
Abstract
Objectives:
Optimal restoration of endodontically treated teeth is very important for the durability of the endodontic treatment. The focus of this study was to evaluate the fracture strength and microleakage of composite endocrowns compared with Class II composite restorations in endodontically treated primary molar teeth.
Materials and Methods:
48 extracted second primary molars were divided into 2 groups. Group 1 (control): teeth with Class II and endodontic access cavities restored with G-aenial composite; group 2: endocrown restorations with G-aenial composite. After completing restorative procedures, teeth were subjected to thermal cycling (500 cycles). Compressive loading was applied to half of the samples, although the other half were immersed in 0.5% basic fucsin solution for 24 h, sectioned, and examined for dye penetration under stereomicroscope. Data were subjected to statistical analysis by the Mann-Whitney U test (α = 0.05).
Results:
The fracture strength of endocrowns (1741 ± 379.35 N) was significantly higher than that of the control group (1126.5 ± 405.39 N) (P < .05). No statistical difference was found in microleakage between the 2 groups (P > .05).
Conclusion:
Endocrown preparation increases the fracture strength of the final composite restoration when used in primary molar teeth. Composite endocrown restorations can be a practical and an esthetic option for restoring endodontically treated primary molar teeth.
Introduction
The restoration of mutilated, endodontically treated primary teeth with a suitable material is very important for regaining function and esthetics for these teeth and ensuring durability of the endodontic treatment. Although stainless steel crowns (SSC) have been successfully used for this purpose since their introduction by Humphrey 1 in 1950, they are usually rejected by a child patient and sometimes by parents because of their unpleasing esthetics.
With the advancements in dental adhesive technologies and materials, indirect composite or ceramic restorations made by either inlay ovens or coronary artery disease (CAD)/ complementary and alternative medicine (CAM) systems have been widely used in recent years.2-6 These types of restorations are considered advantageous in pediatric dentistry as they decrease chairside time 7 and therefore increase the cooperation of children. Recently, the restoration of endodontically treated teeth with adhesive techniques has been advocated as adhesion ensures sufficient material retention without the need for aggressive macroretentive preparations. According to this concept, endocrown-type of restorations was suggested for posterior permanent teeth as an alternative to post and core retained ones.8-10
Endocrown restorations were first introduced by Bindl and Mörmann 11 in 1999. This monolithic type of restoration uses the pulp chamber as a central retention cavity and the adhesive resin cement for microretention. One of the advantages of these restorations is that the endocrown preparation is usually supragingival, keeping the restoration away from periodontium, which is considered beneficial for hygiene and periodontal health. Moreover, the conservation of peripheral enamel maintains the possibility to bond the margins of the future restoration to it. 12 The first endocrown restoration was milled from CAD/CAM porcelain blocks using the CEREC system. Later on, because of their high stress-absorbing properties, resin materials were also used in the fabrication of endocrowns.12-15 Composite restorations might be considered more practical in pediatric dentistry compared with the expensive porcelain restorations. Endocrown restorations were found to perform successfully in endodontically treated permanent molar teeth,11,16 while their use in premolars and anterior teeth is still controversial.16-18 According to our knowledge, this kind of restoration has never been used before in primary teeth; therefore, this study was planned to evaluate endocrown restorations, which can be an esthetic alternative to SSC in endodontically treated primary posterior teeth and in patients with metal allergy.
The aim of this study is to compare the endocrown preparations and Class II cavities associated with endodontic access openings both prepared in primary molar teeth, and to evaluate the effect of both preparations on the fracture strength and microleakage of the final composite restoration.
Materials and Methods
Ethics Committee’s Approval
This experimental research study was conducted by the Department of Pediatric Dentistry, Faculty of Dentistry, Atatürk University, approved by the Research Ethics Committee of Faculty of Dentistry (Ref nos. 10/2017 resolution #58) and in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Specimen Selection and Preparation
This study used a total of 48 primary second molars (24 upper and 24 lower), which were freshly extracted from human patients. All selected teeth had no caries on their buccal, palatal, and occlusal surfaces, were free of any developmental defects, had no visible cracks as a result of the extraction, and had not previously undergone any dental restoration.
The collected teeth were cleaned of soft-tissue debris using a periodontal scaler, immersed in 0.1% thymol solution for 24 h for disinfection, and then stored in saline solution until the cavity preparation was done. All specimens were embedded in cold-cured acrylic resin (Takilon, WP-Dental) up to 1 mm below the cementoenamel junction using standard plastic molds. Then, teeth were randomly divided into 2 groups with equal distribution of upper and lower teeth in each group as follows:
Group 1 (control): Class II cavities with endodontic access openings restored with GC direct G-aenial composite (n = 24). Group 2: Endocrown cavities restored with GC direct G-aenial composite (n = 24).
Tooth Preparation
Group 1 (Class II cavity with endodontic access opening)
Class II cavity preparation was made using inverted cone and fissure burs. For standardization, gingival wall was prepared 1 mm above the cementoenamel junction with 3 mm buccolingual width. After that, endodontic access cavity was opened, and the pulp chamber was cleaned of necrotic pulpal tissues. The walls of the pulp chamber were prepared with 6° to 8° angle divergence using tapered cylindrical diamond bur.
