
Abstract
Removable prosthesis, that is, complete and/or partial dentures cannot function as a substitute for natural dentition, but they have been and will remain the staple treatment for edentulous patients. An edentulous patient is found to be satisfied if prosthodontic rehabilitation restores his/her function with superior esthetics. However, not every case of edentulism, either complete or partial, can be treated with conventional methods of denture fabrication. When a patient is clinically presented with complications such as severely resorbed ridge, microstomia, hyperplastic and/or flabby tissue, xerostomia, osteoma, bruxism, and labially inclined premaxilla, then it becomes difficult for the dentist to fulfill the patient’s desire for both esthetics and function. There is a need for slight modification in the regular clinical procedures by altering the impression technique or the design of the prosthesis so as to achieve best results in compromised cases, commonly known as unconventional approaches. This article intends to highlight the unconventional approaches for the fabrication of complete denture prosthesis that can be kept in mind when such cases are encountered in our daily practice.
Introduction
The goal of complete denture prosthodontics is to ensure that the facial musculature is restored with sufficient support and tonicity that has set in owing to the loss of teeth, thereby making a prosthodontist to restore the lost function, provide better esthetics, and improve the tonicity of orofacial muscles. 1 There are various reasons for the tooth loss which not only alters the psychology of the patient but also disturbs the esthetics, phonetics, and functional occlusion. 2 Some common complications faced by a prosthodontist includes severely resorbed residual ridge, microstomia, hyperplastic/flabby tissue, xerostomia, bony protuberance/osteoma, prominent premaxilla, and grinding of teeth. These complications can be managed by the utilization of certain suitable materials and advanced techniques. 3 However, surgical treatment options are not always feasible owing to the lack of patient motivation to undergo an invasive procedure, financial, or systemic health limitations. 4
Therefore, increasing demands by the patients and revolutionary thoughts of prosthodontics have led to an outcome of the special, that is, the unconventional approach for fabricating complete dentures. Complete dentures fabricated for the patients with complications in a conventional manner prove out to be less satisfactory and come with certain disadvantages. 5 So, highlighting some of these unconventional techniques based on old fundamentals of Prosthodontia, these dentures are fabricated.
A flabby ridge has an excessive fibrous tissue deposition owing to which it becomes more displaceable. Flabby alveolar ridge is a result of replacement of alveolar bone with the hyperplastic soft tissue. Both maxillary and mandibular alveolar ridges are affected but more common in the maxillary anterior region. 