
Abstract
Aim:
This study aims to compare four implant-supported rehabilitation concepts of an edentulous mandible and determines the most biomechanically advantageous technique.
Materials and Methods:
Five models with four implants in different configurations were formed: four axial interforaminal implants, All-on-4 concept (two anterior axial and two posterior distally tilted implants), All-on-4v4 concept (four distally tilted interforaminal implants), All-on-4W (two anterior mesially tilted and two posterior distally tilted implants), and two axial interforaminal implants and two posterior extra-short implants. Straumann bone-level (4.1 × 12 mm) and tissue-level (4.1 × 4 mm) extra-short implants were used for this study. Spherical loadings from canine and molar regions were applied to evaluate tension, compression, and von Mises stresses by implementing 3D finite element analysis.
Results:
Among the alternative concepts, the classic All-on-4 and the All-on-4v4 techniques were the most successful treatment option in biomechanical terms. On the other hand, the use of extra-short implants in the posterior region was found to be the last method of choice. This was because of the high stresses on bones in most conditions, even though it balances the forces from the molar region on the implants.
Conclusion:
The results of the present study indicate that the classic All-on-4 and the All-on-4v4 techniques were the most successful treatment options in biomechanical terms for the rehabilitation of an edentulous mandible with four implant-supported fixed full-arch prostheses.
Keywords
Nomenclature
Introduction
The resorption of the posterior region of the mandible is more rapid than the interforaminal region.1,2 Often, additional procedures are required for implant placement in the atrophied posterior mandible.3,4 The current trends in implantology focus on implant placement, in different configurations, within the interforaminal region to avoid the additional procedures. Placing four axial implants with distal prosthetic cantilever appendages is one of the techniques proposed for the same. 5 Malo et al. 6 described the tilted placement of the posterior implants as the All-on-4 (ALL4) technique. They suggested that the shorter distal cantilever extensions and the longer implants could be placed by this technique, resulting in more biomechanically balanced load distributions. In the following years, Jensen et al. 7 suggested some variations in the ALL4 technique. The main idea of these variations lied in the angulation of anterior implants and tilted posterior implants. This technique was called “All-on-4v4,” (ALL4v4) and Jensen et al. 7 suggested that even severely atrophic mandibles could be rehabilitated using this concept. The use of short implants in the posterior region is another option allowing the elimination of cantilever extensions.3,4 Recently, the definition of a short implant was reserved for implants that are <6 mm in length.8–10
The primary aim of the present study was to compare the rehabilitation options of a mandible with severe posterior atrophy with four implants to support a fixed full-arch prosthesis by using three-dimensional (3D) finite element stress analysis. This study is also a biomechanical comparison of the effects of the tilted placement of some or all of the implants, the direction of tilting of the implants, and the use of extra-short implants in the posterior area to eliminate the cantilever extension. Thus, in the field of modern dental implantology, it is targeted to determine the most advantageous options among the latest trends, such as tilted placement and extra-short implants in terms of stresses on implants and bone tissue to support an implant-supported fixed full-arch mandibular prosthesis.
Materials and Methods
Material Properties of Implant and Prosthesis
The present 3D finite element analysis study used Straumann implants (Roxolid®, Institute Straumann AG, Basel, Switzerland) with a diameter of 4.1 mm. Straumann bone level (SBL) implants used in the anterior region of the mandible have a length of 12 mm, whereas Straumann Standart plus tissue level extra-short (ESI) implants used in the posterior region have a length of 4 mm and a neck area of 1.8 mm with a machined surface. The implants were made of the titanium–zirconium (Ti–Zr) alloy (Roxolid®).
Chromium–cobalt was used as the metal substructure in a hybrid prosthesis, and the superstructure was formed of the acrylic resin. In all models, the prosthesis was composed of 12 feldspathic porcelain teeth, including the first molar, and the dimensions were standardized for each model.
Models
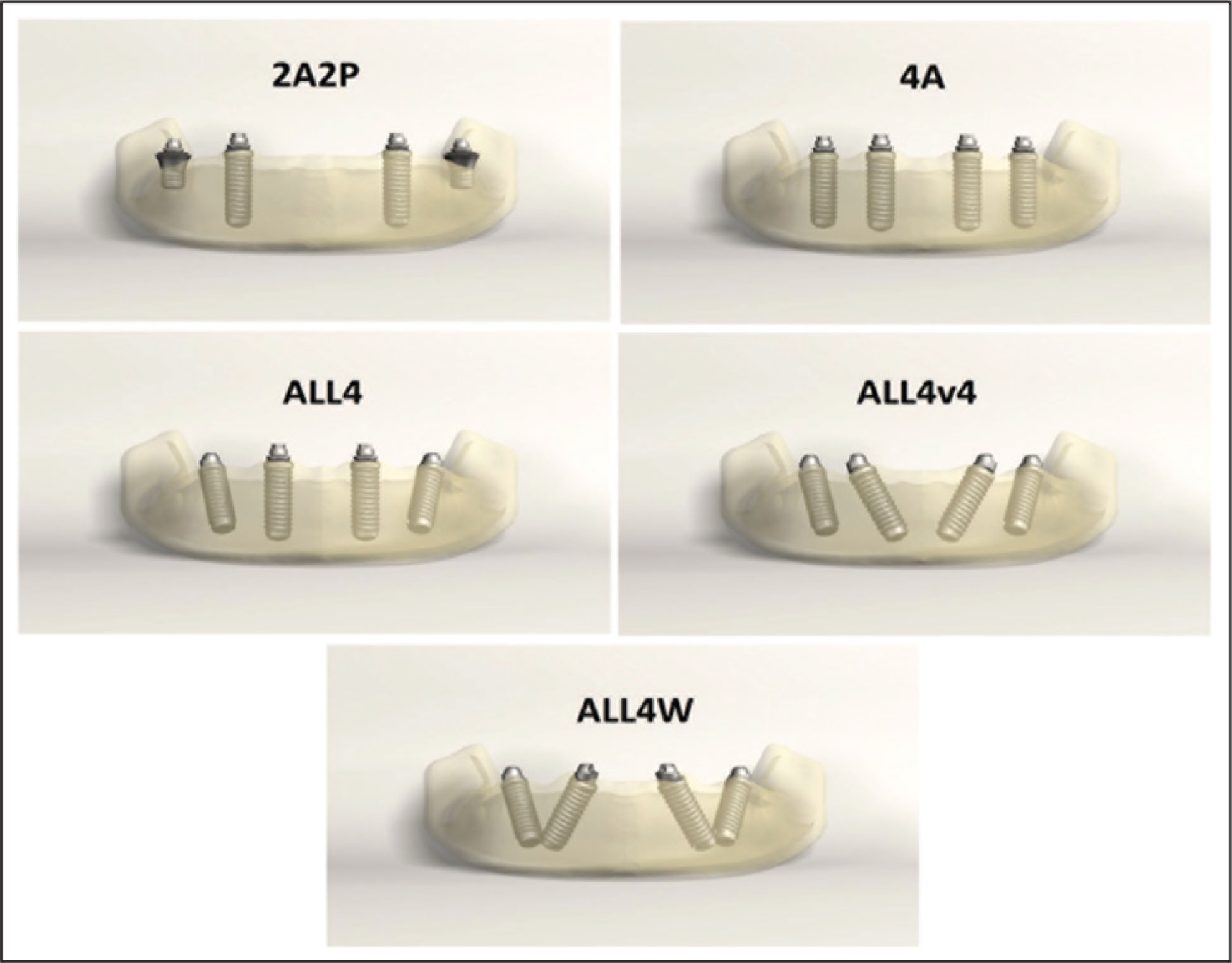
Five virtual mandibular models were created. At the time of labeling the models, abbreviations were considered based on the number of implants present in the anterior (A) and posterior (P) region or variations of ALL4 implant placement techniques.
