
Abstract
Objectives:
Supernumerary dentition has been found to occur in various areas of the head and neck. Although they are commonly found along the dental arch, there are some instances of ectopic supernumerary teeth found elsewhere in the upper aero digestive tract. This case report details an impacted molar tooth in the orbital floor.
Methodology:
We present an unusual case of a 30-year-old male with a chief complaint of nasal obstruction. Clinically, it was manifested with an impacted molar in the orbital floor with associated bony expansion into the maxillary and ethmoid sinuses.
Results:
Radiographically, CT scan revealed a benign appearing expansile mass in the left maxilla, completely occupying the sinus and extending into the nose and expanding laterally into the cheek. There appeared to be a well-formed tricuspid tooth clearly visible at the top of this lesion protruding into the left orbit. The patient underwent endoscopic surgical removal, showed findings of an impacted tricuspid in the medial and inferior walls of the orbit. Histopathologic examination confirmed a large cyst lined by thick stratified squamous epithelium and embedded with dense fibrous connective tissue, consistent with an orthokeratinized odontogenic cyst. The medial orbital wall was decompressed, and his postoperative course was uneventful with no orbital complications. Ectopic supernumerary teeth are unusual findings, particularly in association with the orbit. They are frequently impacted and as such can lead to the development of cystic lesions. As with other odontogenic cysts, surgery is usually definitive. This case study demonstrates complete removal with endoscopic surgery.
Introduction
Supernumerary teeth predominantly affect males and are defined as teeth or odontogenic structures that form from tooth germ that are in excess of the typical number of teeth for a given region of the dental arch.1,2 A supernumerary tooth is classified based on morphology, location, form, and number and can result in complications such as crowding, displacement, or cyst formation. 2 Odontogenic cysts, classified as cysts of either developmental or inflammatory origin, are common lesions that derive their lining from residual epithelium involved in the development of the teeth. 3 The orthokeratinized odontogenic cyst (OOC) is a relatively rare subtype of developmental odontogenic cysts. It was delineated as a separate type of odontogenic cyst in the fourth edition of the World Health Organization Classification of Head of Neck Tumors in 2017. 4 The OOC has a predilection for males between the third and fourth decades of life and affects the mandible more commonly than the maxilla. 5 Approximately 50% to 60% of the time, OOCs can be associated with an impacted tooth, which can appear clinically and radiographically similar to a dentigerous cyst.5,6 Ectopic eruption of teeth into regions other than the oral cavity is a rare occurrence; however, it can occur in the nasal cavity, mandibular condyle, coronoid process, palate, and maxillary sinus. 7 The cysts associated with these teeth can persist for years without symptoms and may be detected only by routine imaging. 8 In other cases, patients become symptomatic with signs of sinus disease such as swelling, facial pain, headache, and nasolacrimal duct obstruction. Additionally, a large maxillary cyst can cause orbital and sinonasal symptoms.9-11
Historically, these lesions have been removed using a Caldwell-Luc approach. In the age of endoscopic surgery, we describe the removal of a cyst of this nature in a completely endonasal endoscopic manner. This eliminates the morbidity associated with Caldwell-Luc procedure, predominantly the high risk of oroantral fistula. There is only 1 other case report in the literature describing such removal.
This article describes the unusual case of a 30-year-old male who presented with nasal obstruction due to an impacted molar in the orbital floor with associated cystic changes and bony expansion into the maxillary and ethmoid sinuses.
Case Presentation
A 30-year-old healthy young male presented to a tertiary referral center with progressive left sided nasal obstruction for 6 to 7 months.
