
Abstract
Objectives:
To gather information about current practices and assess the opinions, preferences, and clinical knowledge of surgeons who perform alveolar bone grafts. In addition, surgical training differences in correlation to techniques and outcomes are evaluated.
Methods:
A survey with both multiple choice and narrative answers regarding surgeons’ practices for alveolar bone grafting was designed and sent via email to members of the American Cleft Palate/Craniofacial Association (ACPA) identified as general craniofacial or oral maxillofacial surgeons. Responses were collected via an anonymous online survey tool.
Participants:
Members (336) of ACPA identified as craniofacial or oral-maxillofacial surgeons were contacted, and 62 responses were recorded.
Results:
The majority of survey respondents were oral-maxillofacial surgeons in practice for more than 15 years. 98.4% of respondents had used iliac crest and at least one additional source for grafting, while only 52.7% had performed grafting using recombinant bone morphogenetic protein (RhBMP). 82% used cone beam CT as their evaluation of choice for graft assessment and the majority (62.9%) waited more than 8 weeks postoperatively to image. Chi-square analysis demonstrated significantly longer time in practice for practitioners without craniofacial fellowship training.
Conclusions:
The results of this study demonstrate that there remains significant variation in alveolar bone grafting practices among surgeons. While some consensus exists, new innovations and technologies will require continued evaluation of surgical practices and outcomes. Long-term follow-up studies are needed especially with regard to the use of RhBMP in alveolar clefts.
Introduction
Alveolar bone grafting is a well-established procedure and a crucial step in the treatment of children with cleft lip and palate.1-5 This procedure, which also involves the closure of any fistulas when present in order to obtain a watertight compartment, successfully establishes bone continuity in the alveolus, stabilizes the maxillary arch, and allows for the eventual eruption of permanent teeth in the cleft.1,5-7 While historically there have been different options for the timing of this procedure (either a primary bone graft in infancy or a secondary bone graft during mixed dentition), today the vast majority of cases are performed as a secondary bone graft.
The historical standard of care in alveolar bone grafts (ABG) has been to use anterior iliac crest bone as the donor graft due to its large supply of cortico-cancellous bone and well-documented success rate of 60% to 80%2-4,7,8 However, one significant drawback to autologous bone grafts from the iliac crest is the associated donor-site morbidity, with complications including increased risk for postoperative pain, infection, sensory disturbances, ambulatory difficulties, and the very rare pelvic fracture.1-4,9,10 While other sources of autologous bone including mandibular and calvarial bones have been described in the literature, studies have demonstrated inferior outcomes with the calvarial bone when compared to the iliac crest bone. 9 Mandibular grafts have demonstrated similar outcomes to the iliac crest, but the limited amount of bone obtained from this donor site precludes its use in larger alveolar clefts.11,12 Much research has been done to find alternative graft sources that are similarly successful to autologous grafts but without the donor-site morbidity.
One promising non-autologous graft source is recombinant human bone morphogenetic protein-2 (RhBMP-2) used in combination with an osteoconductive substrate. RhBMP-2 is an endogenous protein member of the transforming growth factor beta (TGF-B) superfamily.2,7,13,14 It is naturally found in high levels in embryogenic and skeletogenic tissues during development and is also produced in minute quantities in mature bones for use in bone repair and maintenance. When given at super-physiologic levels (roughly 2 ×10 5 times the naturally occurring levels of BMP-2), RhBMP-2 has been shown to be a potent inducer of de novo bone morphogenesis.3,6 Recent studies have shown that RhBMP-2, when coupled with an osteo-conductive base like material such as a demineralized bone matrix, has similar success rates for ABG as compared to those of autologous bone grafts without the associated donor-site morbidity.2,4,13 While RhBMP-2 use currently has a limited range of clinical indications due to the lack of sufficient data and potential safety concerns, it remains one of the most promising future alternatives for alveolar bone grafting.5,7,10,15
While generally accepted that secondary bone grafting should be performed before the eruption of the canine, there is still significant variation among surgeons with regard to the exact timing, surgical sequence, graft source, and donor site selection that should be used for ABG. Emerging alternative non-autologous graft sources like RhBMP-2 and the presence of a surgeon workforce with varied backgrounds and levels of experience have led to a wide range in clinical approaches to perform ABG. No studies have been performed that explore these differences in practice and preferences among a wide group of practitioners. The purpose of this project is to gather information about current practices as well as assess the opinions, preferences, and clinical knowledge of surgeons who perform ABG as well as evaluate the differences in surgical training in correlation to techniques and outcomes.
