
Abstract
Introduction:
Orthodontic discrepancies are a common finding in patients with supernumerary teeth (ST). The presence of a ST can cause a number of orthodontic discrepancies, including delayed eruption or retention of adjacent teeth, crowding, spacing, and abnormal root formation. The aim of the present study was to assess the effect of extraction of an anterior supernumerary tooth on the underlying orthodontic discrepancies without additional treatment for a 6-month period.
Methods:
This was a prospective, longitudinal, observational, study. It included 40 participants with orthodontic malocclusions due to maxillary anterior supernumeraries. We examined the changes in the crowding and excessive space in the anterior and posterior segments on cast models.
Results:
In the group that presented with crowding, a statistically significant decrease of 0.95 ± 0.17 mm (P < 0.001) was found between T0 and T1. Of the participants, three exhibited full self-correction. The excessive space at T0 (3.06 mm) decreased by 1.78 ± 0.19 mm to T1 (1.28 mm) in the anterior segment. Seven participants showed full self-correction of the diastemas after the 6-month observation period.
Conclusion:
The results imply that orthodontic treatment can be postponed for at least 6 months after the extraction of the supernumerary tooth as potential self-correction can be expected. This natural alleviation of the malocclusions may make the orthodontic treatment simpler, shorten the treatment time and decrease overall appliance wear time.
Introduction
A supernumerary tooth (ST) is defined as the presence of an additional tooth or odontogenic structure formed from tooth germs in excess of the normal dental formula, i.e. 20 deciduous and 32 permanent teeth, regardless of their location and shape (Syriac et al., 2017).
Tooth development is a continuous process, including several physiological growth mechanisms and different morphological stages to achieve the final tooth shape and structure. The impact of various factors during the initiation stage can lead to the absence of a single or multiple teeth (hypodontia or oligodontia, respectively) or the formation of a ST. The ‘supplemental’ tooth can be found in every part of the dental arch, most commonly in the premaxilla (called mesiodens when located between the two central incisors). A couple of theories aim to explain the appearance of supernumerary teeth, ranging from hyperactivity of dental lamina and atavism to sectioning of the tooth germ and heredity (Consolaro et al., 2021). While most authors (Rotberg and Kopel, 1984; Scanlan and Hodges, 1997) advocate the early removal of ST, others claim that this approach can be hazardous, if performed too early, to the germs or roots of the developing adjacent teeth (Koch et al., 1986; Scanlan and Hodges, 1997). The optimal time for this procedure remains controversial and an individualised approach is suggested according to the chronological and dental age of the patient, tooth localisation and concomitant deviations. Koch et al. (1986) advocate postponing extraction of the ST until the age of 8–10 years to minimise risk of root injury to adjacent teeth. On the other hand, Omer et al. (2010) report the ideal age for removal of a ST to be approximately 6–7 years, for this will allow the spontaneous eruption of the permanent incisors in most cases. Thus, timely intervention may prevent the development of severe malocclusions and shorten the orthodontic treatment time (Omer et al., 2010; Sharma et al., 2010).
ST are diverse in shape (conical, tubercular, supplemental, odontoma) and are found in 1.2%–3.5% of all orthodontically treated patients (Becker, 2002; Mason et al., 2000). The surgical complications that may arise due to mesiodentes include cystic lesions, intra-oral infections, eruption of teeth in the nasal cavity and perforation of the nasopalatine canal (Maddalone et al., 2018; Mallineni, 2014; Mossaz et al., 2014). The presence of an untreated ST, regardless of its eruption status—unerupted, partially erupted or erupted, can cause a number of orthodontic discrepancies, such as delayed eruption or retention of adjacent teeth, displacement of the crowns of the neighbouring teeth, crowding, spacing, abnormal root formation or root resorption and so on (Barham et al., 2022; Campbell and Kindelan, 2006; Mallineni, 2014).