Group 2 (endocrown cavity preparation)
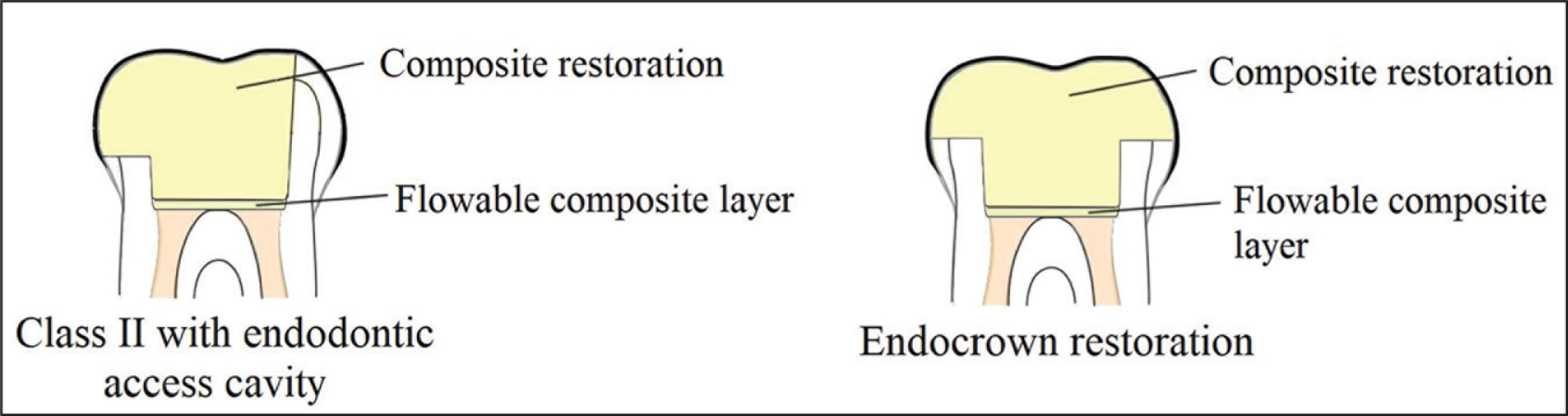
A diamond wheel bur was used to perform an occlusal reduction of 2.5 mm. To achieve a butt cervical margin, the bur was oriented along the major axis of the tooth and held parallel to the occlusal plane. Then, endodontic access cavity was prepared and the pulp chamber was cleaned of necrotic pulp tissues. Using tapered cylindrical diamond bur, the pulpal walls were prepared with 6° to 8° divergence toward the occlusal surface, and a 96° to 98° angle between the pulpal floor and pulpal walls was obtained. Internal angles were smoothened and rounded (Figure 1).
Diagrammatic Representation of Tooth Preparation and Restoration of the 2 Groups (Longitudinal Section)
Restoration of Teeth
After cavity preparation was completed, all canal orifices were covered with flowable composite (GrandioSO Flow, Voco) in order to obtain a straight pulpal floor.
Cavity walls were etched with 35% phosphoric acid gel (Vococid, Voco) by total etch technique (30 s for enamel and 15 s for dentin). After etching, cavities were rinsed with water, dried gently with air spray, and bonding agent (Futurabond U, Voco) was applied and cured with LED polymerizing unit (Woodpecker, Guilin Woodpecker Medical Instrument Co) for 10 s. Restorations were made using G-aenial composite (GC Corporation) with layering technique. Each layer had a maximum thickness of 2 mm and was cured with LED unit for 20 s. After completing the restoration, finishing and polishing was done using Sof-Lex (3M, ESPE) disks and rubber tips.
Thermocycling
All the teeth were stored in a humid environment at 37°C for 1 week. After that, teeth were subjected to 500 thermal cycles between 2 water baths of 5° and 55°C with a dwell time of 30 s at each temperature (MOD Dental, Esetron Mekatronik Ltd).
Fracture Strength Test
To perform fracture strength test, an Instron (Instron Corp) machine was used to apply compressive loading to the samples. A stainless steel bar with ø 36 mm was positioned so that it contacts both buccal and lingual cusps of the tested samples simultaneously. Loading was applied perpendicularly to the occlusal surface with a crosshead speed of 0.5 mm/min till failure occurred, which is represented by fracture of either the restoration or the tooth. The force required to cause fracture was recorded in Newtons (N).