6 Because of high displacement of fibrous tissue, impression making of the flabby ridge is difficult as soft tissue recoils to its original position and results in dislodgment of the denture. 7 Therefore, this flabby ridge has to be managed by using special techniques unless it adversely affects support, retention, and stability of the denture.
Retention, stability, support, esthetics, and preservation of supporting structures are the five basic principles of complete denture fabrication which may not be fulfilled for the cases with these complications by the conventional approach. 4 Hence, it is best to introduce these unconventional routes whenever needed. Therefore, the article highlights simple, effective, and noninvasive treatment alternatives to the classical conventional technique in edentulous patients.
Case Report 1
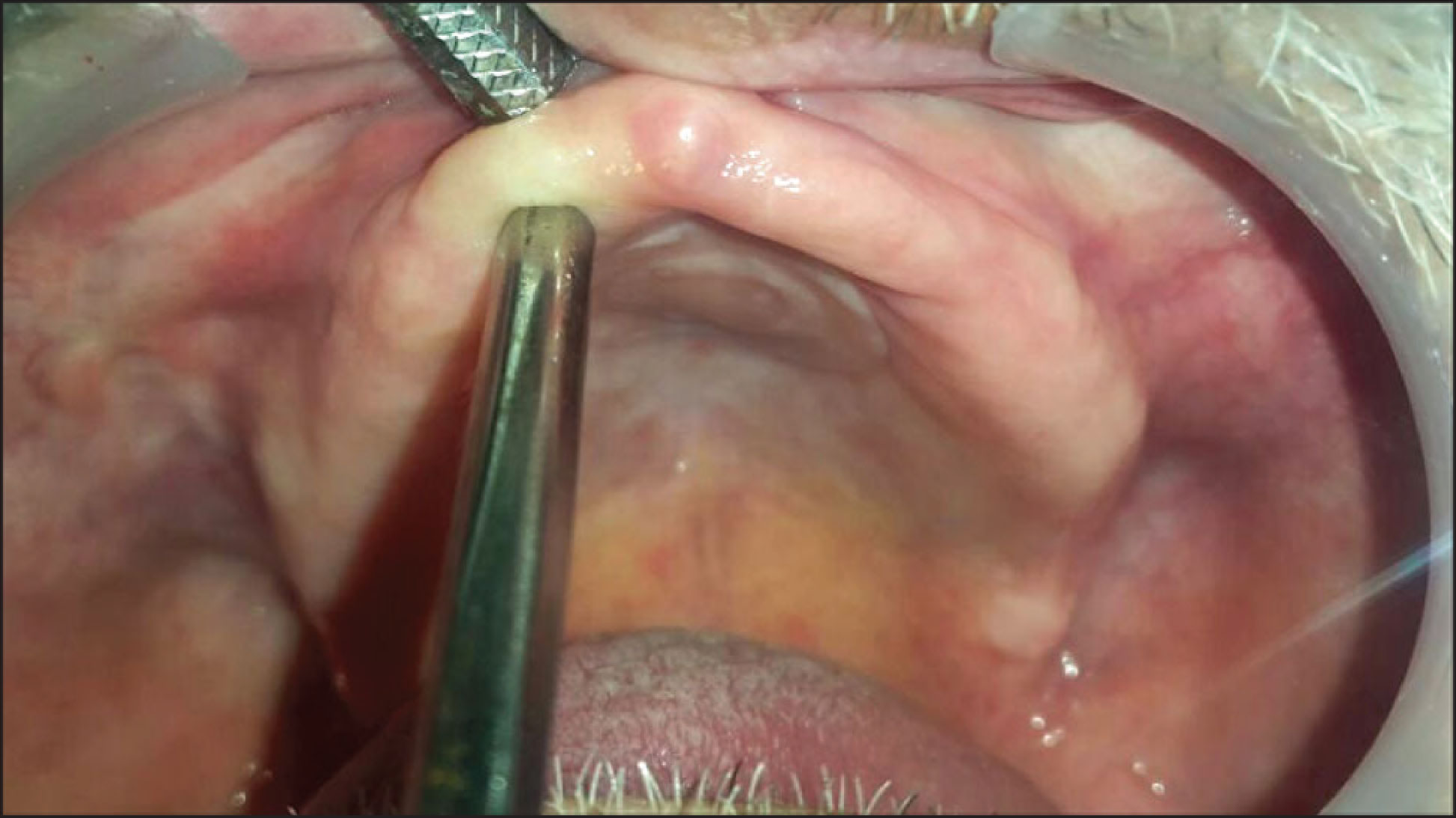
A 65-year-old male patient who has been wearing a denture for over the past seven years reported to the Department of Prosthodontics, Maharishi Markandeshwar College of Dental Sciences and Research, Mullana, Ambala, with the chief complaint of ill-fitting denture since last three years. On intraoral examination, the patient had completely edentulous maxillary and mandibular ridge with an area of flabby tissue in the maxillary anterior region (Figure 1). It was planned to rehabilitate the patient with a new set of denture using the Zafarullah Khan technique 8 or pressureless technique for recording flabby tissue in a undisplaced condition.