On clinical examination, there was no objective facial swelling, tenderness to palpation, or visible masses. Ocular motility and alignment were normal with no proptosis, enophthalmos, or nystagmus. His pupils were equal and reactive to both light and accommodation. Visual acuity was measured at 20/30 + 2 in the left eye and 20/25 + 1 in the right eye. The external nasal exam revealed no lesions, tenderness, trauma, or deformities. In the oral cavity, there were several missing maxillary teeth and 1 fragmented left maxillary molar. On cranial nerve examination, there was a very subtle hypoesthesia in the left V2 distribution, but no other cranial neuropathies were appreciated. Flexible endoscopic examination revealed mild edema and inferior turbinate hypertrophy on the right. However, on the left side, there was evidence of a very large expansile mass with nearly complete nasal airway obstruction, which made further exam posteriorly difficult. The right nasal cavity was otherwise normal, and the remainder of the physical exam was unremarkable.
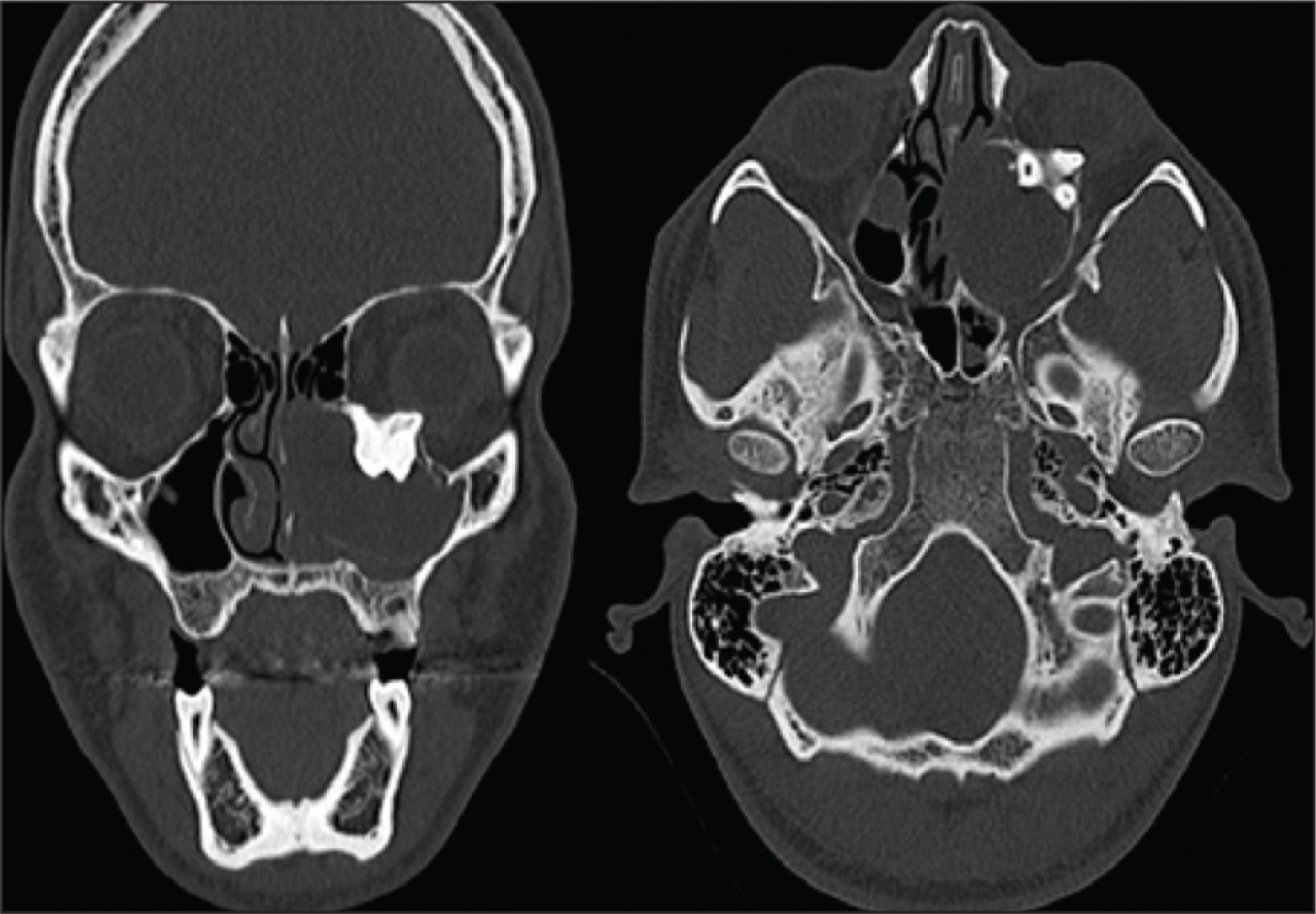
A CT scan demonstrated a large, expansile lesion of the left maxillary sinus associated with an impacted tooth in the floor of the orbit. The patient reported little to no pain and denied orbital symptoms such as diplopia or sudden vision loss. The patient had occasional discharge from the eye but no excess tearing. Review of the outside CT scan revealed a very extensive expansile mass in the left maxilla, completely occupying the maxillary sinus and extending into the nasal cavity medially and the orbital floor superiorly. A well-formed tricuspid tooth was clearly visible at the top of the lesion with protrusion into the left orbit and nearly touching the globe itself, although no other orbital disturbances were evident (Figure 1).