A finite element analysis was conducted for five different implant configurations. In the 2A2P model, two SBL implants were placed axially in the canine and two ESI on the first molar. In the 4A model, four SBL implants were placed axially in the first premolar at the posterior and lateral tooth regions at the anterior site. In the ALL4 model, the anterior implants were positioned axial to the lateral tooth regions, and the posterior implants were positioned at an angle of 30° such that their emergence profiles corresponded to the second premolar tooth region. In the ALL4v4 model, four SBL implants were placed parallel to each other at an angle of 30° to the vertical axis, with emergence profiles corresponding to the canine for anterior implants and the second premolar area for posterior implants. In the ALL4W model, four SBL implants were placed at an angle of 30° to the vertical axis in directions opposite to each other, and the emergence profiles corresponded to the lateral tooth region for anterior implants and the second premolar region for the posterior implants (Figure 1).
The Models of Our Study
Modeling
Computed tomography images of patients with vertical atrophy in the posterior region were obtained and converted into the DICOM format. These data were then modified with the use of the VRMESH (VirtualGrid, Bellevue, USA) and Rhinoceros 4.0 (McNeel Europe, Barcelona, Spain) software. Dense trabecular bone tissue surrounded by a cortical bone thickness of 2 mm resembling D2 bone type was defined in the models. In the posterior region behind the mental foramina, 6 mm bone height between the mandibular nerve and the alveolar crest, 5 mm bone height between the mental foramina and the alveolar crest, and 14 mm bone height between the basal bone and the alveolar crest in the anterior mandible were defined. A bone width of 7 mm was defined along the entire alveolar crest in the mandible. A bone thickness of 1 mm was defined in the neck region of the buccal and lingual surfaces of the implants.
The implants, abutments, and prosthetic superstructures were scanned with a 3D scanner (Activity 880; Smart Optics, Sensortechnik GmbH, Bochum, Germany) and datasets were created in the stereolithographic (.stl) format. Rhinoceros 4.0 software was used to create the models. The implants were connected to the prosthetic superstructure by screws through the multiunit abutments.
Boundary and Loading Conditions
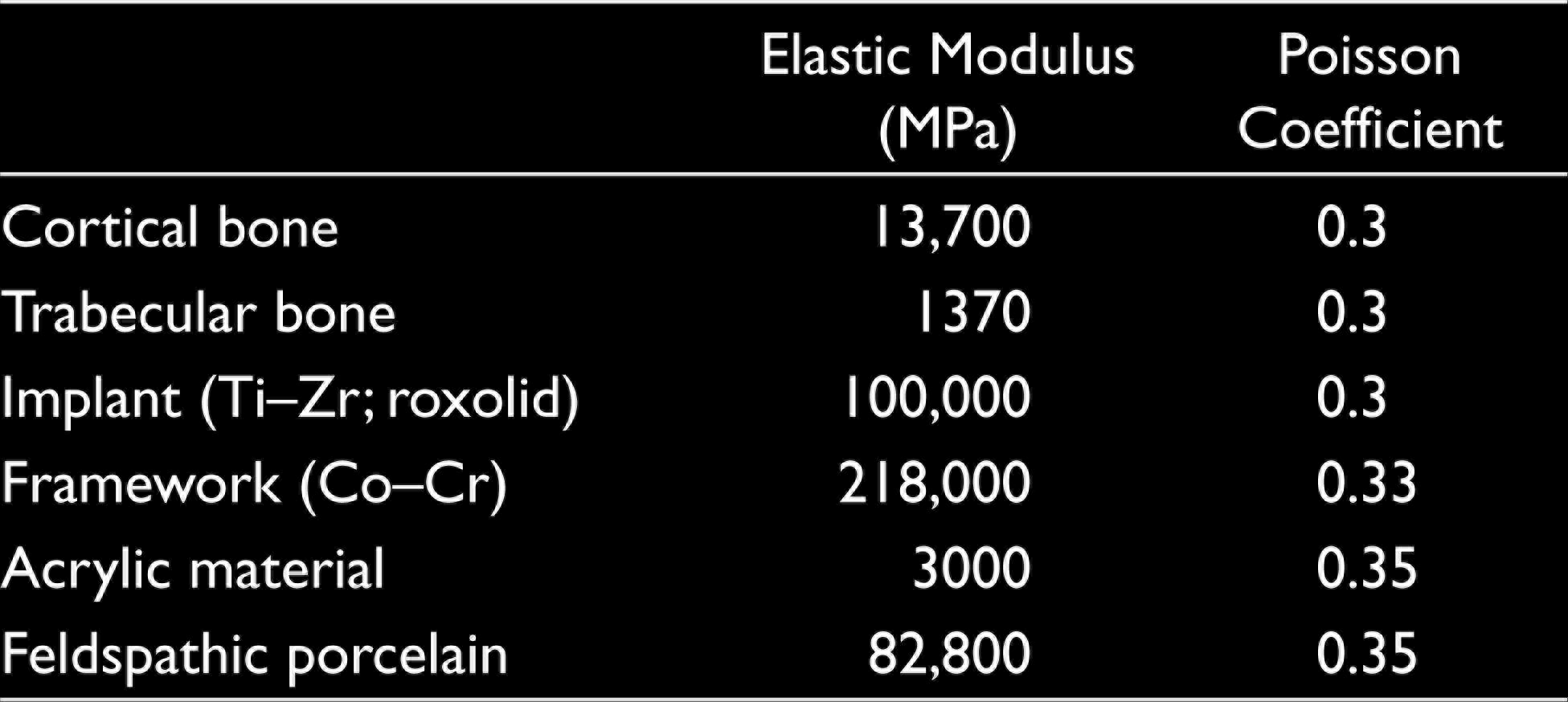
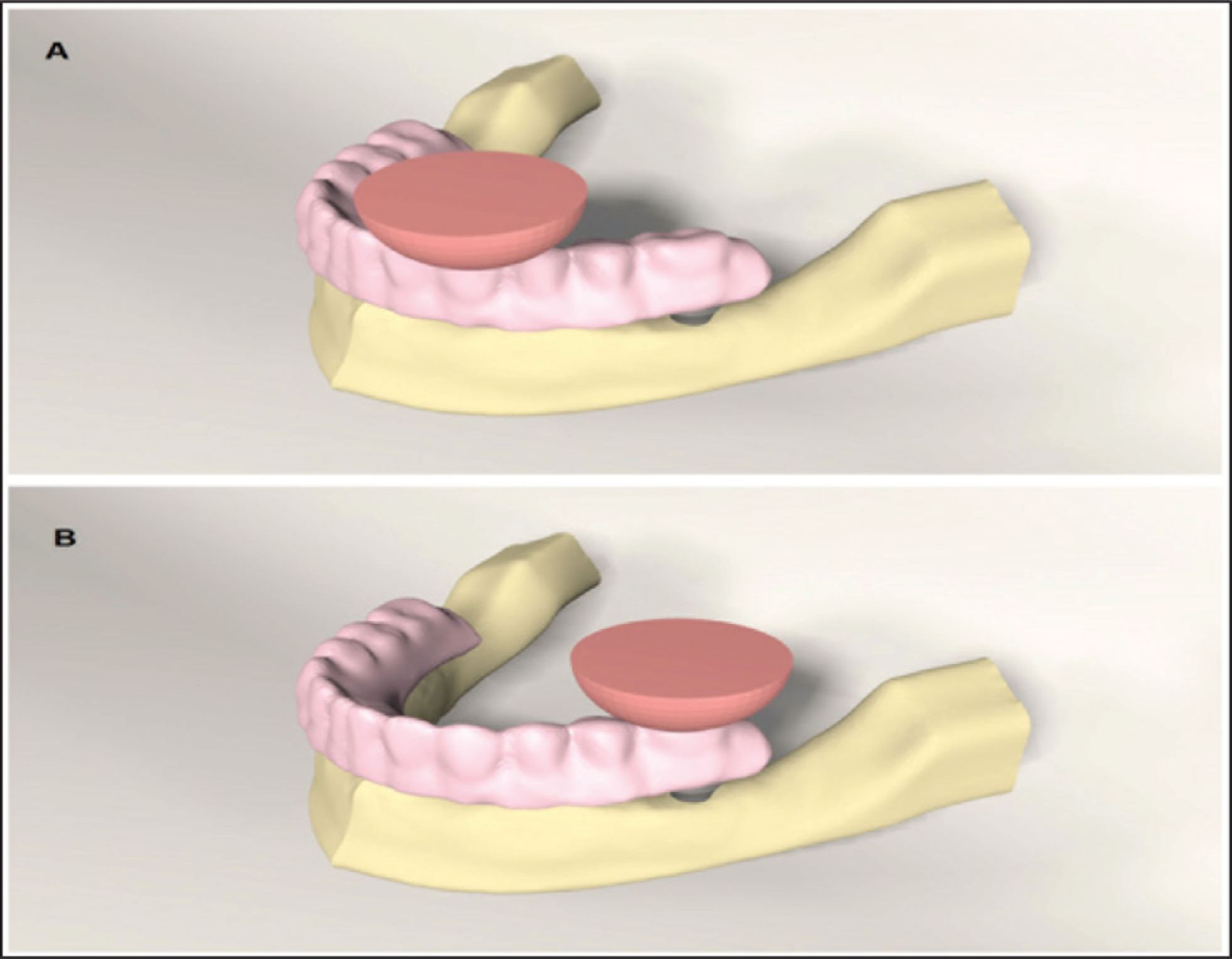