Clinical Procedure
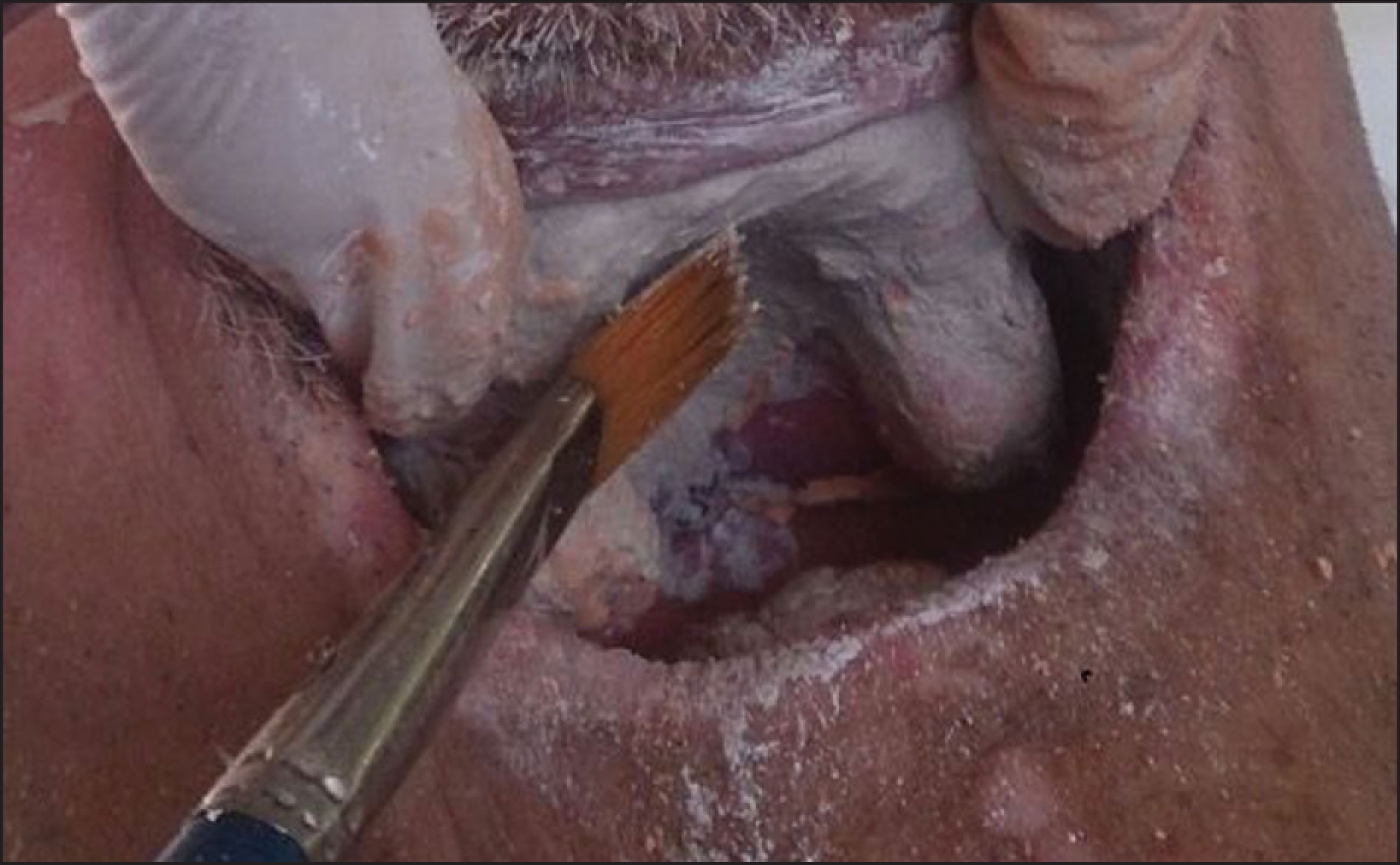
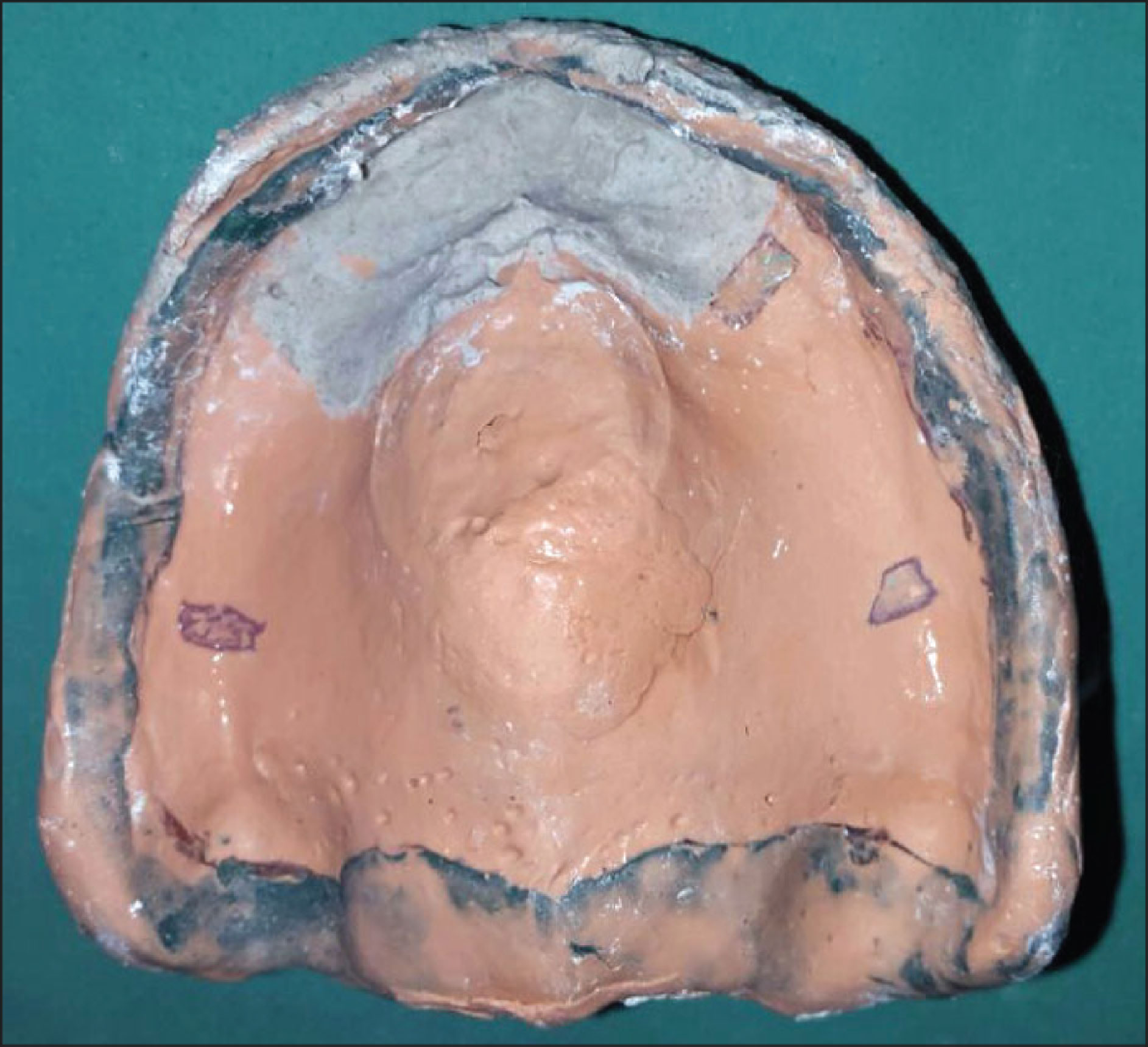
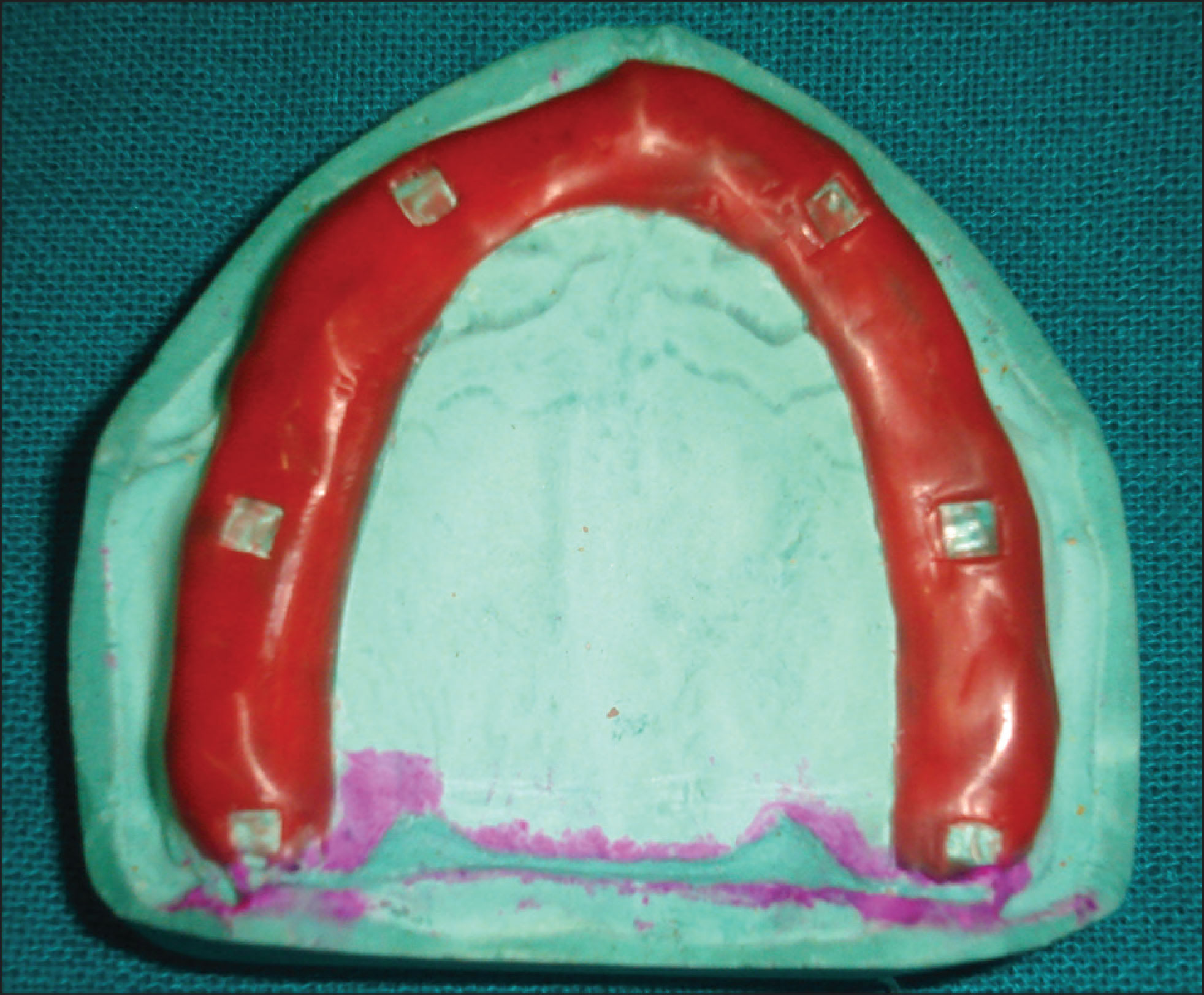
The primary impression was made using an irreversible hydrocolloid impression material (Zelgan, Dentsply, Delhi, India) in perforated edentulous impression trays. The primary casts were obtained and used to fabricate a custom tray by a self-cure acrylic resin (DPI RR Cold Cure, Mumbai, India). A spacer was adapted over the primary cast except in the region of flabby tissue. A special tray was fabricated providing a window in the region of flabby tissue. The borders of the tray were kept 2 mm short of the vestibular depth. Border molding was performed using a green stick compound (DPI, Pinnacle). After the completion of the border molding spacer, wax was removed and relief holes were drilled. The final impression was made with the zinc oxide eugenol paste (DPI Impression Paste, Mumbai, India), and the area with the exposed flabby tissue was painted with impression plaster. The impression plaster was allowed to set, and the tray was removed from the mouth (Figures 2A–D). Master cast was poured with dental stone (type III gypsum). Denture fabrication was then continued in a usual manner. The denture was delivered, and the patient was recalled after two weeks; the patient was comfortable using the denture.


