. The researchers recommended that the use of multipegs instead of smartpegs when a clinic is equipped with a magnetic Osstell device.
Osstell and Penguin RFA systems have their own pegs, smartpeg and multipeg, respectively, screwed to the implants for measurement. The main difference between these two pegs is that the smartpeg allows use in a single patient only, whereas the multipeg is made of titanium and is autoclavable. According to the developers of the Penguin system, the clinicians can use both machines with both pegs. There are two cross-reference tables at the Penguin RFA website to correct the measurements performed with different RFA machines and pegs, such as an Osstell machine with the multipeg 12 or a Penguin machine with the smartpeg. 40 The cross-reference tables also suggest that these two machines are not identical and, therefore, more studies are needed to clearly understand the relationship between the Osstell and PenguinRFA measurements.
One limitation of this study is the lack of measurements by Osstell Mentor’s original smartpeg. This is the difference of this study from the aforementioned studies,10,11,39 which compared the Osstell Mentor and PenguinRFA machines, and this also prevents a direct comparison of studies. In addition, experimental setting was not similar with patient oral environment (saliva, mouth, temperature, etc.). Within the limitations of this study it can be concluded that a PenguinRFA system could provide similar ISQ measurements as an Osstell Mentor system and the hypothesis of the study was accepted. Further research is essential to evaluate the accuracy of implant stability measurements by the PenguinRFA machine.
Footnotes
Acknowledgements
The authors acknowledge AGS Medical (Istanbul, Turkey) for kindly providing the implant and the abutments.
Author Contributions
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.