Coronal and Axial Scan Depicting Molar Tooth and Associated Cyst Lodged in the Orbital Floor
Ultimately, the patient was brought to the operating room for definitive surgical management though an endoscopic endonasal approach. Figure 2 demonstrates expansile mass obstructing the left nasal cavity. After proceeding to perform a left maxillary antrostomy, a dense keratinaceous white material was evacuated. This material was consistent with epithelial lesions of an epidermoid type nature, grossly similar to cholesteatoma or epidermoid lesions of the skull base. Wide access to the ethmoid and lamina was achieved by performing a partial middle turbinectomy and a total ethmoidectomy. The displaced third molar tooth was clearly visualized impacted in the orbital floor (Figures 3 and 4). The surrounding bone was thinned out, and the tooth was extracted en bloc with remnants of the orbital floor and medial orbital wall, leaving the periorbita intact. It was then removed from the left nasal cavity (Figure 5).
Expansile mass shown obstructing the left nasal cavity. Superiorly, the middle turbinate can be visualized.a

Keratinaceous Cystic Material Being Removed Endoscopically Through Medial Maxillectomy

Identification of tricuspid molar tooth impacted in the orbital floor. This was able to be removed without violating the orbital floor.
Ectopic tooth with surrounding bone from the orbital floor being removed via the left nares. Cyst removal was performed entirely through an endoscopic approach.

A sphenoidotomy was performed for visualization of the sphenoid sinus contents, and no pathologic material was found. To allow for future disease surveillance and assist in debridement, a modified endoscopic medial maxillectomy was performed. All of the diseased maxillary sinus mucosa was removed. The cavity was irrigated and subsequently packed with Gel-Foam and Merocel packing. There were no intraoperative or postoperative complications. Vision was unchanged, and he had no restriction of gaze in any direction.