Boundary conditions were modeled as fixed in all directions. Modeled structures were simulated as tightly bonded. It was assumed that load transfers were performed according to the internal properties of the cortical and trabecular bone. The connection between the implants and the supporting tissues, the relationship between the multiunit abutments and implants, and the multiunit abutments and prosthesis were designed to transfer loads directly. The implants were assumed to be 100% osseointegrated. All materials used in this study were defined as homogeneous, isotropic, and linear elastic. Properties of prosthetic material, mucosa, cortical bone, trabecular bone, and implants were determined in accordance with a similar study (Table 1). For each model, two occlusal loads (100 N) were applied from a spherical solid material (12 mm diameter) placed in the left canine and left first molar regions for the simulation of foodstuffs, to visualize the chewing forces more naturally11–13 (Figure 2).
Mechanical Properties of the Materials
(a) Spherical Loading Applied From the Canine Region. (b) Spherical Loading Applied from the Molar Region
Analysis
Principal stresses were evaluated for brittle structures such as bone. Maximum principal stress (Pmax) represents tension stresses, whereas minimum principal stress (Pmin) represents compression stresses. To evaluate the stress formation in implants, von Mises stresses were analyzed. In this study, Pmax, Pmin, and von Mises stresses were measured in megapascals (MPa).
ALGOR FEMPRO (Algor Inc. Pittsburgh, USA) software was used for the analysis of the data. Since the data obtained from finite element analysis are mathematical calculations without variance, the results were not statistically analyzed; they were evaluated with scales instead. All stress values were represented using color and quantity scales. The results were evaluated in comparative terms.
Results
Maximum Principal Stresses
When stresses in the cortical bone were evaluated against forces applied from the canine region, the highest stress of 12.9 MPa was observed in the 2A2P model, whereas the lowest stress of 6.4 MPa was seen in the 4A model. Stress occurrences were observed to be close to each other in all three models, forming ALL4 variances. The highest stress of 3.8 MPa was seen in the trabecular bone in the 2A2P model, whereas the lowest stress of 0.7 MPa was observed in the 4A and ALL4W models. Stress values were closely related to each other in all models except the 2A2P model, where stress formation was nearly five times more than the other models (Figures 3 and 4).