Almost all affected patients manifest some sort of mesiodens-related issues (Barham et al., 2022). Early management is vital to prevent aggravation of the orthodontic discrepancies (Leyland et al., 2006). However, once the malocclusions are present, it is unclear how and to what extent extraction of the ST would influence the aforementioned deviations. In these cases, a multidisciplinary approach is needed to restore the normal anatomy, function and aesthetics (Leyland et al., 2006). Lee et al. (2014) support the early extraction of mesiodens as it would bring about self-correction of the orthodontic discrepancies but their conclusion is based solely on a case report of three participants. Further research is needed on a larger contingent of patients to determine the consequences of ST removal on the orthodontic deviations. The aim of the present study was to follow up the effect of extraction of anterior ST on the orthodontic discrepancies in mixed and permanent dentition for a 6-month period without applying any orthodontic treatment.
Materials and methods
The present study was approved by the University Ethics Committee (reference no. Р-2636/16.10.2019).
Participants
The study comprised 40 Bulgarian participants with a mean age of 10.28 ± 2.11 years (age range = 8–13.0 years) diagnosed with a single maxillary anterior non-inverted ST using a convenience sampling method. All participants were admitted for consultation in the Department of Oral surgery and Department of Orthodontics in the Faculty of Dental Medicine-Plovdiv, Bulgaria with aesthetic or functional complaints over the course of 3 years. They were chosen by an oral surgeon and orthodontist according to the criteria below.
Inclusion criteria
The inclusion criteria consisted of the following: (1) patients with a single erupted or unerupted ST in the maxillary anterior segment; (2) patients with orthodontic discrepancies due to the ST; and (3) patients with no eruption problems due to the ST.
Exclusion criteria
The exclusion criteria consisted of the following: (1) missing teeth or pathological formations adjacent to the ST; (2) jaw injury in the last 2 years; (3) previous orthodontic treatment before the initial examination; (4) ectopic ST, in which the surgical procedure would cause injuries in the maxillo-facial region; (5) syndromic supernumerary teeth; (6) and malocclusions that required immediate initiation of orthodontic treatment.
Intervention
In the present study, all the ST were diagnosed clinically and/or radiographically. Initial study models were also obtained (T0). All participants had a panoramic radiograph and in the cases of impacted ST, cone-beam computed tomography (Figure 1) was also performed. The participants’ parents were thoroughly acquainted with the condition, its possible consequences and the study essence, and signed an informed consent for participation. All ST were removed by the same oral surgeon with no complications thereafter. No orthodontic treatment was performed for the next 6 months and participants were monitored every 3 months by an orthodontist. At 6 months after the extraction, study models were obtained for diagnostic and study purposes (T1).
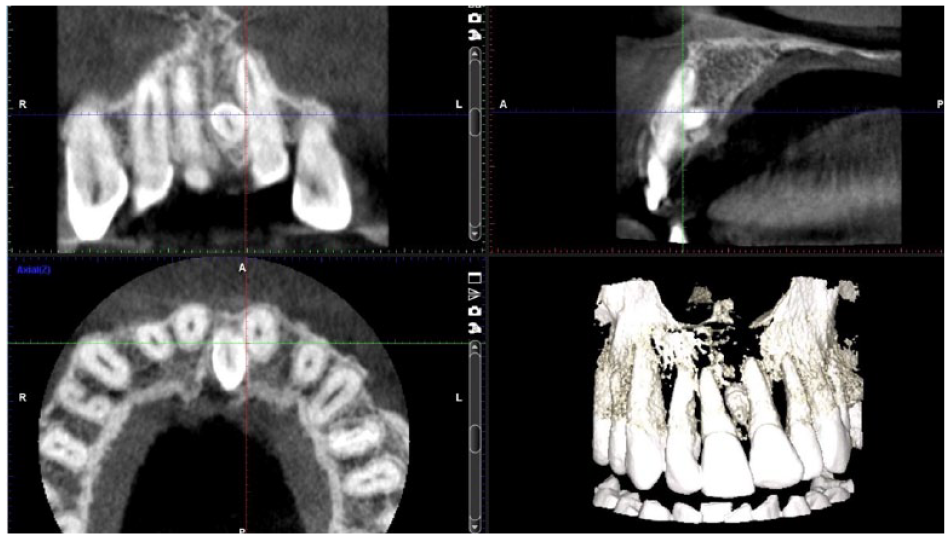
Cone-beam computed tomography of an impacted mesiodens.