Management of Repeated Denture Fractures
The construction of single complete denture opposing the natural dentition has certain drawbacks such as prosthesis fracture, instability owing to difficulty in obtaining occlusal balance, and achieving satisfactory esthetics. Denture base resins in a single complete denture have been frequently found to fracture under excess masticatory forces. 9 Metal bases have been proved to be a valuable alternative for denture bases opposing natural dentition to strengthen bases and less likely to break under normal conditions. 10
Case Report 2
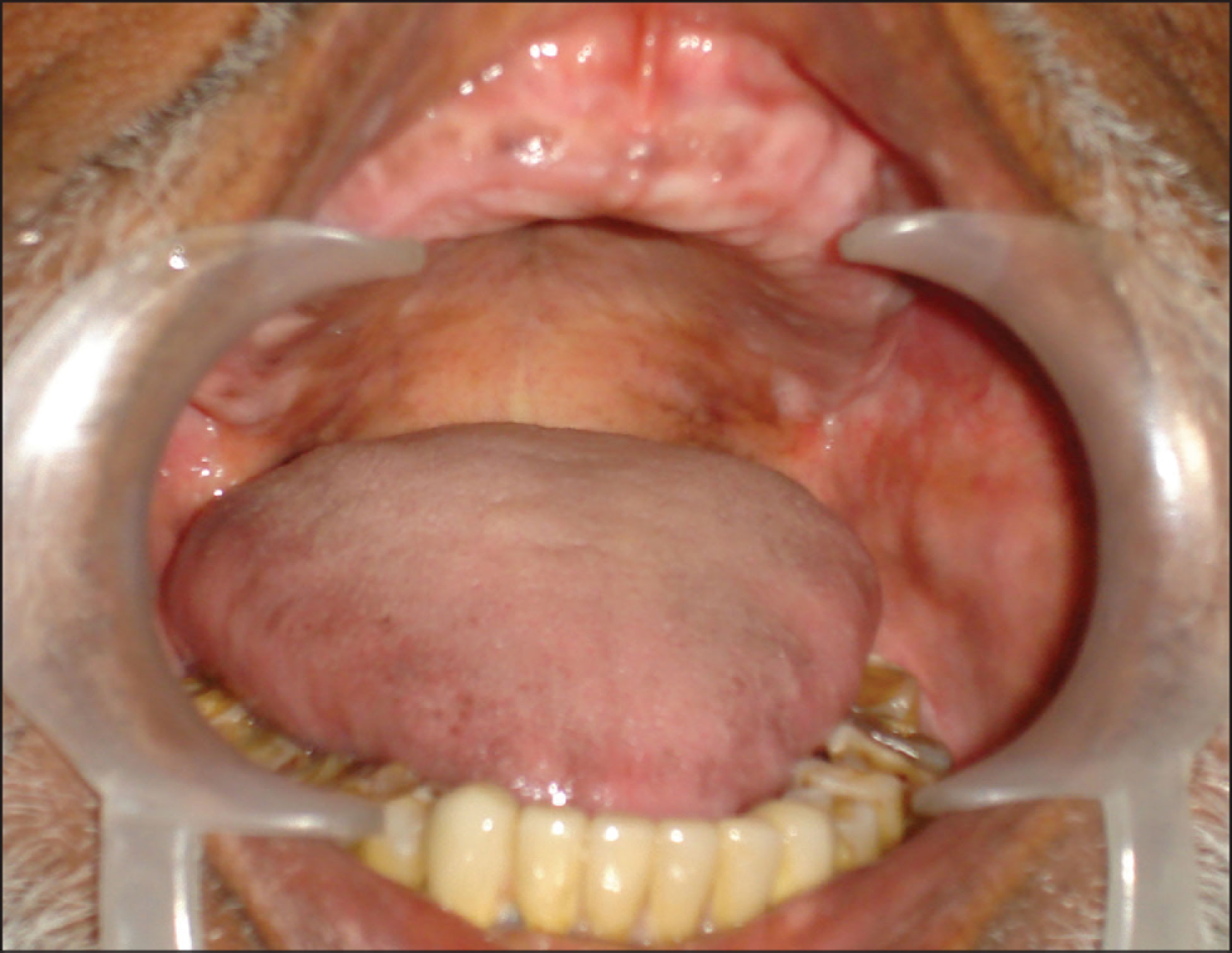
A 55-year-old male patient reported to the Department with the chief complaint of repeated fracture of a maxillary complete denture. Intraoral examination revealed completely edentulous maxillary ridge and opposing natural dentition (Figure 3). On examination, it was revealed that the previous denture was fractured from the midline, and retention, stability, and support of the denture were also compromised. The denture was relined, and the patient was advised for the construction of a new denture with the metal denture base so as to prevent the frequent fracture of the denture.
