
Abstract
Angina bullosa hemorrhagica (ABH) is a rare, benign disorder characterized by one or multiple blood-filled blisters in the oral cavity (mainly soft palate, and sometimes oropharynx) with a sudden onset, that may lead to a potentially threatened airway. The most common hypothesis of its unknown origin is mild trauma. This lesion can easily be confused with other mucosal diseases or hematological disorders. Knowledge of the condition is important for correct diagnosis and treatment. Incision of the bulla, intubation, or even tracheotomy may be indicated. Here we present a case of 35-year-old woman with a complaint of dysphagia without dyspnea. During oral examination, a blue and/or purple blister on the soft palate was present. On endoscopic examination, an edematous uvula was observed, without other abnormalities. Eventually, the blister ruptured spontaneously and healed within one week without any sequelae.
Introduction
Angina bullosa hemorrhagica (ABH) is a relatively rare entity with an overall good prognosis. Knowledge of its clinical symptoms is crucial in order to facilitate an adequate workup, treatment, and patient counseling. In this article, we describe an overview of the etiology, pathophysiology, diagnostic workup, and treatment of ABH.
Case Report
A healthy 35-year-old female with no relevant medical history (no known allergies and no medication use) was presented at the emergency department with a swelling in her mouth after eating an unsalted assorted nut mix. She described that within seconds after eating, a swelling developed in the back of her throat, which led to dysphagia. There was no itching, pain, bleeding, or dyspnea earlier. It was not the first time she ate this kind of nut mix, but she had never had these complaints before. In the ambulance, the patient was administered a single dose of intravenous hydrocortisone and clemastine (Tavegyl®) on suspicion of angioedema.
In the emergency room, it was noticed that the patient was talking with a “hot potato voice.” During oral examination, we saw a blue and/or purple blister on the soft palate, extending into the uvula (Figure 1). On endoscopic examination, an edematous uvula was observed, without other abnormalities. Importantly, there was no pharyngeal swelling obstructing the airway.
Inspection of the Oral Cavity at Presentation

Given the location of the lesion and the possibility of a threatened airway, the patient was admitted for overnight observation. Additional laboratory tests were performed to exclude hematological disorders. Apart from a lightly elevated fibrinogen (5.1 g/L (normal 2.0–4.0 g/L)), no abnormalities were found (prothrombin time, activated partial thromboplastin time, thrombin time and hemoglobin were all normal).
The next morning, there was no change in the appearance of the blister. After 32 hours, the initial blister ruptured leaving a superficial erythema with white discharge (Figure 2). The specific presentation, location, and fast regression of the lesion and exclusion of other possible hematological diseases led to the diagnosis of ABH. Two days after admission, the patient was discharged from the hospital.
Inspection of the Oral Cavity 32 Hours After Presentation

For follow-up, we examined the patient one week later at the outpatient clinic. Inspection of the oral cavity showed normal mucosa with a mildly reddish area at the initial location of the blister (Figure 3). After 5 months, the patient was free of complaints, and the lesion had completely healed without any scar formation (Figure 4).
Inspection of the Oral Cavity Seven Days After Presentation