Microleakage Test
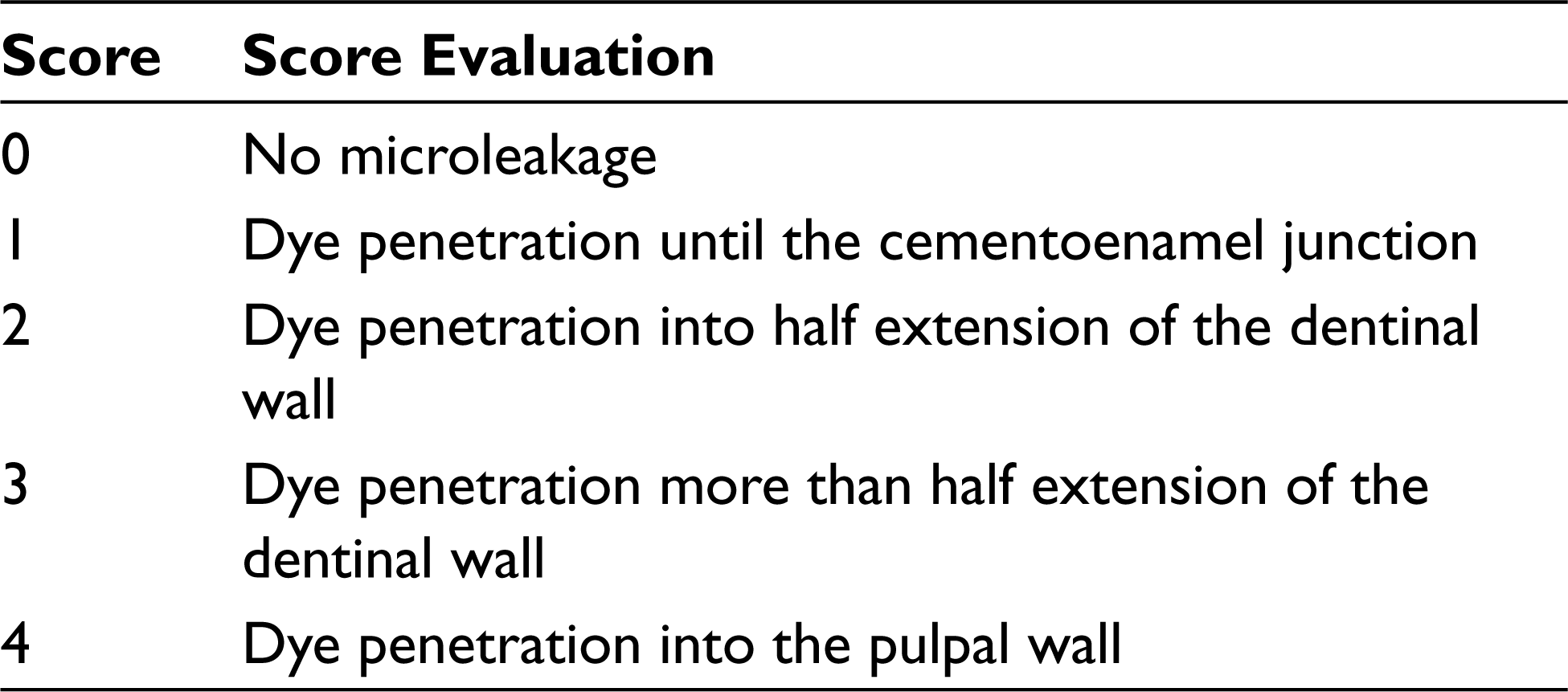
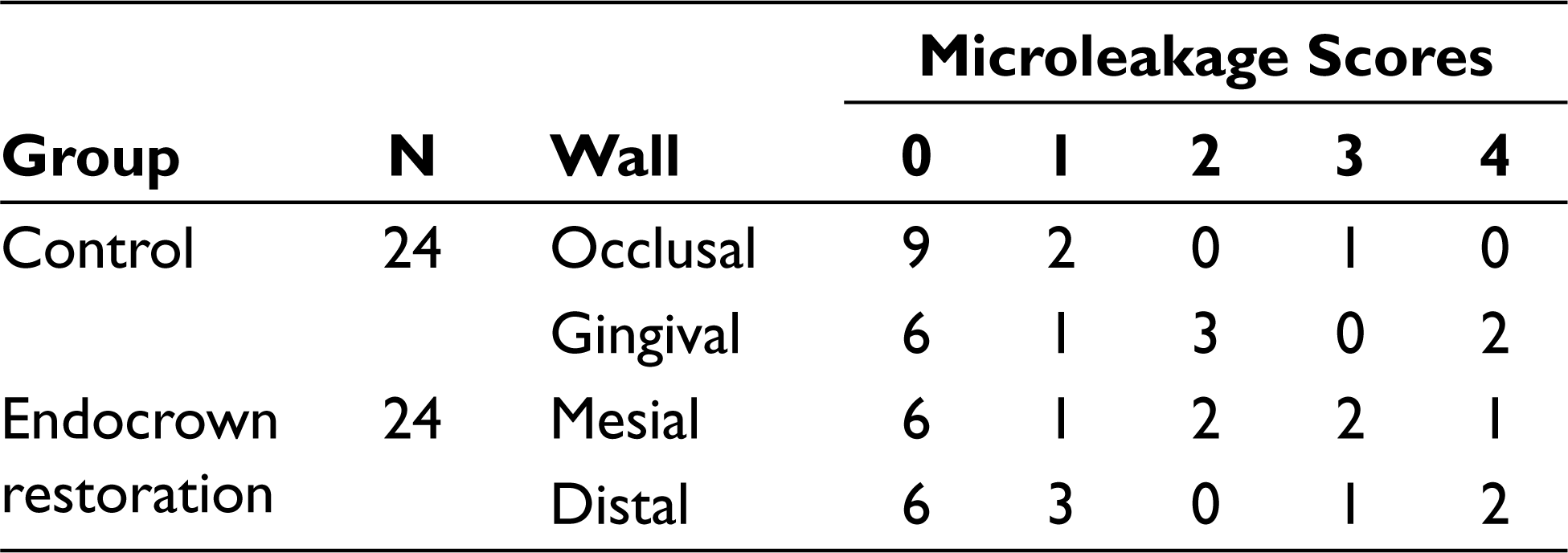
The specimens for this test were covered with 2 layers of nail polish except for 1 mm around the tooth-restoration interface and were embedded in a 0.5% basic fucsin solution at room temperature for 24 h. Teeth were taken out of the dye and washed with water. After that, specimens were sectioned in a mesiodistal direction with a low speed diamond saw using Isomet 1000 (Buehler) machine under water cooling. For the assessment of dye penetration, the sections were examined under stereomicroscope (Novex, Zoom Stereo RZ-Range), and photographs were taken using digital camera (Nikon Coolpix 4500, Nikon Corporation). For each sample, 2 scorings were taken. For Class II with an endodontic access opening group, dye penetration at the tooth/restoration was scored for occlusal and gingival walls, while for the endocrown group, it was scored for mesial and distal gingival walls. Table 1 shows the scoring system, using a scale from 0 to 4.