We examined the level of dental crowding in the upper dental arch separately for the anterior segment and the two posterior segments clinically and on study models. We defined the anterior segment as the part between the distal anatomical contact point of the two canines (primary or permanent). The posterior segment was defined as the area between the distal contact point of the canine and the mesial contact point of the first permanent molar. We examined the change in the severity of crowding and width of diastemas and tremas (gaps between the teeth) before the ST extraction (T0) and 6 months after its removal (T1). Crowding is a condition in which the distance between distal surfaces of the maxillary canines (in the anterior segment) and the distance between the distal surface of the maxillary canine and mesial surface of the first permanent molar (in the posterior segment) is insufficient to accommodate the teeth in the line of the arch. Diastemas and tremas were considered to be present when spaces were greater than 1 mm.
Comparison
All measurements were performed by the same orthodontist on the cast models obtained at T0 and T1 using a Williams periodontal probe CP10 (Medesy) (Figure 2) marked with a 1-mm scale. To determine the presence or absence of crowding, the perimeter of the three segments was measured and compared against the sum of mesio-distal widths of the present teeth (not including the ST) in the corresponding segments. These measurements were performed before the extraction and again 6 months after it. The erupted ST were excluded from all measurements as there could be no comparability between the space needed for the teeth present at T0 and T1. Crowding was considered present when the difference between the available space and the sum of mesio-distal width of the teeth was greater than 1 mm.

Williams periodontal probe CP10.
The examination for excessive space in the respective segments was performed in a similar manner at T0 and T1. The same periodontal probe was used, placing it perpendicular to the long axes of the teeth adjacent to the tremas or diastemas to measure the spaces (Figure 3).

Measurement of a diastema due to mesiodens.
Outcomes
All parameters were measured and registered with the participants’ names omitted from the models twice by the same orthodontist with a 2-week interval to minimise bias. The mean values were used for the statistical analysis. We monitored for exfoliation of primary teeth and eruption or extraction of permanent teeth as this could influence the results, since it changes the sum of mesio-distal width of present teeth. At T1, all participants’ orthodontic treatment needs were assessed to determine who required additional intervention.
Study design
This was a prospective, longitudinal, observational, study of 40 participants diagnosed with ST and orthodontic discrepancies.
Sample size calculation
Although the two separate groups consisted of a small number of participants, they exceeded the estimated size of power calculation. The calculation of the minimal required sample size for a paired t-test was performed using Minitab statistical software version 21.3.1 (2022). We assumed a mean difference between T0 and T1 with an absolute value of 0.50 mm, a standard deviation of the paired differences of ±0.30, a Type I error of 0.05 and a power of 0.90 (Type II error = 0.10). For the entered parameters, the minimum required number of pairs was 7, with an actual power of 0.95 versus a target power of 0.90. This reassured us that the available data would be sufficient to detect systematically occurring differences in the same participants between T0 and T1.
Statistical analyses
The interclass correlation coefficients was used to determine intra-observer reliability between the two measurements. The statistical analysis was performed using SPSS Statistics for Windows version 20 (IBM, 2011). The Shapiro–Wilk test was used to determine the normality of the continuous variables. The paired-samples t-test was used to examine changes in crowding and excessive space in the anterior and posterior segments as all target variables were normally distributed (P > 0.05 for all tests). A frequency analysis of qualitative variables (nominal and ordinal) was also carried out, including absolute frequencies, relative frequencies (in percentages) and cumulative relative frequencies (in percentages). All statistical tests were two-tailed and statistical significance was accepted at P < 0.05.