Tension Stresses (Pmax) in Cortical and Trabecular Bone Against Loadings from the Canine and Molar Regions
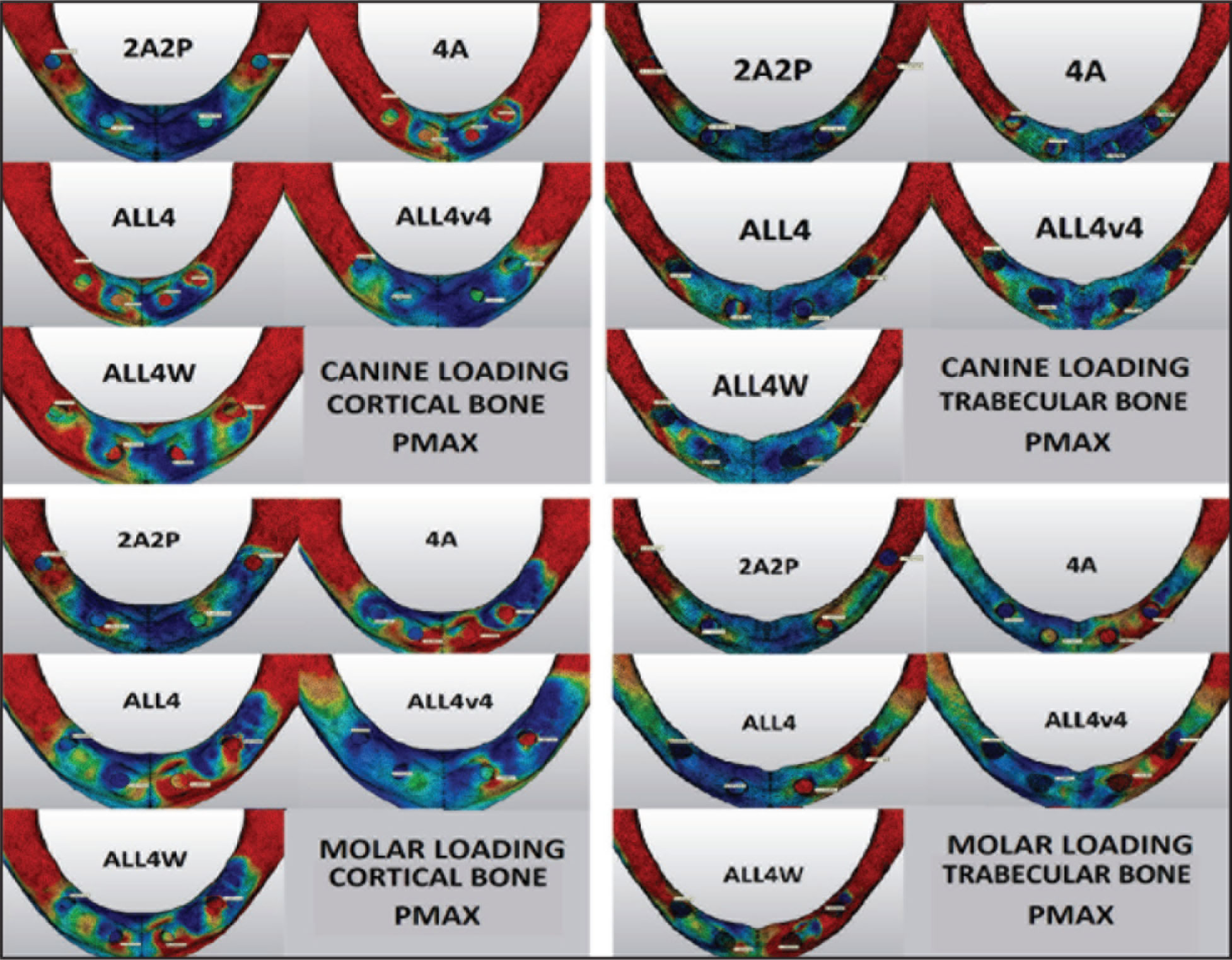
Numerical (MPa) and Graphical Comparison of Tension Stresses (Pmax) in the Cortical and Trabecular Bones Against Canine and Molar Loadings
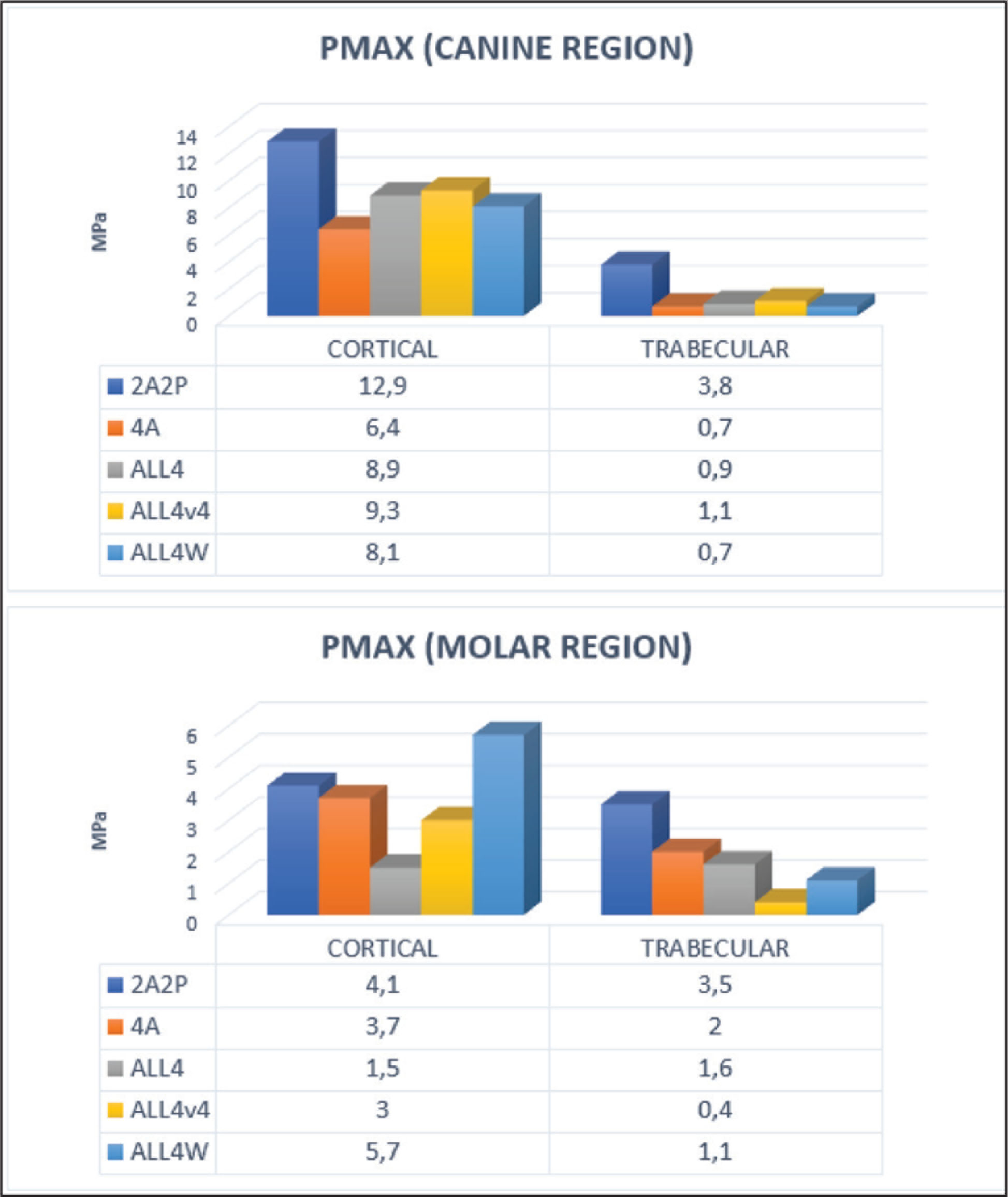
When stresses in the cortical bone were evaluated against the forces applied from the molar region, the highest stress of 5.7 MPa was observed in the ALL4W model, whereas the lowest stress of 1.5 MPa was observed in the ALL4 model. All models, other than the ALL4 model, produced 3 MPa more stress. The highest value in the trabecular bone was observed in the 2A2P model with 3.5 MPa. The ALLV4 model produced the lowest stress with 0.4 MPa, creating approximately one-third of the nearest stress value (Figures 3 and 4).