Microleakage Scoring Scale
Statistical Analysis
Values and scores obtained from the tests were submitted for statistical analysis by a nonparametric Mann-Whitney U test (α = .05) using IBM SPSS v20.0 software program.
Results
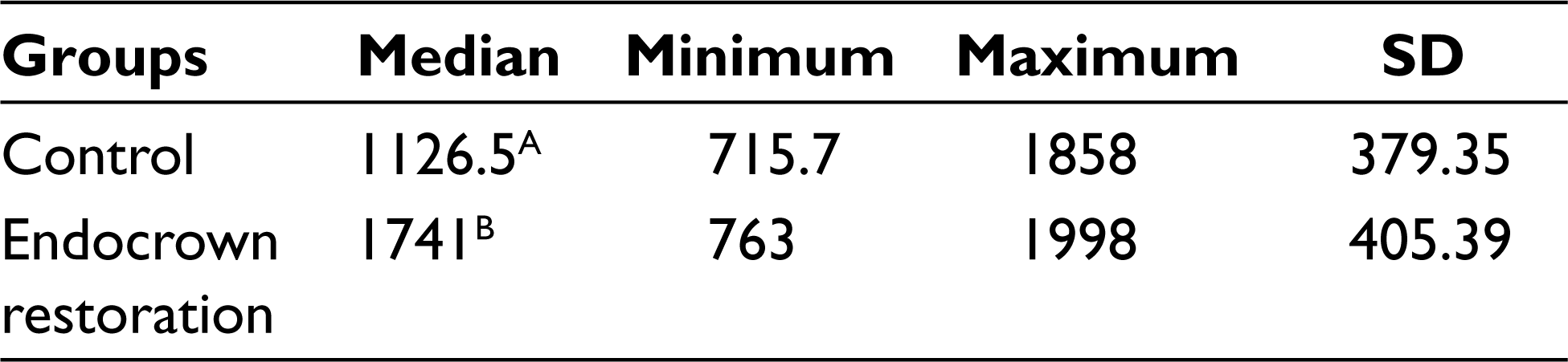
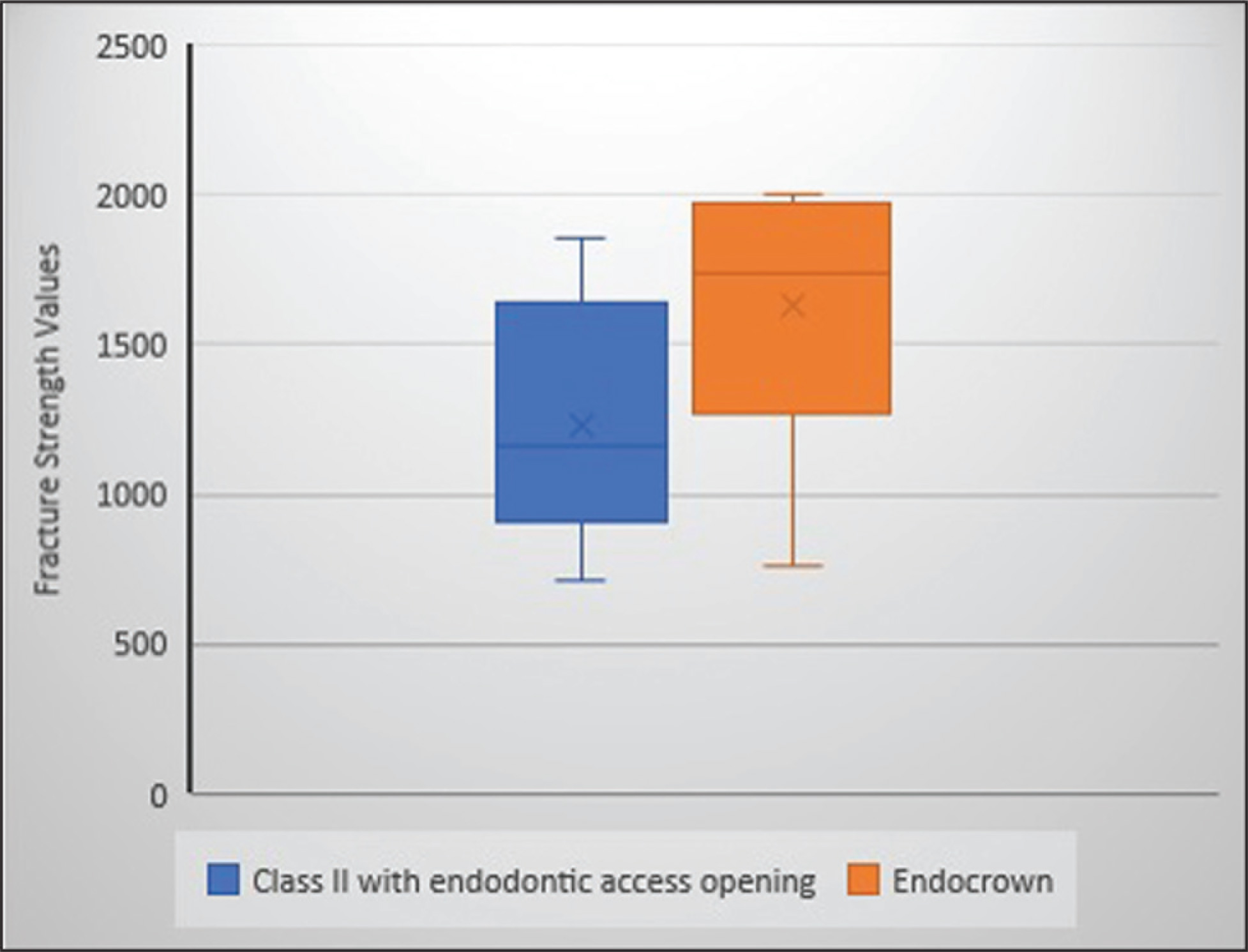
The median values, standard deviations, and the Mann-Whitney U test results from fracture strength