Results
The intra-observer reliability between the two measurements showed a value of 0.95. There was one drop-out of the study because they exhibited exfoliation of primary teeth and eruption of their permanent successor, which affected the needed space and the comparability of the results. Hence, 39 participants (31 boys [79.5%], 8 girls [20.5%]) in mixed or permanent dentition were included in the statistical analysis of the results. There were 23 (59%) erupted ST of all supernumeraries while there were 16 (41%) unerupted ones. Out of the 39 participants, 19 (48.7%) had crowding in the anterior segment, 18 (46.2%) exhibited excessive space in the anterior segment, 2 (5.1%) had crowding in the posterior segment and no participants had excessive space in the posterior segments (Table 1).
Study participants.
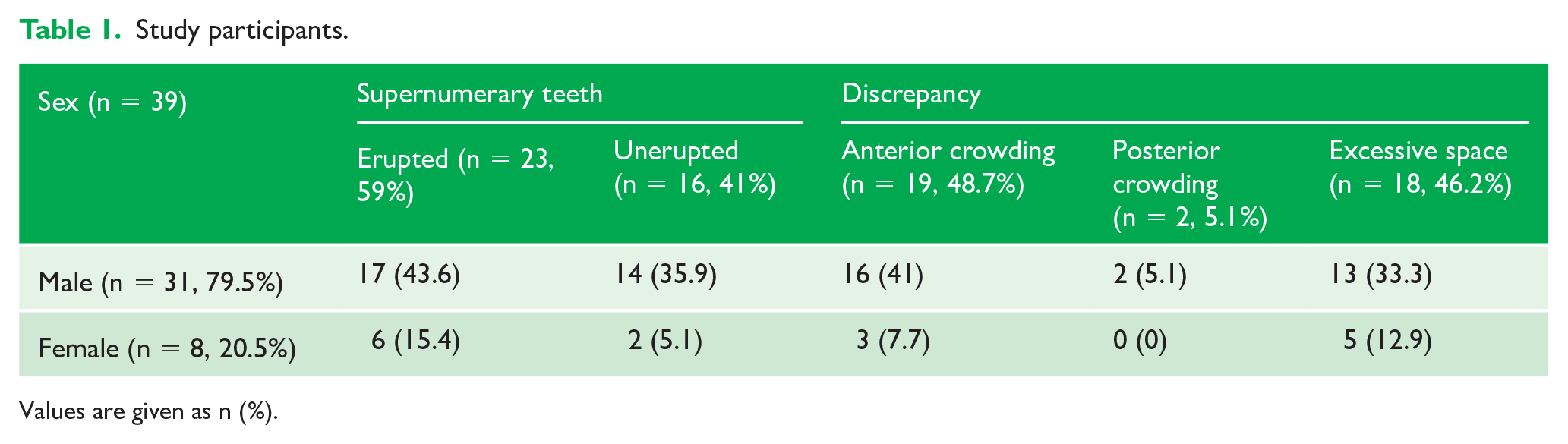
Values are given as n (%).
Crowding
After the repeated measurements in the group presented with crowding a statistically significant decrease of 0.95 ± 0.17 mm (P < 0.001) was found between T0 (2.95 ± 1.28 mm) and T1 (2.00 ± 1.45 mm) in the anterior segment. The right posterior segment presented a difference of 0.25 mm, which was neither clinically nor statistically significant. In the left posterior segment, no change was documented (Table 2). Out of the 21 participants with crowding, 3 (14.3%) exhibited full self-correction, all of whom had anterior crowding (Table 3).
Change of crowding (n = 21).