Clinical Procedure
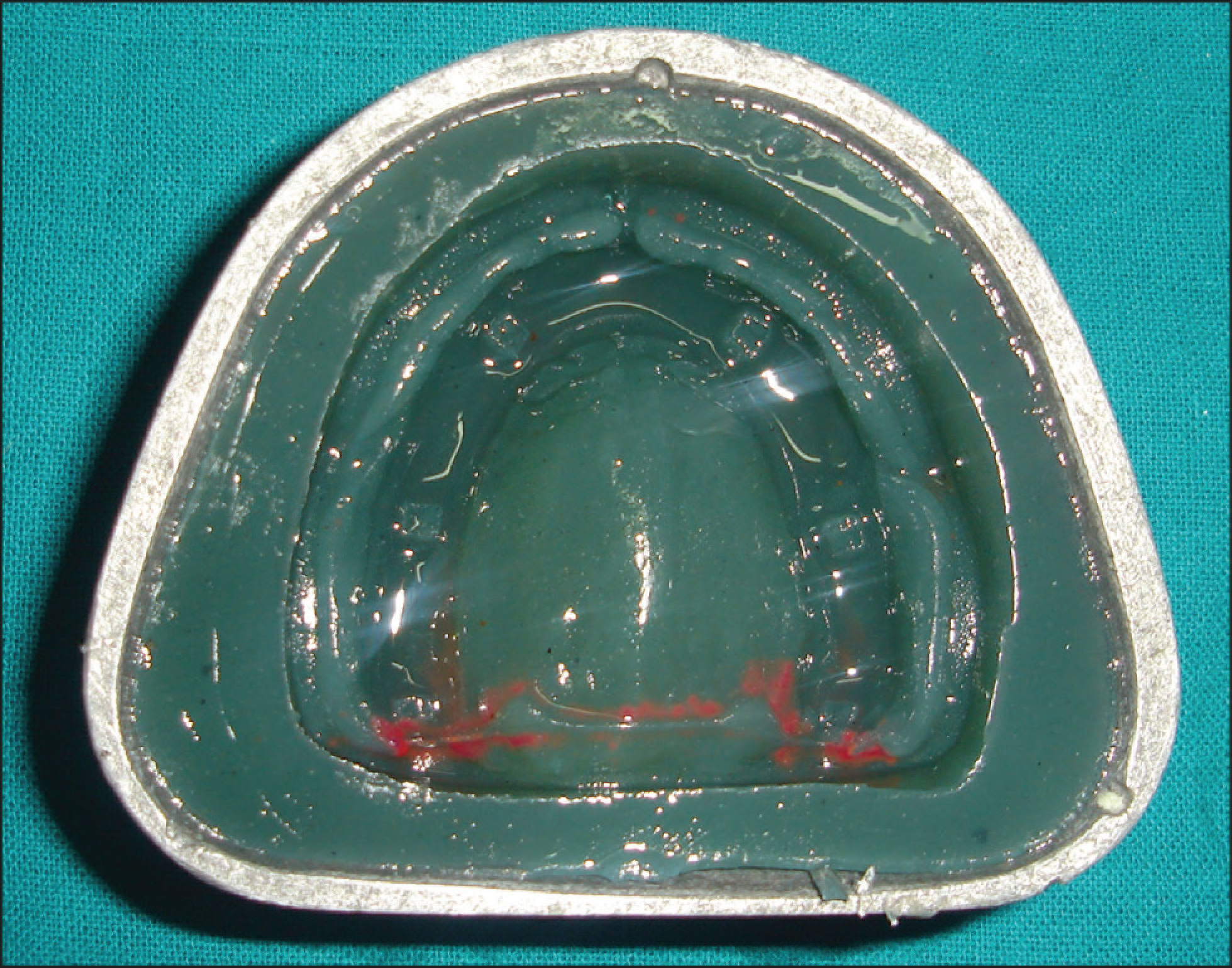
The primary impression of the maxillary edentulous ridge was made with an impression compound (API, ROLEX India), and the mandibular arch was made with an irreversible hydrocolloid impression material (Zelgan, Dentsply, Delhi, India) in a metal stock tray. The cast was poured using dental plaster and a custom tray was fabricated. Border molding of the maxilla was performed using a green stick impression compound (DPI, Pinnacle, Mumbai, India), and a secondary impression for the maxillary arch was made with the zinc oxide eugenol impression paste (DPI Impression Paste). The master cast was poured with dental stone (type III gypsum). A spacer was adapted on the primary cast in the alveolar region which provided the relief. The master cast was then duplicated with Agar, duplicating the impression material to form a refractory cast. The refractory cast was poured. On the refractory cast, the denture base pattern wax was adapted and the sprues were attached and invested (Figures 4A–C). The metal denture base was finished, adapted on the master cast, and polished. The maxillo-mandibular relation was recorded. Teeth were arranged in centric occlusion so that the centric relation records could be verified. Though a perfect balanced occlusion is impossible to achieve in such cases with the involvement of natural teeth, maximum effort was made to get an occlusion, which was close to the balanced occlusion. Try in was done in the patient’s mouth. The trial of waxed up maxillary single complete denture with metal denture base was done followed by acrylization with heat-polymerized acrylic resin (Figures 5A and B). Postinsertion instructions were given to the patient regarding its maintenance, nutrition, and hygiene.



Management of Severely Resorbed Alveolar Ridges
The conventional denture fabricated for the patients with severely resorbed residual ridge or with a large maxillofacial defect proves to be bulkier and heavier and usually exhibits compromised retention and stability of the prosthesis. As a result of the increased interarch space, the amount of the denture base material increases in denture fabrication, thereby making it less retentive. 3 So, a conventional denture with a hollow cavity can be planned to reduce the weight of the denture base.