Minimum Principal Stresses
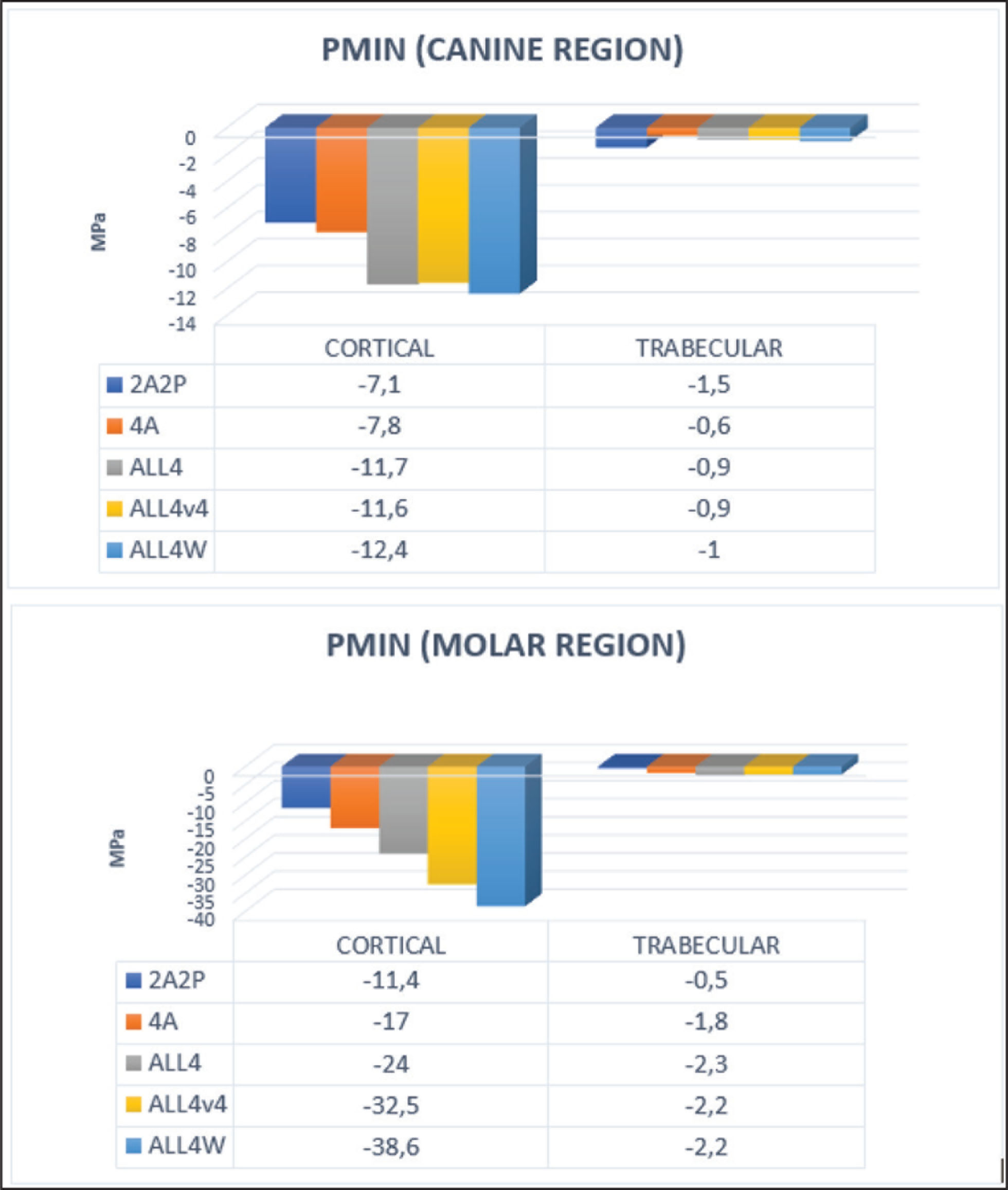
When stresses occurring in the cortical bone were evaluated against forces applied from the canine region, the highest stresses were observed in the three models that produced ALL4 variances with a mean value of –11.5 MPa. The lowest stress of –7.1 MPa was observed in the 2A2P model. In the trabecular bone, the highest stress of –1.8 MPa was observed in the ALL4W model, and the lowest stress of –0.6 MPa was observed in the 4A model (Figures 5 and 6).
When stresses in the cortical bone were evaluated against forces applied from the molar region, the highest stress of –38.6 MPa was observed in the ALL4W model, whereas the lowest stress of –11.4 MPa was observed in the 2A2P model. The three models of ALL4 variance presented higher stresses up to three times than that of the 2A2P model without a cantilever extension at the posterior region. In the trabecular bone, the highest stresses of –2.2 MPa were observed in three of ALL4 variance models, whereas the lowest stress of –0.5 MPa was observed in the 2A2P model (Figures 5 and 6).