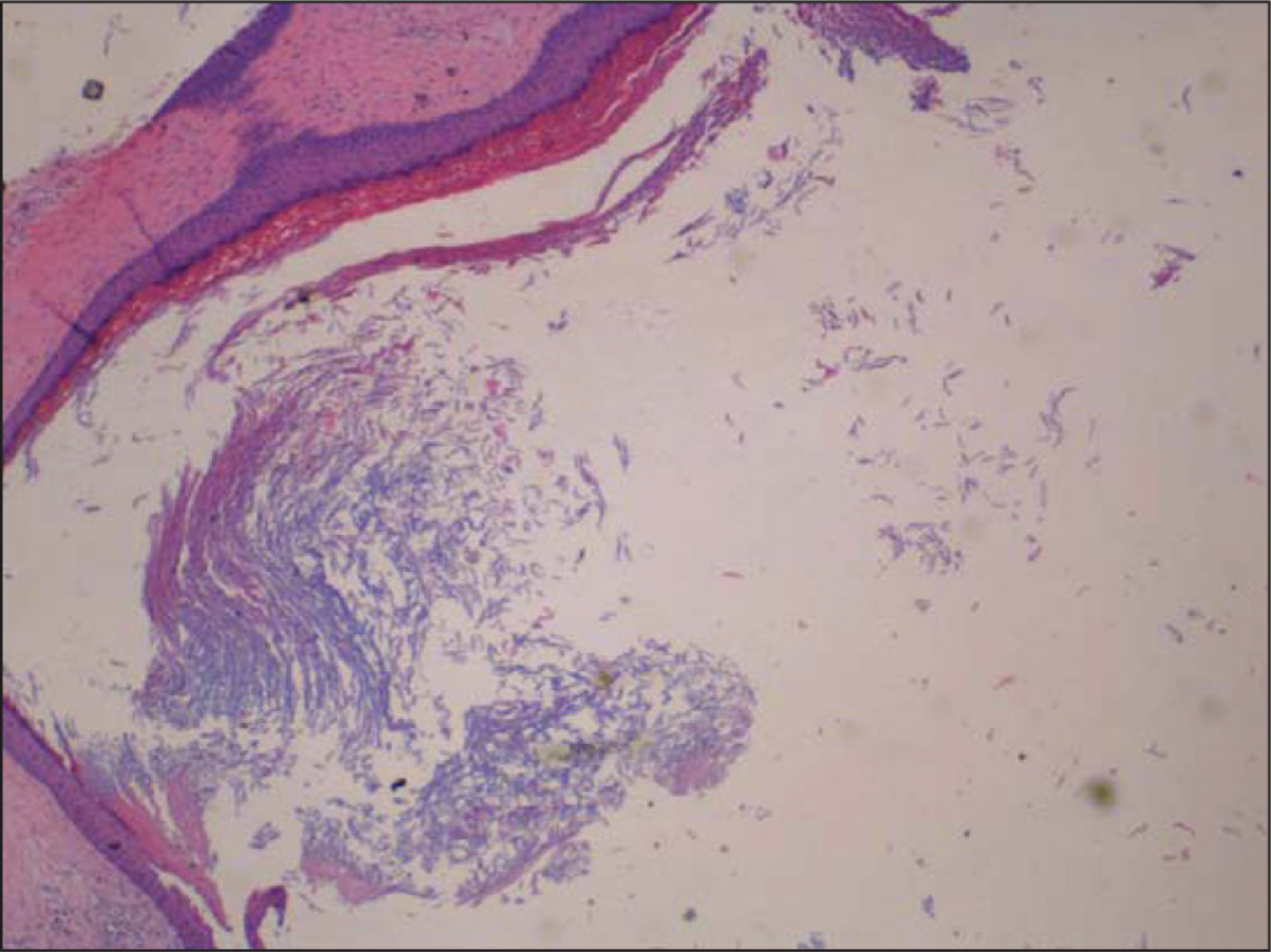
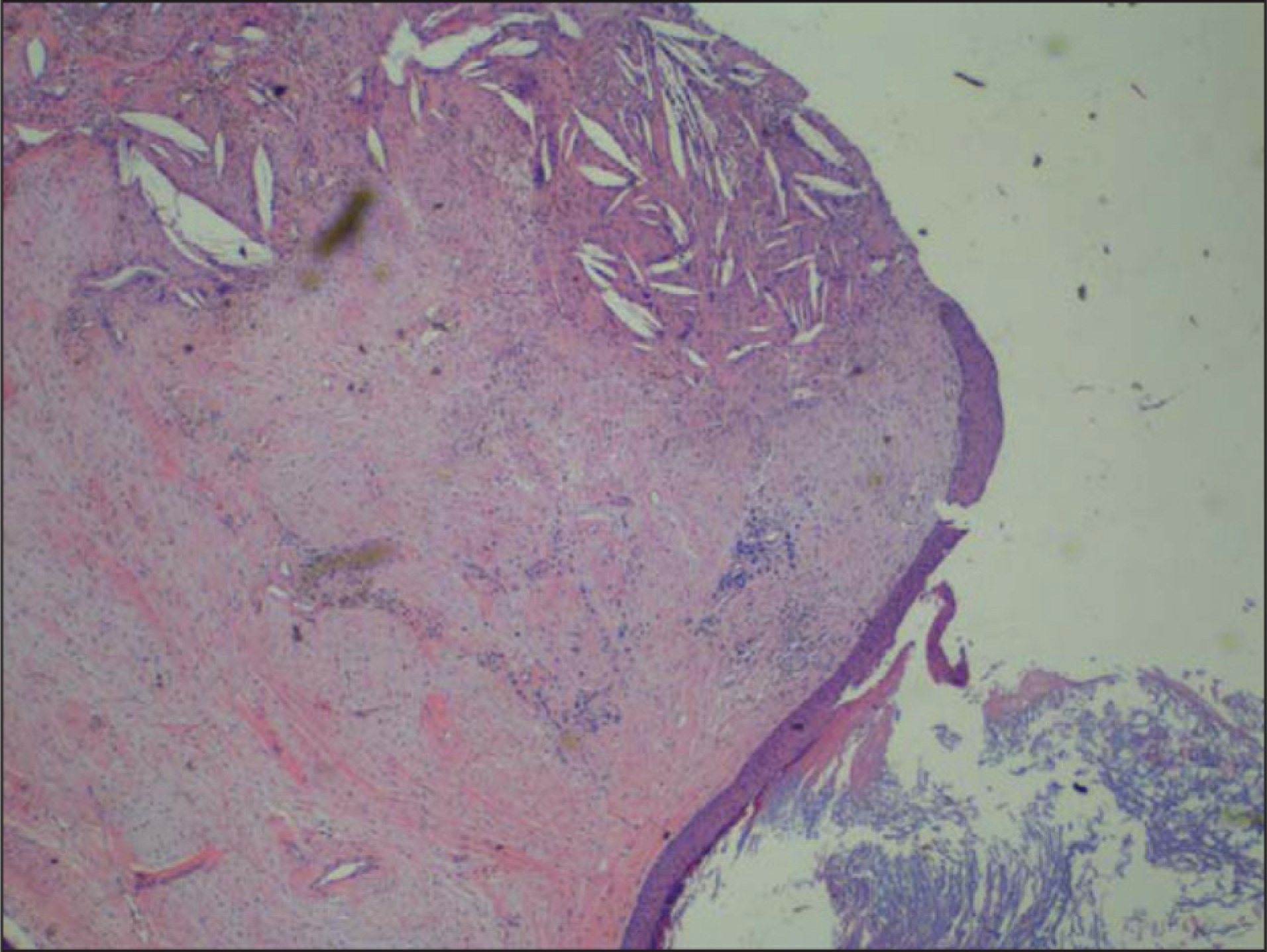
Histopathologic examination confirmed a large cyst lined by thick stratified squamous epithelium and embedded with dense fibrous connective tissue, consistent with an OOC (Figures 6 and 7). The patient was discharged the following day. He followed up in the clinic postoperatively and had no postoperative complications or recurrence of the cyst.
Histopathologic Slide Demonstrating Cyst Wall With Keratin Deposits
Histopathologic Slide Demonstrating Cholesterol Clefts in the Connective Tissue of the Cyst
Discussion
It is infrequent to find ectopic teeth outside of the dental arch, but there have been documented case reports of dentition elsewhere in the upper aero digestive tract. In this case report, we demonstrate a tricuspid tooth that appeared to be impacted and fixed in the left orbital floor. Remarkably, this patient’s symptomatology was related to the expansile nature of the associated cystic lesion into the nasal cavity, resulting in nasal airway obstruction, and he had no orbital symptoms preoperatively or postoperatively.