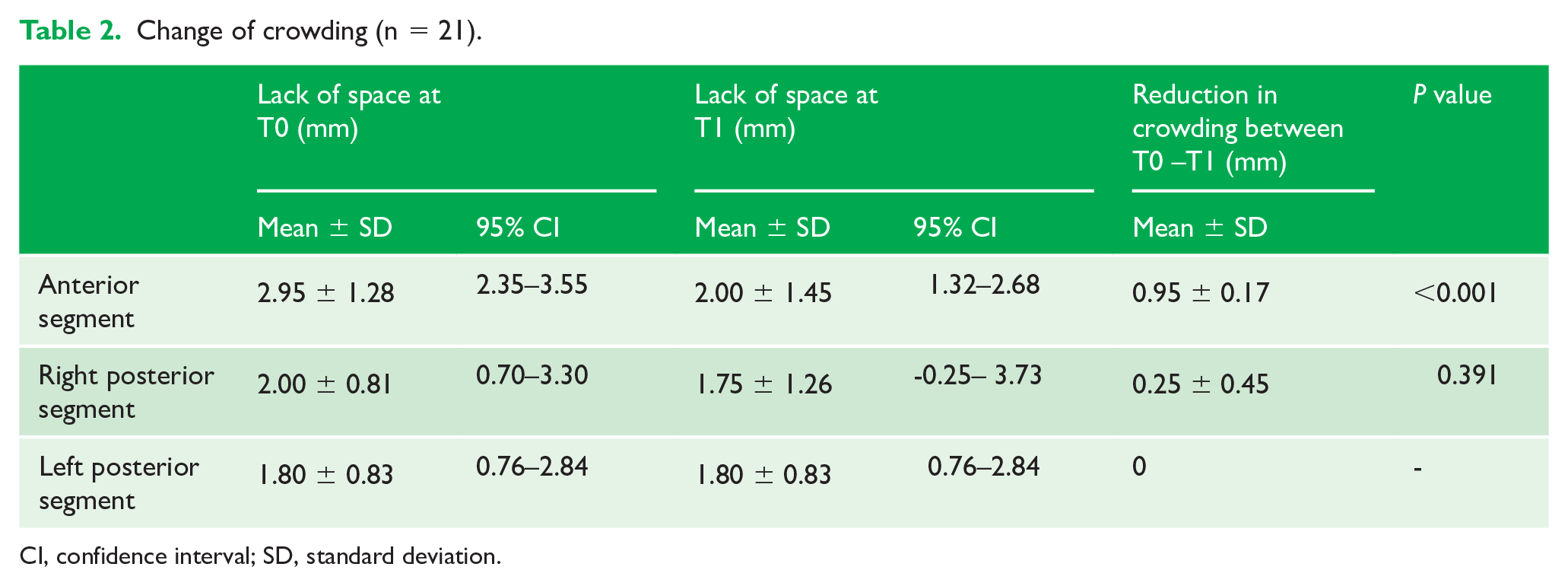
CI, confidence interval; SD, standard deviation.
Self-correction.
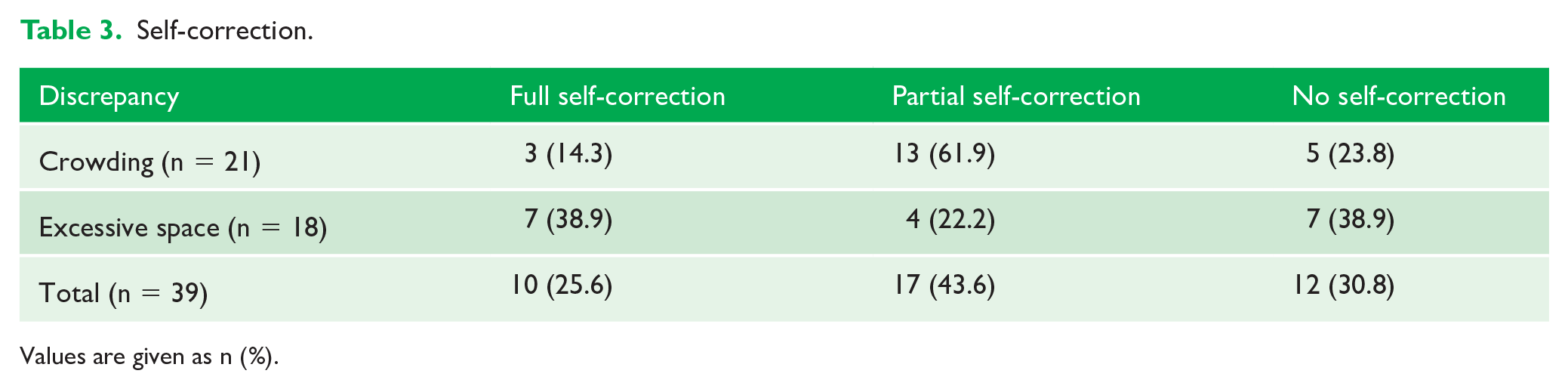
Values are given as n (%).