test are presented in Table 2 and graphically drawn (Figure 2).
Comparison of the Fracture Strength Results Between the Groups
Box-Plot Showing Fracture Strength Results of the Groups
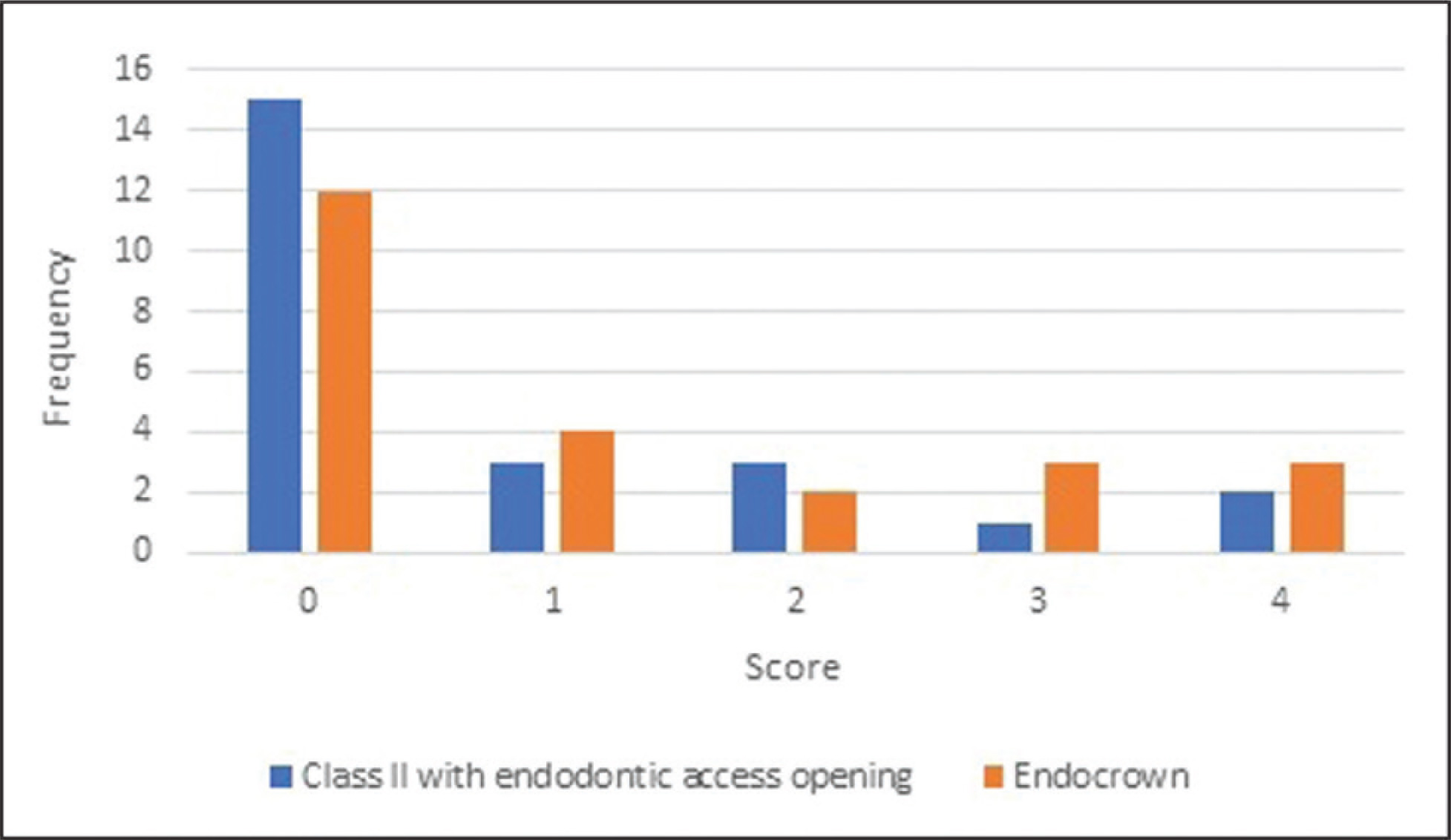
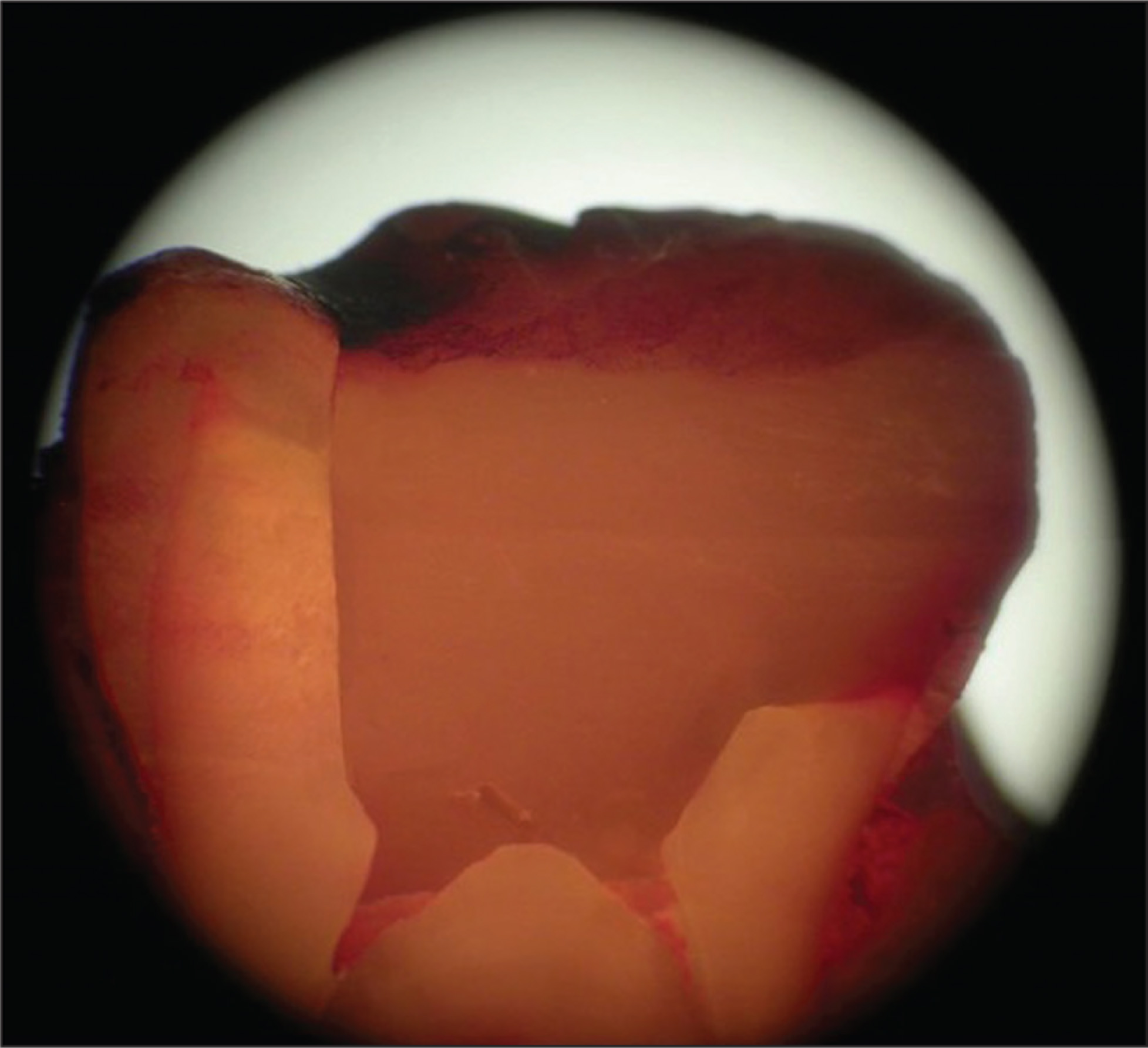
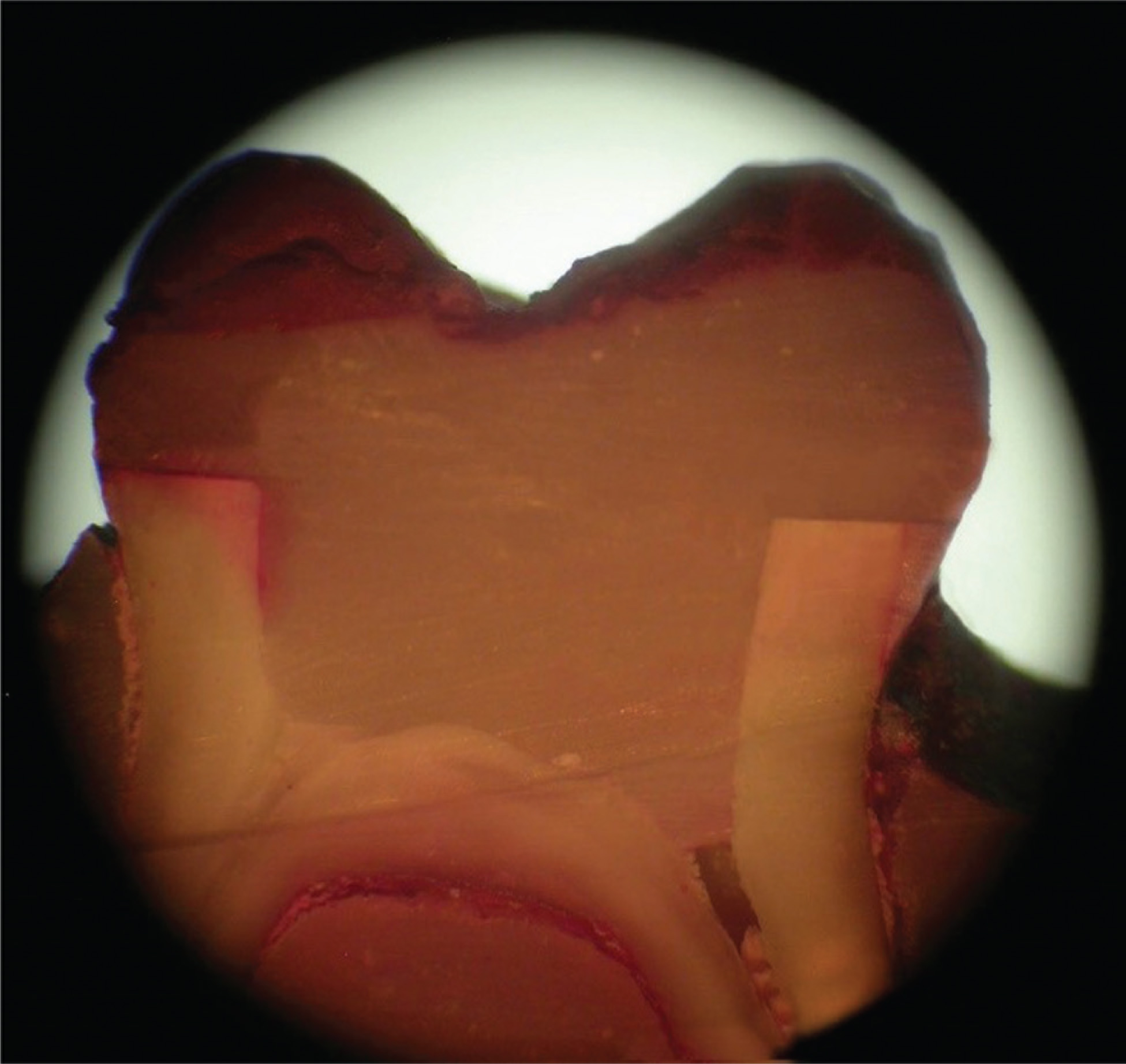
The microleakage scores of the groups are shown in Table 3 (Figures 3-5).
Microleakage Scores of the Groups
Column Chart Showing Microleakage Results
Dye Penetration at the Margins of Group 1 Sample (Occlusal Wall 1, Gingival Wall 2)
Dye Penetration at the Margins of Group 2 Sample (Mesial Wall 4, Distal Wall 0)
Mann-Whitney U test results showed that the endocrown group (1741 ± 379.35 N) had significantly higher fracture strength than the control group (1126.5 ± 405.39 N) (P < .05). On the other hand, no significant difference in microleakage was found between the 2 groups (P > .05).
Discussion
Restoration of endodontically treated primary molar teeth in an optimal way that guarantees their survival until the exfoliation time and the determination of how to reconstruct the remaining structures of these teeth can sometimes lead to disagreements between the child, the parents, and the dentist.