Most reported cases of ectopic teeth associated with cystic expansion into the maxillary sinus are dentigerous in origin. Because ectopic teeth of the maxillary sinus and their associated dentigerous cysts may affect adjacent structures with their expansion, it is recommended that these be removed surgically to avoid complications. A similar case report involving a 19-year-old male who presented with blurred vision in his right eye was published in the Journal of Craniofacial Surgery. On radiographic imaging, he was found to have an ectopic molar with associated dentigerous cyst that was causing bony erosion of the orbital floor. This was removed via a Caldwell-Luc procedure, and the patient’s symptoms resolved postoperatively.¹¹ In 2006, a dentigerous cyst producing unilateral maxillary sinus opacification on CT secondary to obstruction of the osteomeatal complex was one of the few reported cases at the time to be treated endoscopically via a middle meatal antrostomy. This approach reduces morbidity in comparison with the traditional Caldwell-Luc procedure, which was used more commonly in the past because of its direct visualization into the maxillary sinus. 12 In 2001, a patient presenting with nasal obstruction, hyposmia, facial fullness, and recurrent headaches was found to have an ectopic third molar and associated dentigerous cyst with close adherence to the infraorbital wall. The lesion was also removed endoscopically via middle meatal antrostomy with resolution of presenting symptoms after surgery. 13
As previously mentioned, historically, these lesions were removed through a Caldwell-Luc procedure, which allows for direct visualization into the maxillary sinus. However, this procedure is associated with increased risks and morbidities when compared with endoscopic removal.¹ 4 In an age of increased utility of advanced endoscopic techniques, this particular lesion has become amenable to endoscopic endonasal approaches. The use of angled endoscopes and alternative techniques for accessing maxillary sinus pathology (Denker’s approach, prelacrimal approach) essentially eliminates the need for a Caldwell-Luc procedure.
Classification of odontogenic cysts and tumors has been continually debated in the literature. According to the 2017 World Health Organization Classification of Head and Neck Tumors, the most significant change in this fourth edition was the reclassification of odontogenic keratocysts (OKC). 3 OOC, formerly regarded as a variant of OKC, was recognized as a distinct subtype of odontogenic cyst of developmental origin. In addition to OOC and OKC, the developmental cyst category includes dentigerous cyst, lateral periodontal and botryoid odontogenic cyst, gingival cyst, glandular odontogenic cyst, and calcifying odontogenic cyst. Odontogenic cysts are of inflammatory origin and include radicular cysts and collateral inflammatory cysts. 15 The OOC remains a relatively rare form of odontogenic lesion, and its identifying and distinguishing clinical, radiographic, and histopathologic features have only recently been defined consistently.
The exact incidence of OOC remains unspecified as most were previously considered a variant of OKC. In a systematic review of OOCs conducted in 2010 by MacDonald-Jankowski, 6 48% of OOCs were discovered incidentally, and the most common symptoms were swelling and pain. All groups included demonstrated a predilection for the mandible especially the posterior aspect, and 68% were associated with unerupted third molars. 6
The association of OOCs with unerupted teeth particularly supports inclusion of dentigerous cysts in the differential diagnosis of OOCs. Dentigerous cysts are the second most common type of odontogenic cyst behind radicular cysts and are thought to arise from the follicle of an impacted or unerupted tooth.12,16 Although dentigerous cysts are most commonly associated with mandibular third molars, maxillary canines, or mandibular premolars, an ectopic supernumerary tooth can be involved in an estimated 5% to 6% of cases.17,18
In this case of 30-year-old male who presented with an ectopic supernumerary tooth of orthokeratinized odontogenic origin, the presentation was similar to rare reported cases of dentigerous cysts in the maxillary sinus and, even more rarely, those with orbital involvement. We have shown that even with orbital involvement, it is safe to perform the removal endoscopically and therefore reduce patient morbidity.
Conclusion
Ectopic supernumerary teeth are unusual findings, particularly in association with the orbit. They are frequently impacted and as such can lead to the development of cystic lesions. OOCs are a rare form of developmental odontogenic cysts. As with most odontogenic cysts, surgical management is usually the definitive treatment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.