Excessive space
The excessive space at T0 (3.06 ± 1.21 mm) decreased by 1.78 ± 0.19 mm to 1.28 ± 1.40 mm at T1 in the anterior segment (Table 4). This result was statistically significant (P < 0.001). Out of the 18 participants with excessive anterior space, 7 (38.9%) also showed full self-correction (Figure 4) after the 6-month observation period (Table 3). The posterior segments exhibited no change in their values.
Change of excessive space (n = 19).
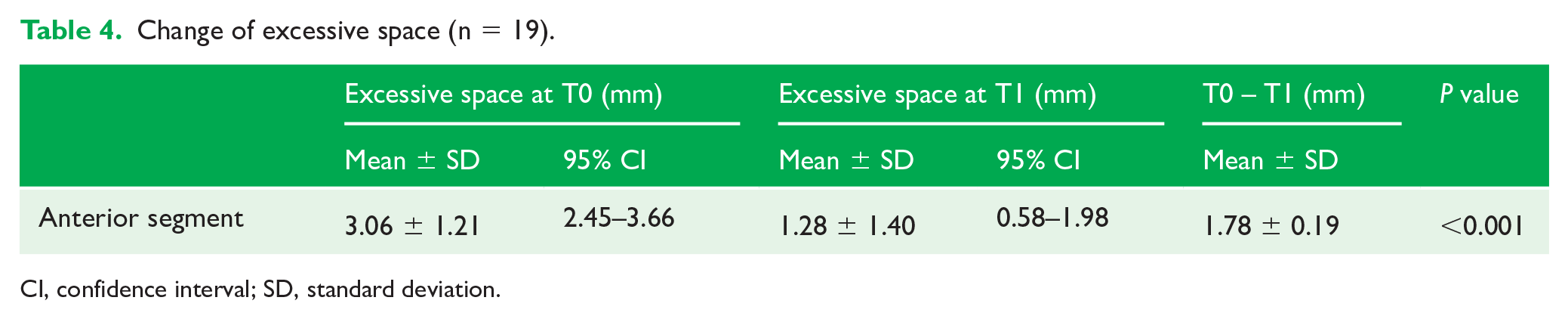
CI, confidence interval; SD, standard deviation.
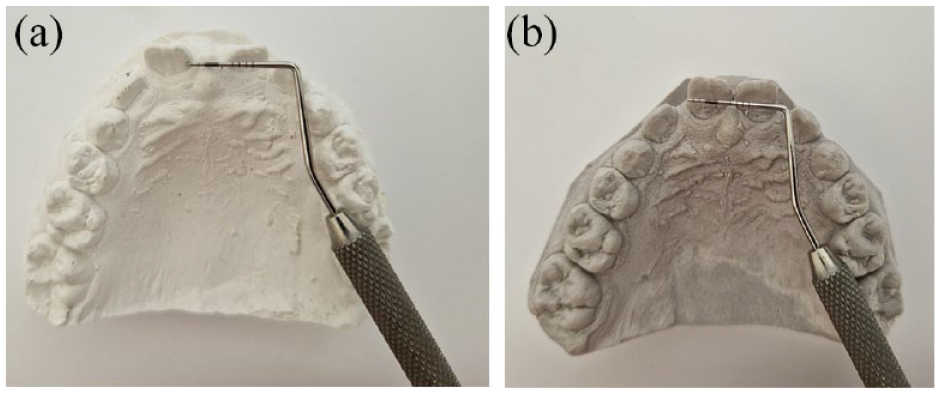
(a) Diastema before the extraction of the mesiodens and (b) self-correction of the diastema after the extraction of mesiodens.
Of the participants, 12 presented no change in the orthodontic discrepancies after the 6-month observation period (crowding, n = 5; excessive space, n = 7).