Inspection of the Oral Cavity Five Months After Presentation

Discussion
ABH was first described in 1967 and simultaneously named “traumatic (or recurrent) oral hemoplyctenosis.” 1 It is characterized by one or multiple subepithelial blood-filled blisters that cannot be attributed to any systemic disease or hemostatic disorders.
The exact incidence and prevalence of ABH are not known. However, Grinspan et al. 1 observed over 10,000 patients between 1990 and 1996 in their dental hospital and found 54 patients presenting with ABH. Between 1985 and 2016, a total of 225 cases were reported in literature. 2 The male-to-female ratio is about 1:1, and it is mostly seen in patients aged between 45 and 70 years.1–4
ABH is characterized by rapidly developing blue and/or purple blisters around 2–3 cm in diameter. These blisters mostly develop on the soft palate, although localization on the hard palate, tongue, and cheek mucosa is also described.2,4–6 The lesions are painless, but can be preceded by a burning sensation. The blisters rupture spontaneously within 24–48 hours. 3 After the lesion has ruptured, a reddish erosion and scraped white epithelial lining (previously the roof of the blister) is visible. These rest symptoms subside within 1–2 weeks after onset.6,7 The risk of recurrence is 30 per cent, and the blister may appear at a different location than the primary blister.1,4,8
The exact mechanism of the disease is unclear; however, in most cases, it seems to present after eating. During chewing, vasodilation of the oral mucosa occurs due to the parasympathetic reflex. This vasodilatation combined with the frail mucosa of the soft palate and the trauma of chewing hard food may easily lead to bleeding.2,5 ABH is also reported after other traumas in the oral cavity, such as surgical procedures by dentists, thermic injury, and intubation.2,4,5 Other contributing factors might be long-term usage of in-halation steroids, hypertension, and diabetes mellitus, which may lead to oral mucosa atrophy.3,4,7–10
The isolated nature of the swelling, typical clinical presentation, and rapid healing process of the blister are often sufficient to diagnose ABH. In clinical practice however, the diagnosis is often delayed by the unfamiliarity of the diagnosis of ABH and fear of other more serious diseases. During the workup, laboratory testing, including differential blood count, and coagulation assessment tests are indicated to exclude any possible underlying hemostatic defects. A tissue biopsy or analysis of blister fluid is not advised, because it may cause a secondary infection at the blister site.3–5
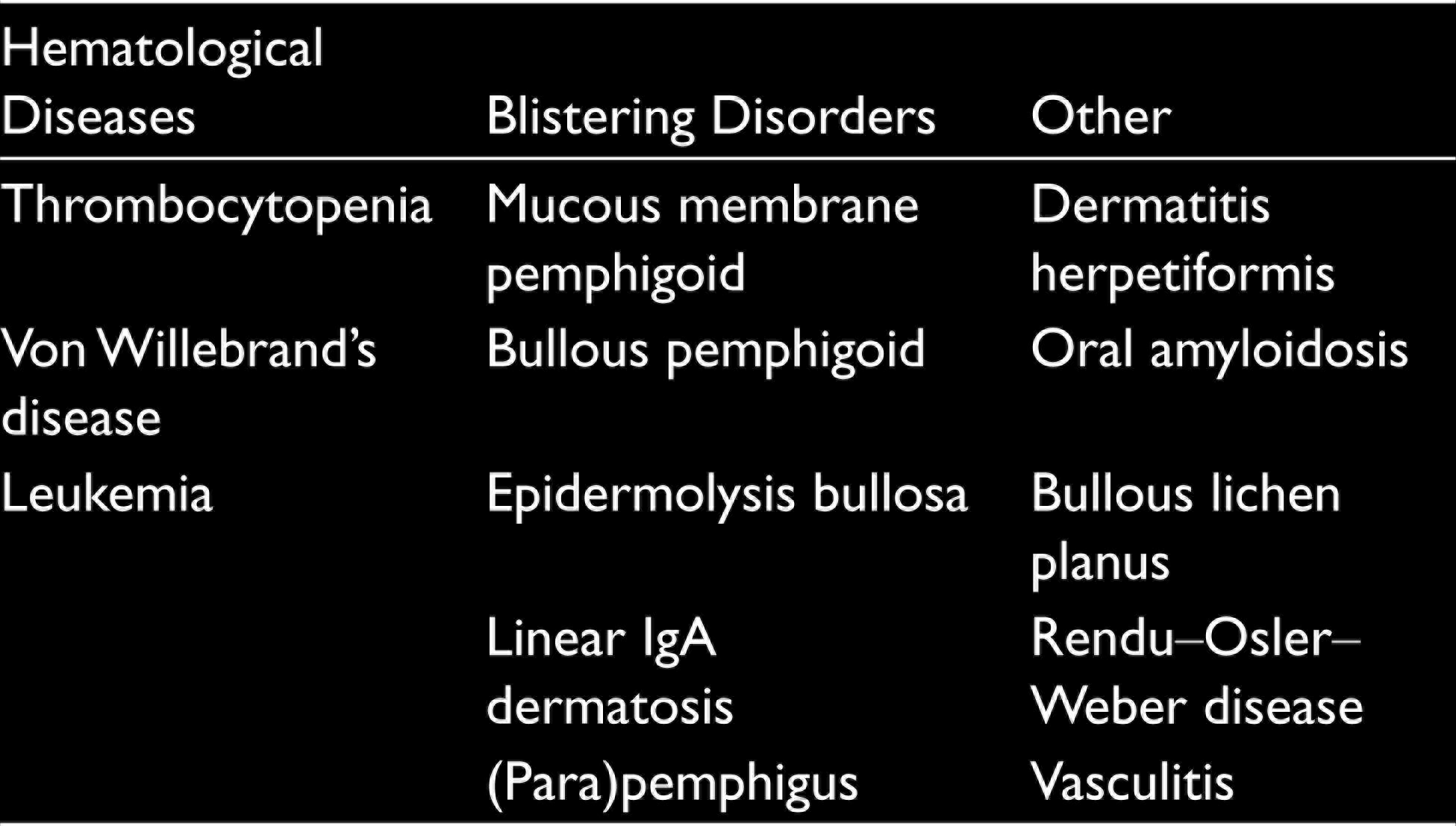
The differential diagnosis of ABH can be divided into three categories as shown in Table 1: hematological diseases, blistering disorders, and other.1,2,6 Hematological causes can be distinguished from ABH using clinical presentation and previously described laboratory tests. Other bleeding manifestations such as hematuria or epistaxis may be concomitant symptoms, guiding the clinician in the differential diagnosis. Blistering disorders and other causes often present as a more generalized condition with earlier manifestations in the patient’s medical history.1,4,11,12
Differential Diagnosis of ABH
The first step in ABH management is patient counseling. The overall benign character of the condition and its favorable prognosis should be highlighted. Only in the case of a potentially threatened airway, the incision of the bulla may be necessary. In rare occasions, an intubation or even a tracheotomy might be needed to secure the airway in case of a deeper protruding swelling.3,12,13 To prevent the secondary infection of the blister site, 0.12–0.25 per cent chlorohexidine gluconate can be used to wash the mouth.1,6 A long-term follow-up is advised to exclude any underlying disease. 6
Conclusion
ABH is a rare, benign disorder with acute, post-traumatic blood-filled blister development, in the oral cavity. The blisters heal spontaneously without any sequelae. Workup should start with a detailed history-taking, thorough physical examination and laboratory tests focusing on hematological causes to exclude other disorders. When ABH leads to a (potentially) threatened airway, intubation or tracheotomy may be necessary. Otherwise, watchful waiting and adequate counseling should be initiated. A long-term follow-up is advised to exclude underlying disorders.
Footnotes
Ethical Statement
The patient provided written informed consent for publication.
Acknowledgements
The authors would like to thank the patient for providing written informed consent for the publication of this case. A short version of this case report was published in Dutch in Ned Tijdschr Geneeskd 2019; 163. pii: D3837.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.