Methods
A survey with both multiple choice and narrative answers regarding surgeon’s practices for alveolar bone grafting was designed (Appendix A). And an approval was obtained from University of California, Irvine Institutional Review Board. The survey was sent via email to a total of 336 members of the American Cleft Palate/Craniofacial Association (ACPA), identified as general craniofacial or oral maxillofacial surgeons who had opted in to receive emails from the association’s listserv. Responses were collected for a period of one month with an anonymous online survey tool (
Results
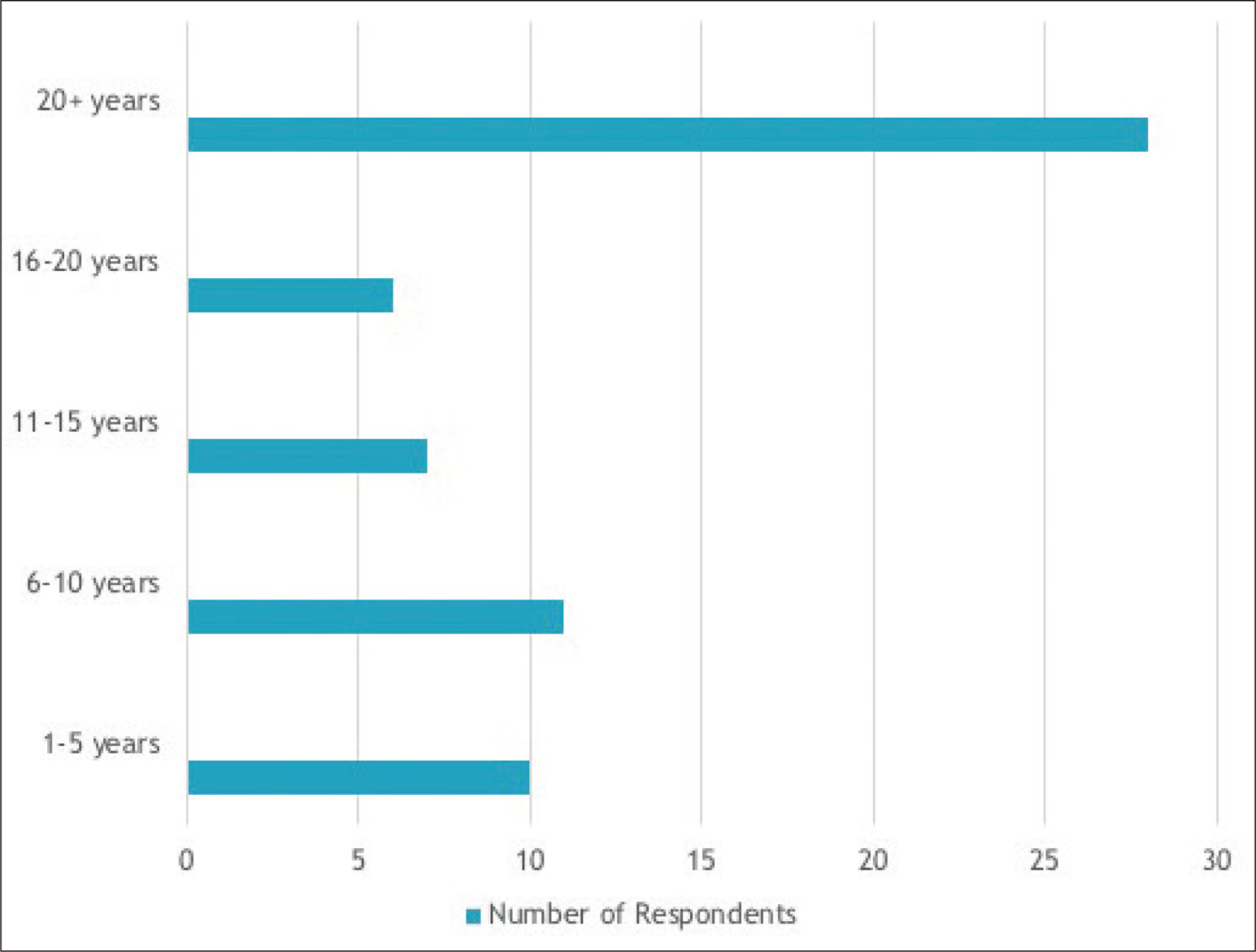
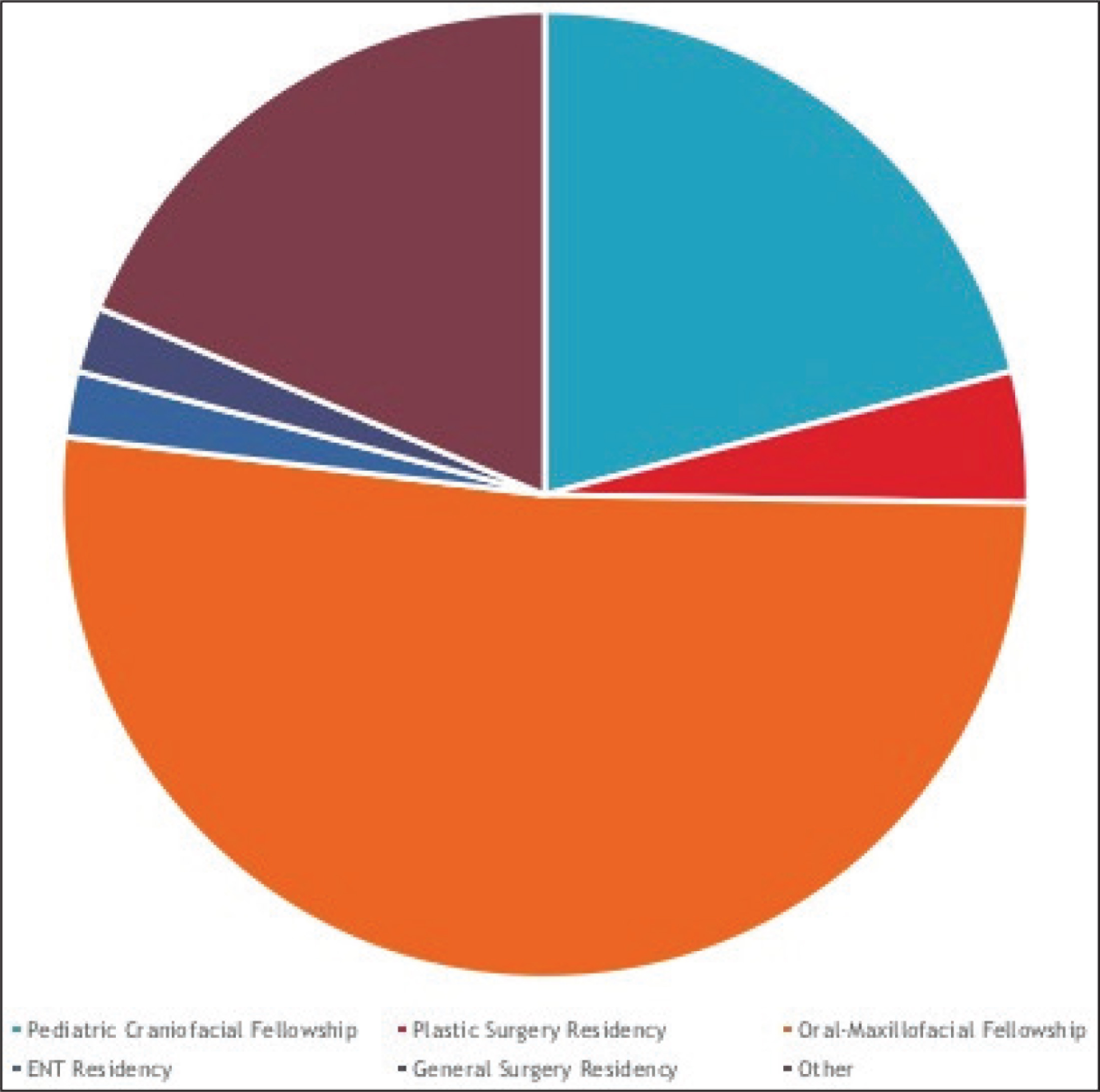
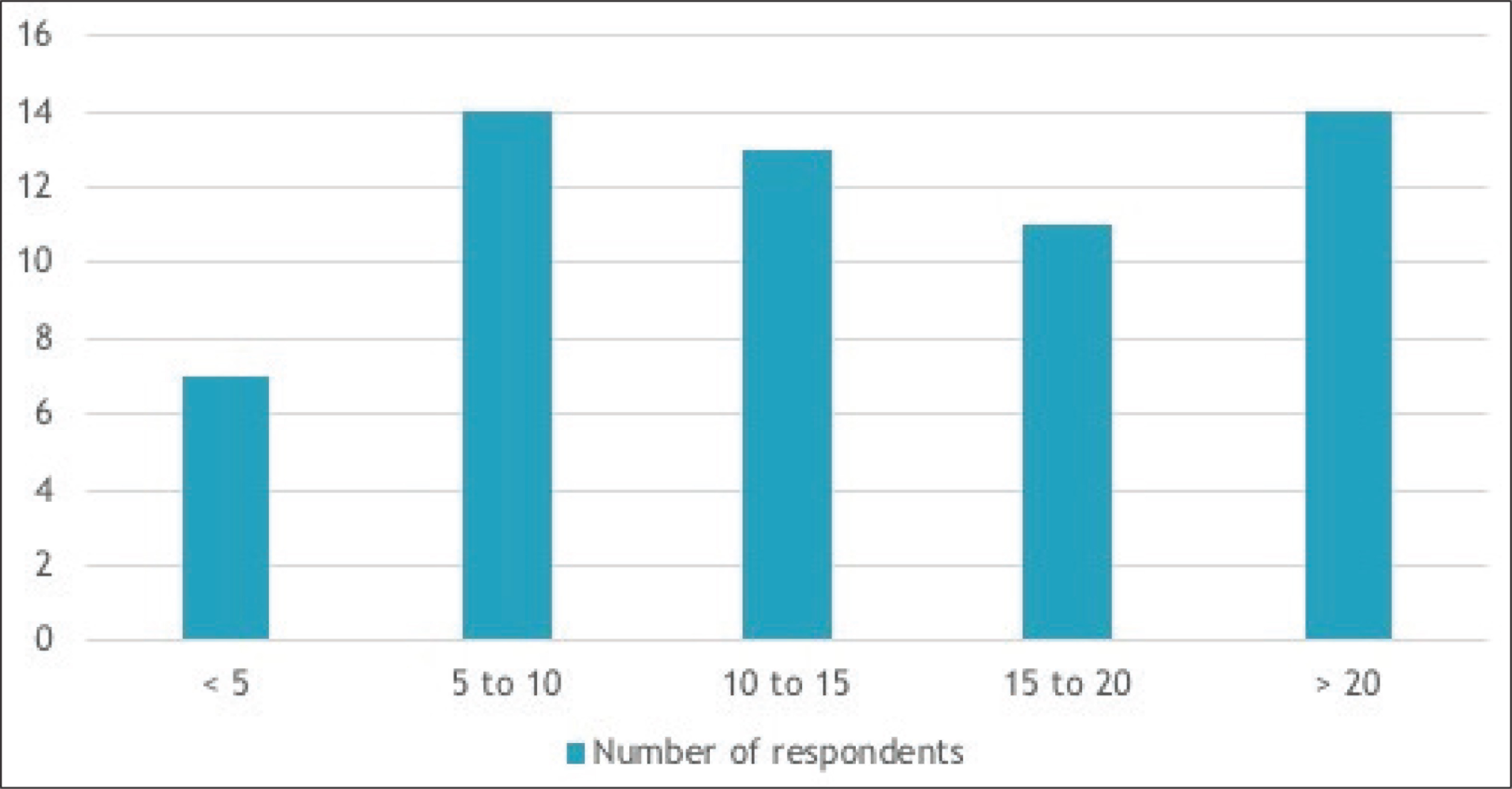
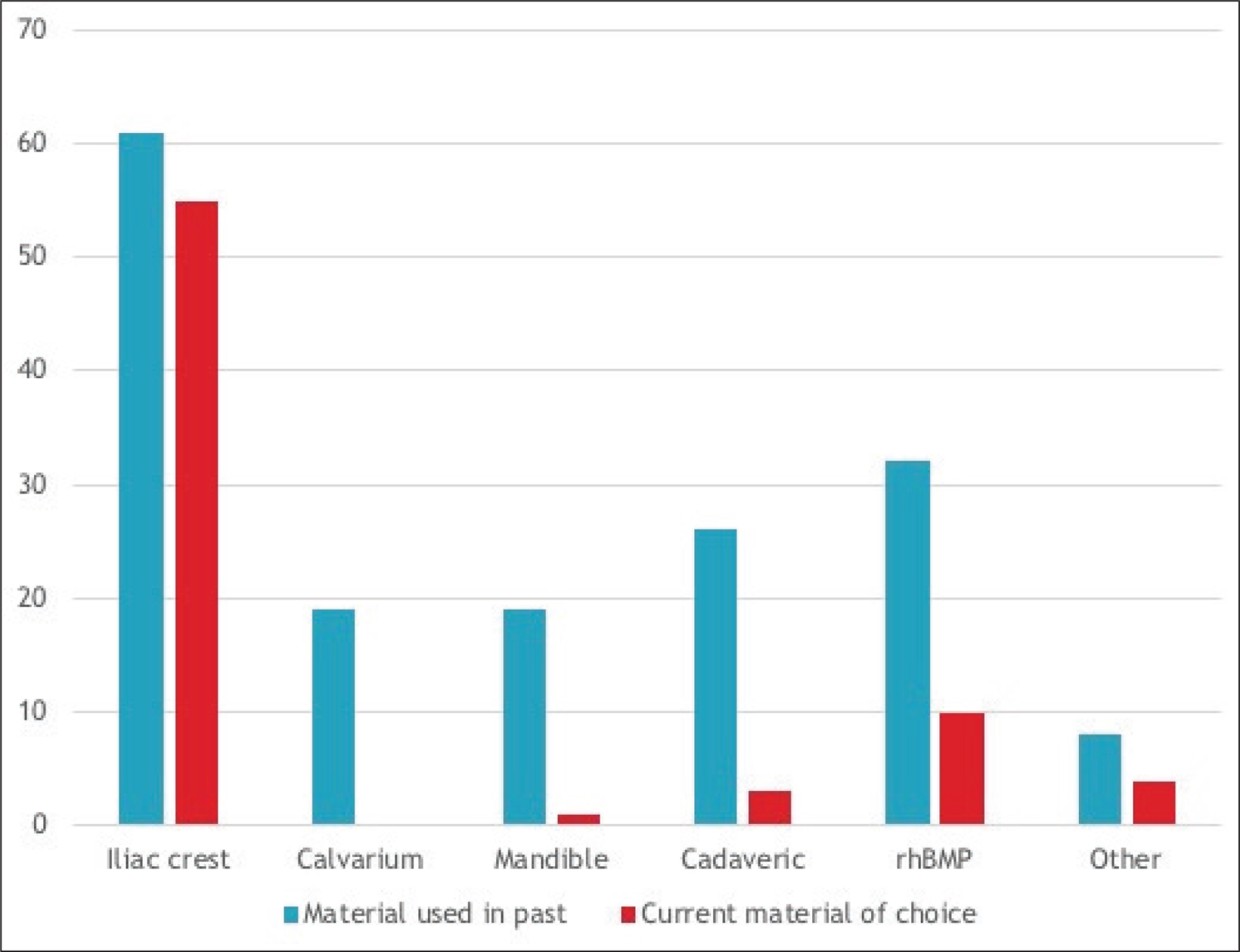
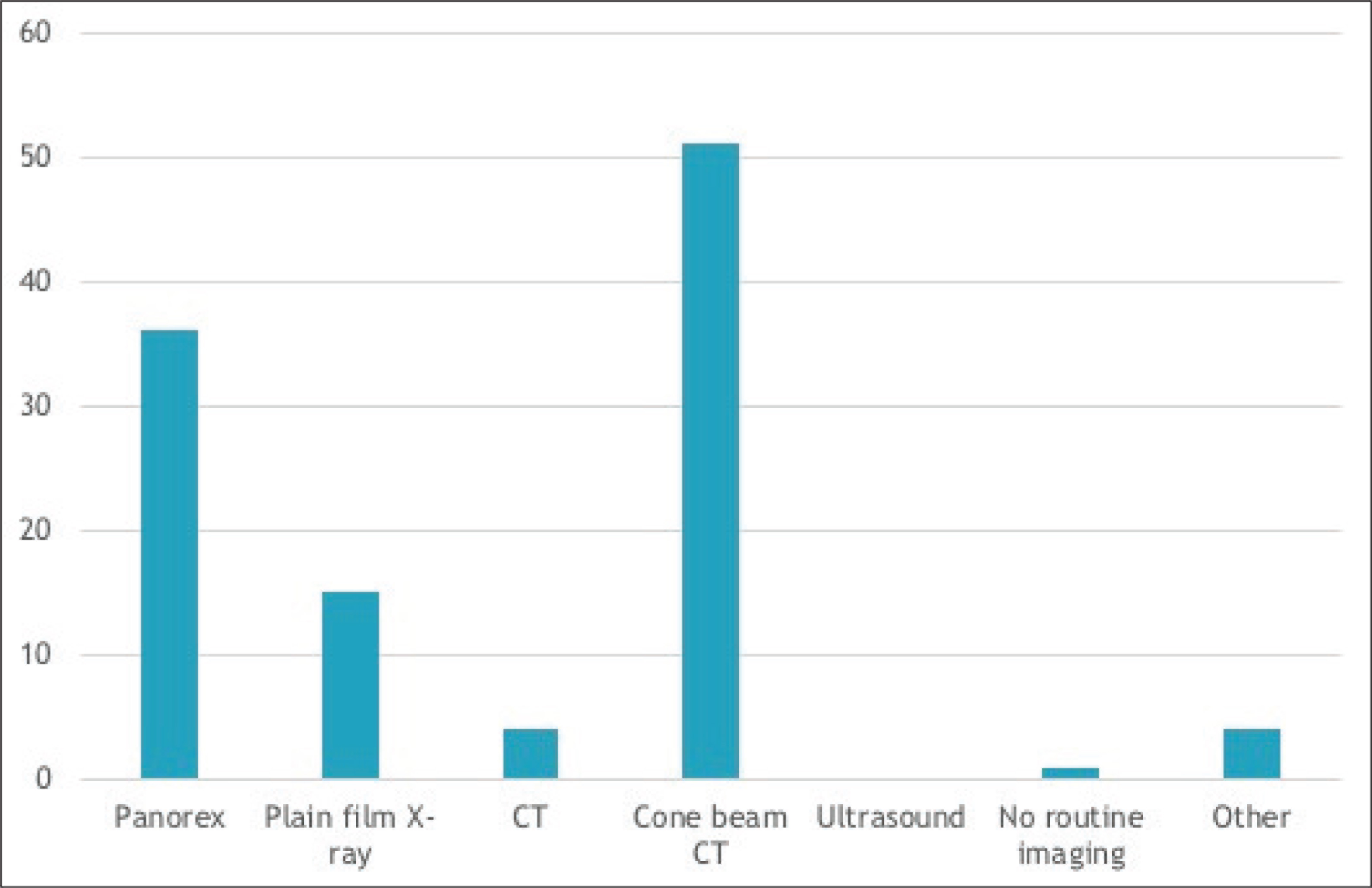
62 survey responses (18.5%) were received. Of the respondents, the majority were oral-maxillofacial surgeons in practice for more than 15 years (Figure 1); 30% had completed a Pediatric/Craniofacial Surgery fellowship (Figure 2); 61.29% of the respondents reported that they perform 10 or more bone grafts per year (Figure 3); 98.4% of the respondents had used iliac crest and at least one additional source (mandible, calvarial, RhBMP, or cadaeric bone) for grafting (Figure 4); 52.7% had performed grafting using RhBMP at some point, but only 16.1% identified it as their current material of choice and 9% reported intention to use it for grafting in the future. Some commonly cited concerns with RhBMP included the lack of approval from Food and Drug Administration (FDA) to use it in case of children, the cost, and the complications including swelling, flap loss, and the perceived quality of bone. With regard to the timing of bone grafting, 6.5% respondents performed grafting before age of mixed dentition, 32.3% performed it at the time of mixed dentition, and 43.6% performed it prior to the eruption of the canines. 82% used cone beam CT (CBCT) as their evaluation of choice for graft assessment and the majority (62.9%) waited more than 8 weeks postoperatively to image (Figure 5). The eruption of canines through the graft was the most commonly cited marker of success. Chi-square analysis demonstrated significantly longer time in practice for practitioners without craniofacial fellowship training (Table 1)
Chi Square Analysis

Discussion
The results of this survey demonstrate the continued variation in alveolar bone grafting practices among craniofacial surgeons.