Compression Stresses (Pmin) in the Cortical and Trabecular Bones Against Loadings from the Canine and Molar Regions
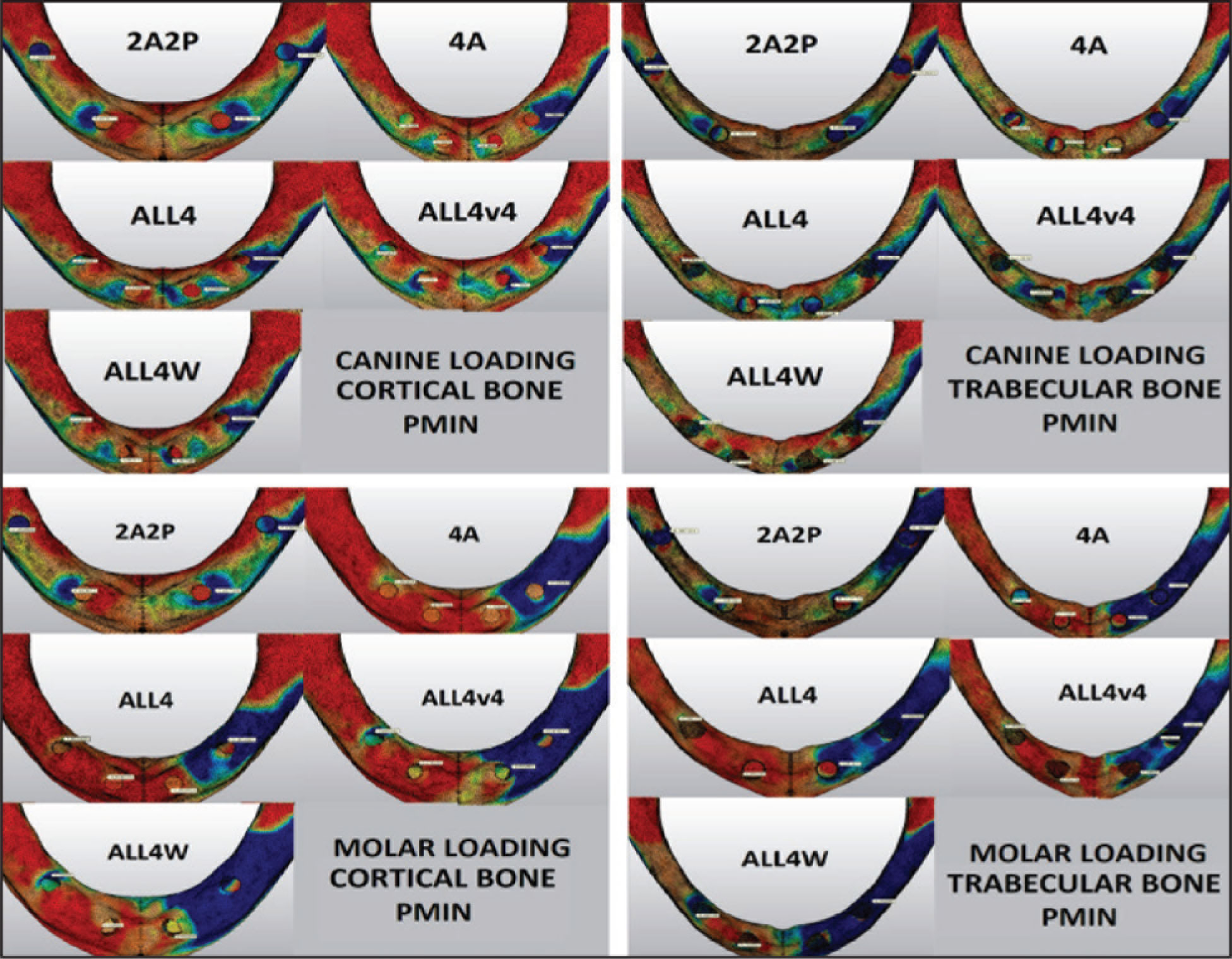
Numerical (MPa) and Graphical Comparison of Compression Stresses (Pmin) in the Cortical and Trabecular Bones Against Loadings from the Canine and Molar Regions
Stresses in Implants (Von Mises Stresses)
When stresses on the implants, as a result of the forces applied from the canine region, were evaluated, the lowest stress 17.5 MPa was observed in the ALL4v4 model, and the highest stress of 35.5 MPa was measured in the ALL4 model. The other three models presented similar stress values (Figures 7 and 8).