Case Report 3
A 62-year-old male patient reported to the Department with the chief complaint of difficulty in chewing food and heaviness in his upper denture. History revealed that patient was edentulous for the past 15 years and had used many sets of complete dentures. On examination, it was found that both maxillary and mandibular ridges were severely resorbed. His upper lip was long, the inter-ridge distance was more than normal (Figure 6). The previous denture of the patient was heavy with attrited teeth and was under extended. Hence, it was decided to fabricate a new set of denture for the patient but in an unconventional manner so a hollow denture was planned.

Clinical Procedure
Preliminary and final impressions were made in a conventional manner. At the time of jaw relation, due consideration was given to adjust maxillary occlusal rims properly so as to provide proper aesthetics to the patient with a long upper lip. Teeth were selected and arranged in a balanced occlusion and try-in was done first for anterior teeth and then for posterior teeth. All the procedures were carried out by the conventional method till the dewaxing stage. Half of the heat cure polymethyl methacrylate (PMMA) (Trevalon, Dentsply India Pvt. Ltd, Gurgaon, India) at dough stage was positioned accurately over the dewaxed mold, and then salt crystals were placed over it. Above that, the remaining heat cure resin was packed and cured at 74 °C for 7–8 hours. The cured denture was retrieved, and three holes were made in the thickest palatal area. All the residual salt crystals were removed by flushing water with the high pressure syringe through the holes. After making sure that all the salt crystals have been removed, the escape holes were closed with autopolymerizing resin. The hollow cavity seal was verified by immersing the denture in water; if no air bubbles are evident, an adequate seal is confirmed (Figures 7A–C).



Discussion
The above case series presents the most common difficulties challenging the dentist: flabby alveolar ridge, repeated fractures of maxillary denture, and severely resorbed residual ridge. In the first case, the fibrous tissue in maxillary ridge acts as a consequence to tooth loss that can be explained as the replacement of residual alveolar ridge by mobile fibrous tissue. Compromised retention/stability of the maxillary complete denture and easily displaceable tissue labially, buccally, or lingually are some of the problems associated with the flabby ridge. 11
Although various impression techniques have been described in literature to record flabby tissue. Liddlelow, Osborne, Hobkirk’s 12 and Lynch and Allen’s have described different impression techniques for accurately recording of flabby alveolar ridges. 13 Each technique has its own advantages and disadvantages. The technique described in this article does not involve extra clinical steps in the construction of complete denture. The impression materials used in this technique are widely used. The use of window and wax as described by Watson 14 minimizes the displacement of flabby tissue thus increasing the stability of the denture. This technique was also advocated by McCord 15 and Ahmed. 16
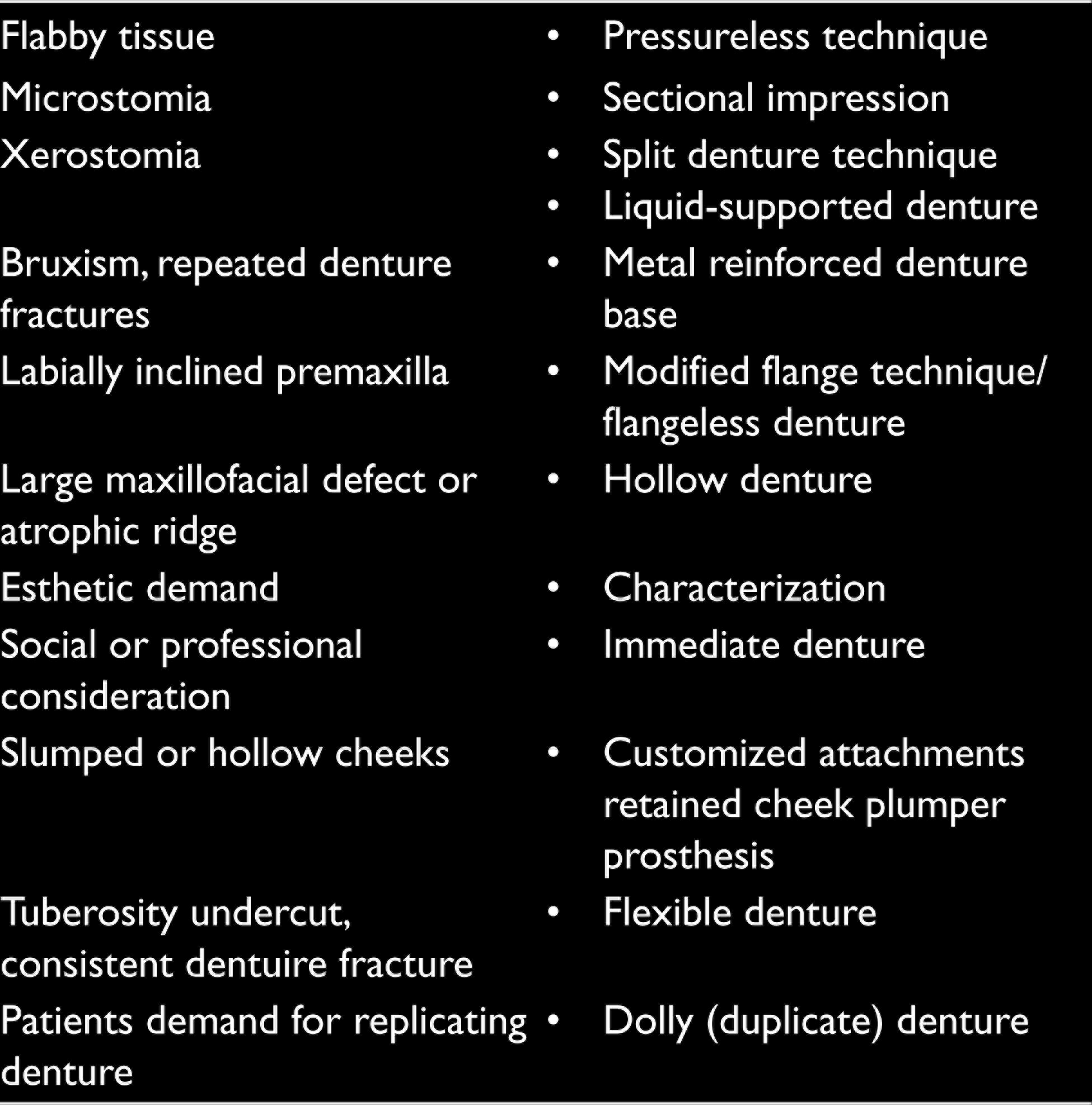
Routine Complications and Their Proposed Techniques 3
Although dentures made from PMMA (acrylic) resin show good mechanical, biological, and esthetic properties, they might fail due to excessive parafunctional and/or functional forces. Therefore, metal-based denture is used in the second case to strengthen the denture bases. Flexural fatigue failure, acrylic deformation, sharp changes in contour, pin holes, and residual processing stresses may result in the midline fracture of the denture base. Various approaches to reduce the incidence of midline fracture other than the use of metal bases can be: use of wires, bars, and high impact acrylic resin. 17 In this case report, the base was not extended till the vibrating line, but the acrylic resin base extended till the vibrating line, which shows favored and successful rehabilitation of the edentulous patient with the metal denture base with a regular follow-up period.