At T1, in terms of spacing and crowding, 21 (53.8%) participants were considered in need of further orthodontic intervention. The other 18 (46.2%) participants included the 10 with full self-correction and eight with partial self-correction who had 1 mm or less of crowding or spacing that was deemed unnecessary to treat at this point as further self-correction with growth was expected. Nevertheless, due to unresolved concomitant sagittal and vertical discrepancies, such as class II or overbite tendency, 34 (87%) out of the 39 participants were offered additional orthodontic help after the observational period.
Discussion
Summary
This study demonstrates self-correction of the orthodontic abnormalities after the removal of an anterior ST and reduction in the severity of crowding and excessive space. After removal of the ST, alignment of the existing teeth was improved under the influence of the force generated from the surrounding soft tissues. Thus, the permanent teeth acquired a better position in the dental arch, resolving the crowding either completely or partially. This is in line with previous research that reports restoring the proper alignment after extraction of the ST (Lee et al., 2014).
The width of the diastemas and tremas also decreased 6 months after the extraction. We account for this phenomenon by the natural tendency for mesialisation and further root development of the anterior teeth. This process was additionally facilitated by the newly formed, low-density bone at the extraction site (Diedrich and Wehrbein, 1997). Some participants did not exhibit self-correction as the reason for the excessive space could include impaired tongue function, heredity and long labial frenula.
Limitations
A true limitation of this study was the lack of a control group with unextracted ST. This would allow us to determine the extent to which the documented changes were due to normal growth or ST removal. However, this would raise ethical issues for any dental complications and prolonged orthodontic treatment that could potentially entail. Other drawbacks were the selection bias because of the convenience sampling method utilised and the 6-month follow-up period for self-correction. A longer observational period could be considered for future studies for patients with extraction of ST who refuse orthodontic treatment, for instance.
Comparisons with other studies
Diastemas or crowding are typical clinical findings in patients with unerupted ST. According to Barham et al. (2022), the most common finding is displacement of adjacent teeth’s crowns accounting for 29% of cases, followed by diastema in 17% and delayed eruption in 6.3%, while other studies (Jung et al., 2016; Koch et al., 1986) report a diastema and delayed eruption to be the most prevalent ones. Displacement of the adjacent teeth varies from mild rotations to severe crowding (Anil, 2012; Mallineni, 2014) and is observed in 28%–63% of the cases according to Ata-Ali et al. (2014). This is in line with our results, which indicate 53.8% crowding. The higher prevalence of crowding could be potentially attributed to the higher percentage of erupted ST (59%) among our participants. In our study, 46.2% of the participants presented with a diastema before the mesiodens extraction. According to Mallineni (2014), mesiodens can be a causative factor for the development of diastema in 10% of cases. Other studies report a higher percentage of diastema presence – from 22.2% (Syriac et al., 2017) and 28.6% (Ata-Ali et al., 2014) to 52.2% (Shih et al., 2016), the latter of which is in agreement with our results.
Implications for clinical practice
The reported 0.95-mm self-correction in our research does not hold great clinical significance; however, additional self-correction may be expected for a longer observational period in patients who are actively growing or have residual jaw growth. While 34 out of the 39 participants (87%) were offered additional orthodontic treatment, had it not been for the concomitant malocclusions, only 21 (54%) needed it due to unresolved crowding or spacing. This implies that around half of the participants did not need further treatment 6 months after removal of the ST provided no additional discrepancies were present. These results apply to only one ethnic and age group and caution should be exercised, if they are to be extrapolated to other populations.
Implications for further research
Additional division of the results according to the eruption status of the ST, erupted or unerupted, would be beneficial. However, the current sample size was insufficient to make such further differentiation. This could be an area of research for future investigations.
Conclusion
The results from the study imply that orthodontic treatment can be postponed for at least 6 months after extraction of the ST as potential self-correction can be expected. This natural alleviation of the malocclusions may make the orthodontic treatment simpler, boost the child’s confidence, shorten the treatment time, which is crucial for patients with unsatisfactory oral hygiene, and decrease overall appliance wear time.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.