Von Mises Stresses on the Implants in Models Against Loadings from the Canine and Molar Regions
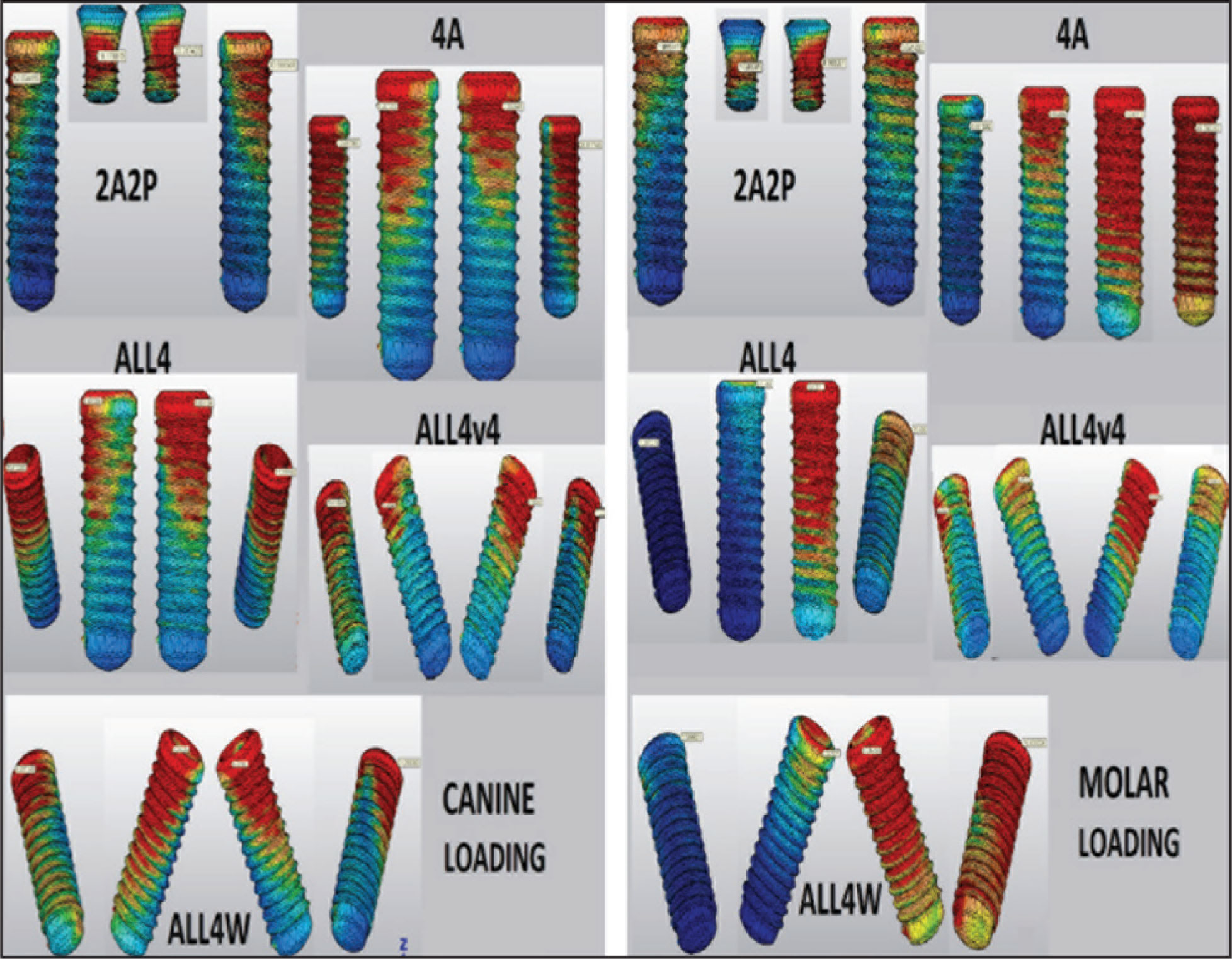
Von Mises Stresses (MPa) in Implants Against Loadings from the Canine and Molar Regions
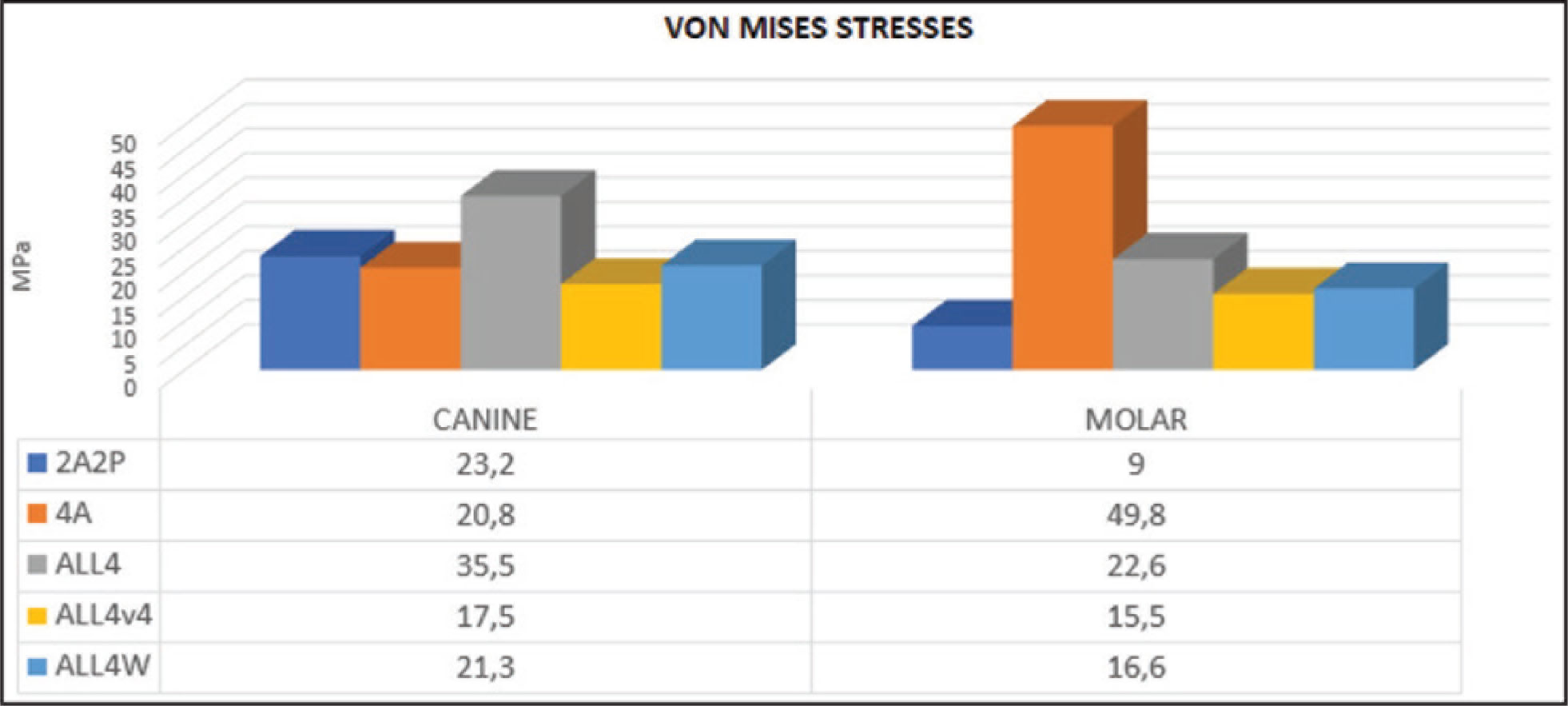
Against forces applied from the molar region, the highest stress was observed in the 4A model with a twofold difference compared to the closest model having 49 MPa stress, and the lowest stress of 9 MPa was found in the 2A2P model with no cantilever extension. In ALL4 variance models, stresses were observed to vary between 16 and 22 MPa (Figures 7 and 8).
Discussion
The classical ALL4 configuration showed a more balanced stress distribution than the other models in the study. Short implant support in the posterior region provided a more balanced stress distribution by reducing the stresses on implants via forces applied from the molar region, as expected. However, it could not achieve the desired results, mainly due to the high Pmax (tension) stresses on the bones. Of ALL4 variants, the ALL4W model, in which implants were opposed to each other, caused high stress, particularly on cortical bones. The ALL4v4 model, another variant of the ALL4 model, stands out as a good alternative to the ALL4 model, apart from the high-stress formation in the cortical bone against forces from the canine site. The 4A model, which includes four axially placed implants, was found to be the best alternative at the third place, except for the twofold stress occurring against molar region forces on implants, when compared to the closest model.