In regard to graft material of choice, the iliac crest was considered the “gold standard” by a vast majority of respondents due to its ease of availability, minimal morbidity, and proven success record. While 52.7% of practitioners had worked with RhBMP at least once, its use elicited most controversies among respondents. Those with concerns mainly cited the lack of FDA’s approval to use it in treatment of children, the cost, some complications, and the perceived quality of the bone. The proponents of the use of RhBMP or other materials noted early discharge and return to activities, the ability to perform surgery as an outpatient procedure, and minimal invasiveness. Further more, some opponents to RhBMP cited their prior trainings solely with iliac crest grafts as the reason for its lack of use. This suggests both the continued need for the further evaluation of the use of RhBMP for initial alveolar bone grafting in this population and the incorporation of different graft sources into training programs.
Early secondary bone grafting (prior to the eruption of the canine) was practiced by 43.6% of respondents. The rationale cited in the survey for this timing included to provide bone stock for canine eruption as well as to stabilize the bicuspid and incisor abutting the cleft. Palatal expansion may either be performed before grafting or after the graft has healed. The pre-expansion alveolar cleft has a smaller soft tissue and bone defect, and studies have shown that expansion can be successfully performed after grafting.16,17 Expansion also provides postgraft stimulation that may encourage maturity and decrease resorption of the bone graft. 18
When comparing surgeons with and without craniofacial training, there were no significant differences in practice including the number of ABG performed in the past year, the use of RhBMP, the preferred grafting material, or the timing of imaging after grafting between the two groups. Statistical analysis did indicate that surgeons in practice for more time were less likely to have completed a craniofacial fellowship, suggesting a trend toward more specialization in newer surgeons. Given the imminent projected changes to the US physician workforce over the coming years, the combination of increased specialization and advances in knowledge regarding relatively new materials like RhBMP may lead to alterations in surgical management that warrants further follow up.
The trend of increasing the use of CBCT to monitor graft success demonstrated in the survey data is another interesting finding. The significantly lower doses of radiation, higher image resolution, and the cost of ownership compared to conventional CT have made CBCT a standard for dental and maxillofacial procedures. 19 CBCT has been used to assess the preoperative volume of the cleft defect as well as the postoperative bone volume and support of dental implants after placement.20,21 As the rates of imaging with this modality increase, earlier detection of insufficient grafts may result in changes in management or allow more informed counseling for parents and patients regarding the potential need for additional grafting procedures.
We acknowledge multiple limitations to this study. Our results were limited by a small sample size as well as self-reporting of data from surgeons, which may lead to bias with regard to the data collected on outcomes. In addition, there is an inherent self-selection bias that was present due to the voluntary nature of the survey. Lastly, given the wording of some of our questions, there may have be ambiguities in our open-ended questions that limit the survey’s external validity.
Conclusion
The results of this study demonstrate that there remains significant variation in alveolar bone grafting practices among surgeons. While some consensus exists, for example the iliac crest bone as the “gold standard” donor material, new innovations and technologies will require continued evaluation of surgical practices and outcomes. Long-term follow-up studies are needed especially with regard to the use of RhBMP in alveolar clefts.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Survey Questionnaire
MD/DO
DMD/DDS
Other (Please specify in blank below.)
Pediatric Craniofacial Fellowship
Plastic surgery residency
Oral-maxillofacial fellowship
ENT residency
General surgery residency
Other (Please specify in blank below.)
1-5years
6-10yrs
11-15yrs
15-20yrs
>20yrs
Plastic surgery, general practice, both adult and pediatric patient population
Pediatric craniofacial surgery
Pediatric otorhinolaryngology
Oral and maxillofacial surgery
Other (Please specify in blank below.)
<5
5-10
10-20
>20
<5
5-10
10-15
15-20
>20
Iliac crest
Calvarium
Mandible
Cadaveric
rBMP
Other (Please specify in blank below.)
Iliac crest
Iliac crest
Calvarium
Mandible
Cadaveric
rBMP
Other (Please specify in blank below.)
Yes
No
At time of palate repair
Before age of mixed dentition
At the age of mixed dentition
Before eruption of canines
After the eruption of canines
No preference
Panorex
Plain film XR
CT
Cone-beam CT
Ultrasound
Other (Please specify in blank below.)
<40%
40-60%
60-80%
>80%
<40%
40-60%
60-80%
>80%
<40%
40-60%
60-80%
>80%
<40%
40-60%
60-80%
>80%
2weeks or less
2-4weeks
4-6weeks
6-8weeks
>8weeks
Bergland
Witherow
Long
None
Other (Please specify in blank below.)
2 weeks
4 weeks
6 weeks
8 weeks
Other (Please specify in blank below.)
2 weeks
4 weeks
6 weeks
8 weeks
Other (Please specify in blank below.)