A metal denture base can be indicated in patients where additional strength is needed, that is, in patients with deep palatal vault, prominent residual ridges, shallow flat palates, and mentally compromised patients as they may drop their prosthesis. These dentures are generally fabricated from Co–Cr alloys (most retentive), Al, Ni–Cr alloys, Ti, and Au. 17 One of the significant advantages using thin metallic bases is the high thermal conductivity of the metal. Because of this, the sensation of hot and cold can be easily perceived by the patient. Some of the advantages of using thin metallic bases are rigidity, fracture resistance, good adaptability to the underlining tissues, denture plaque control, highly biocompatible, no fluid absorption, which may lead to dimensional changes, and no interferences with phonation. The major disadvantages include increased cost, difficulty in fabrication, and difficult to rebase. 18
In the third case, with the aim to treat the patients with severely resorbed residual ridges, weight reduction of dentures is one of the accepted techniques to make the denture lighter. All the necessary precautions must be carried out so that the denture base is not included in the planned area of hollow cavity of the prosthesis.
Several techniques have been described in literature for creating hollow cavities in dentures and obturators. For the first time, a technique using two split denture flasks for the fabrication of hollow denture was described by Holt 19 and Fattore et al. 20 It reduced the acrylic denture weight as much as 25%. Various authors have given different materials for creating a hollow cavity in a denture which includes a solid three dimensional spacer with dental stone, 21 cellophane, wrapped asbestos, 22 silicone putty, 19 or modeling clay 23 during laboratory processing.
The use of salt crystals in the present case report has advantages over previously described techniques for hollow denture fabrication. The salt crystals being heat labile melt during the curing procedure, and thorough flushing can be easily done unlike the tedious efforts made to remove putty from the denture, especially from the anterior region. Moreover, the escape holes made for salt removal were also smaller than the openings made for the other varieties of spacer used. This lost salt technique is simple to execute and utilizes a very cheap and easily available spacer material.
Apart from modifying the impression technique to get maximum denture bearing area, modifying the type of denture may also be better accepted by patients. Hence, less denture weight provides for healthy and comfortable living.
Conclusion
Patient satisfaction can only be achieved by accurate diagnosis and appropriate treatment plan. Better rehabilitation of the edentulous patient is possible with the appropriate use of these unconventional dentures. The above case reports provide us with adequate knowledge of use of these unconventional techniques to meet the prosthetic requirements of such compromised patients. Even though meta-analysis data and follow-up studies are minimal regarding these unconventional dentures, we deliver these special dentures in our routine practice for better patient compliance.
Clinical Significance
The various available treatment options and modifications in impression procedures allow a clinician to provide a more natural and esthetically pleasant rehabilitation to the patient, thereby satisfying his/her esthetic, phonetic, and functional demands.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Patient consent:
Informed written consents were taken from all patients at time of participation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.