Finite element analysis is a method to investigate the stress values on complex structures. Under normal conditions, stresses arising from loading are impossible to visualize clinically. However, 3D finite element analysis makes it possible to examine stresses around dental implants and bones three dimensionally and provides an insight into the mechanical resistance under loading conditions. Knowing and understanding the biomechanical characteristics with studies of this type could help improve their characteristics in order to have more predictable oral rehabilitations.14–16
In recent years, the most trending technique for fixed implant-supported rehabilitation of completely edentulous mandible is the placement of four implants in different configurations. Full-arch fixed mandibular prosthetics supported by fewer implants are still skeptical. 17 Considering these conditions, the present study compared the rehabilitation options for completely edentulous mandible using four implants in different configurations.
One of Branemark’s recommended applications for the use of osseointegrated dental implants in the rehabilitation of atrophic and completely edentulous jaws in the posterior region is the placement of four axial implants in the interforaminal area of the edentulous jaw and the use of prosthetic cantilevers. 5 Although the success rates reported for this technique are high,18–20 a very long size of cantilever in these applications may cause various technical complications, especially on prosthetic materials.21–23 Due to such factors, distal-angled implant placement has been studied over recent years to allow more posterior positioning of the implants to benefit from the interforaminal space and reduce the length of the cantilever.6,21,24 The ALL4 treatment concept was proposed by Malo et al. 6 to be used in the fixed prosthetic rehabilitation of completely edentulous jaws. Following the reports of long-term data published by Malo et al., 24 other authors confirmed the high success rates associated with the use of this protocol. The tilted placement of distal implants has been proposed to provide numerous biomechanical and clinical advantages for fixed restorations with less invasive techniques than conventional axial implants and grafting procedures.11,24–27
After the ALL4 concept gained popularity, Jensen et al. 7 proposed some modifications to this concept for severely atrophic mandibles. In the modified technique, known as ALL4v4, the researchers replaced the two anterior axially placed implants in the original concept, as tilted and parallel to the posterior tilted implants. The researchers emphasized that the advantages of this modified technique included reduced fracture risk in atrophic mandibles, higher insertion torque values, ability to place longer implants, in addition to the maintenance of all advantages of the standard ALL4 concept prosthesis. They also emphasized that the implant locations and distributions in the ALL4v4 technique have very suitable biomechanical properties. In the present study, the original ALL4 concept (ALL4 model) of Malo et al., 6 as well as the “All-on-4-v-4 technique” (ALL4v4 model) of Jensen et al. 7 and a modification of them, in which the implants are tilted opposite to each other (ALL4W), have been illustrated. The present study found that ALL4 gives the most balanced results in terms of stress distributions, whereas the ALL4v4 model is a good alternative, giving results close to ALL4. The ALL4W model caused higher stresses on cortical bones than other variations in terms of the stress distribution.
Despite the success of the ALL4 technique, some studies reported that the same results could also be achieved with the axial placement of the same number of implants. Krennmair et al. 28 reported that there was no statistically significant difference in terms of the success of the implants and prostheses after a three-year follow-up period, between the four implant-supported full-arch mandibular fixed prostheses in which the posterior implants were tilted or placed axially. The researchers stated that the axial placement of the implants might be advantageous as the use of four axial implants provides the same success and, therefore, eliminates the need for angled abutments and different fittings that have to be used in tilted implant placements, thereby reducing the costs. In our study, the stresses in the 4A model, especially on the implants against the forces exerted by the molar region, were twofold higher than the closest model. In other situations, the 4A model caused average stress so that it can be considered at the third place after the ALL4 and ALL4v4 techniques, in terms of reducing the costs as highlighted by Krennmair et al. 28
Nowadays, the expectations of the patients and clinicians from a treatment plan include conservative treatment and reduced treatment time. Many studies have suggested that this goal can be achieved with short implants. Various studies have emphasized that short implants can be a good alternative to longer implants in cases which require additional augmentation procedures.3,4 The worst possible scenario was envisaged in the present study to allow implant placement in the posterior mandibular region, and the shortest implants available in the market, having a diameter of 4.1 mm and a length of 4 mm, were used for extra-short implants. Yet, current information about 4 mm extra-short implants is sparse in the literature.8,9 Passaretti et al. 29 rehabilitated an edentulous mandible using a fixed prosthesis supported by four extra-short implants measuring only 5 mm in length. The canine and firstmolar tooth regions chosen by Passaretti et al. 29 for implant placement were the same as the implant distributions in the 2A2P model, which utilizes an extra-short implant in the present study.
Ogawa et al. 30 established in their biomechanical study that supporting prosthetic rehabilitations with a cantilever in the mandible having short implants in the posterior region produced better stress values against axial and oblique forces than the prostheses with no posterior implants, and they argued that cantilever extensions should be supported with extra-short implants in the posterior region.
In the 2A2P model used in the present study, predictably, even though the posterior extra-short implants were able to reduce and compensate the stresses caused by the cantilever extensions, especially at the posterior sites by eliminating the moment of forces, it was not able to achieve the same success in bones. In most cases, higher stresses were experienced on bones. However, the effects of support on four implants placed in the interforaminal region with extra-short implants in the posterior region can be investigated in future biomechanical or clinical studies.
Conclusions
Among the four implant-supported full-arch fixed rehabilitation alternatives for a completely edentulous mandible, the classic ALL4 and the ALL4v4 techniques were observed to be the most successful treatment options. On the other hand, the use of extra-short implants in the posterior region, for the elimination of cantilever extension, was decided to be the last method of choice among all the techniques compared in this study. This was because of the high stresses on bones in most conditions, even though it balances the forces on the implants against the forces applied from the molar region.
The results of the present study support that the tilted placement of the implants provides an advantage for stress distributions biomechanically. As the direction of the tilting, the distal direction gave better results. On the other hand, although the use of extra-short implants provided the predicted support by eliminating the cantilever extensions, it was insufficient to form the posterior support of a prosthesis with only four implants. In future studies, it will be useful to investigate the contribution of the extra-short implants to the prosthesis supported by more implants.
Author Contributions
SK and HCT both are equally responsible for conceptualization, data curation, investigation, methodology, project administration, resources, and validation. SK single-handedly managed formal analysis, funding acquisition, software, visualization, and original draft. HCT single-handedly managed supervision and review and editing.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.