Dentists’ insistence on SSC to provide long-term survival of these badly mutilated teeth might lead to conflicts with parents’ desires for an esthetic treatment. The loss of marginal ridges may be a major factor in weakening teeth and decreasing their fracture resistance, and its conjugation with an endodontic access cavity leads to a dramatic increase in cuspal deflection.19-21 Cuspal reduction was suggested in these badly broken teeth as it led to lower stress values in dental tissues and restorative materials. 22 Therefore, overlay restorations with cuspal coverage are preferable to inlay restorations in the weakened endodontically treated teeth. 23 Adhesive technology was found successful in restoring badly broken teeth and increasing their fracture resistance values. 24 Endocrowns are restorations with increasing popularity in recent years that satisfy all the mentioned rationales and are used widely in endodontically treated permanent molars. To our knowledge, the use of these restorations in primary teeth has never been discussed previously. Our study evaluates fracture strength and mircroleakage of this kind of restoration that can be an esthetic option for primary molar teeth.
Endocrown is a type of restoration that combines core and crown parts as a single unit, using the walls of the pulp chamber for macroretention and adhesive resin cement for microretention.17,25 Endocrown is a contemporary reconstruction option typically indicated for endodontically treated molar teeth.8,14,26 Moreover, many studies found this type of restoration clinically successful.11,27-31
Thermocycling and mechanical loading are commonly used methods during microleakage and fracture resistance testing in in vitro studies that aims to simulate aging and create stresses at the adhesive interface. 32 These stresses are generated during thermocycling due to the difference in the coefficient of thermal expansion between the restorative material and the tooth, and results in microcracks that propagate along the bonded interface. 13
Regarding fracture strength of endocrown restorations, a previous study performed by Biacchi and Basting 26 on permanent mandibular molars found the fracture strength of endocrowns significantly higher than conventional crowns retained by glass fiber posts. In our study, the fracture strength of endocrown restorations made using G-aenial composite systems was compared with restorations made using also G-aenial composites in teeth with Class II cavities with endodontic access openings as a control group. The results showed that endocrown restorations had significantly higher fracture strength than the control group. These observations imply that the endocrown preparation significantly increased the restoration’s strength, likely due to a more homogeneous structure and more favorable distribution of forces over the endocrown restoration rather than the restoration-tooth junction.
Coronal mickroleakage is one of the most common causes of failure of endodontically treated teeth. Microleakage at the margins of restorations allows the passage of bacteria, fluids, molecules, or ions, which leads to stainings at the restoration-tooth interface, postoperative sensitivity, secondary caries, restoration failure, and pulpal pathology. 33 Several methods have been used for the evaluation of microleakage, including dye penetration, bacterial and endotoxin penetration, quantitative analysis of glucose and radioisotope penetration.34,35 Dye penetration is a widely applied method because it is easy, simple and provides the ability for accurate observation using digital imaging.
Abo-Elmagd and Abdel-Aziz 36 studied the microleakage of endocrown restorations in comparison with post and core supported conventional crowns and found endocrowns with butt margins had significantly lower leakage values. Despite some authors stating that bonding of resins to dentin is more difficult and less predictable than bonding to enamel,37,38 and the fact that occlusal enamel is thicker than proximal enamel, our study found no significant difference in microleakage between endocrown restorations and Class II restorations with endodontic access cavities. Although endocrown preparations had 2 proximal (gingival) walls, the preparation of the control group had one occlusal and one gingival surfaces. Our results indicate that the difference in enamel thickness in the 2 preparations did not have a significant effect on the higher fracture strengths of the endocrown group with no significant difference in microleakage in comparison with the other group.
For standardization, all cavity preparations and restoration procedures were carried out by a single operator. Also, standardization of compressive load application point was provided. In our study, artificial periodontium simulation was not done and the teeth were directly embedded in cold-cured acrylic. In other studies, simulation of the periodontal ligament has been performed by different elastomeric materials such as polyether impression material,39-41 silicon rubber material, 42 and urethane rubber material. 43 Artificial periodontium might be necessary to simulate clinical situations in in vitro studies. On the other hand, artificial periodontium simulation has several disadvantages; covering the roots with simulating materials before embedding into acrylic resin might lead to mobility of the sample during loading. Furthermore, these materials have dissimilar elasticity when compared with normal periodontium, which accordingly does not represent the clinical status. Moreover, it has been reported that thickness of silicone material around the roots of the teeth was not standardizable, leading to uncontrolled and unstandardized mobility, thus affecting results. 44
It is known that in vitro tests have limitations in attempts to reproduce the exact clinical condition, and therefore difficulties are inherent in the nature of these studies. The results of the present study do not necessarily reflect the clinical performance of the tested restorative approaches. However, this study provided a controlled environment that allows comparing the behavior of materials under controlled circumstances.
Conclusion
In conclusion, within the limitations of this study:
Endocrown restorations showed significantly higher fracture strength than Class II restorations in endodontically treated primary molar teeth when both restorations were made of the same material (G-aenial system). This indicates that endocrown preparation had a positive effect on fracture strength. No significant difference in microleakage was found between endocrown restorations and Class II restorations with endodontic access openings. Composite endocrown restorations can be a practical and an esthetic option for restoring endodontically treated primary molar teeth. Also, they can be an alternative for SSC in patients with metal allergy. However, more in vivo and in vitro studies are needed before recommending this type of restoration.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.