
Abstract
Background:
Updated information on oral health status could be used to monitor oral disease patterns, as widespread variations in oral health outcomes within and between different countries are reported.
Aim:
The objective was to examine the status of oral and systemic health and their association with demographic characteristics of the population attending a public dental center.
Methods:
A cross-sectional secondary analysis of the patients’ record was conducted during June 2017 attending the dental center of Madina Teaching hospital Faisalabad, Pakistan. Study variables were analyzed using the t test and the c2 test with a significance level of P ≤ .050.
Results:
The mean age of the study sample was 31.9 ± 14.5 years; 56% were females; 48% had primary or higher education; 9% were hypertensive; 5% had hepatitis; and 5% diabetes mellitus; 52% were with poor oral hygiene, 68% had dental caries, 84% had no fillings, 27% had tooth loss, and 99% functional dentition; 74% patients had calculus, 67% had gingivitis, and 5% had periodontitis. Age was the strongest risk indicator. Dental caries, tooth loss, poor oral hygiene, gingivitis, periodontitis, and tooth mobility were significantly associated with diabetes mellitus; tooth loss and tooth mobility were associated with cardiac disease; tooth loss, periodontitis, and tooth mobility were associated with hypertension, whereas tooth loss and calculus were associated with hepatitis. Higher age and lower income were positively associated with poor oral hygiene.
Conclusion:
Age and gender remain to be the strongest predictors for both oral and systemic conditions. Poor oral health and tooth loss showed a strong relationship with chronic systemic conditions.
Introduction
Oral diseases are among the most common chronic diseases worldwide. Widespread variations in oral health outcomes within and between different countries are reported. 1 Scientific research refers these variations to various sociodemographic, psychosocial, and behavioral factors. 2 Whitehead and Dahlgren 3 proposed age and sex to occupy a central position, whereas material and social factors as proximal factors to affect health events. People are exposed to numerous oral health risk factors originating from genetic, environmental, behavioral, and sociodemographic factors, and these have been assessed for risk assessment, prevalence, disease pattern, and rate of onset of oral disease. 4
Data regarding oral health status could be used to monitor oral disease patterns and make an essential component of the oral health information system. The Pakistani population is less well studied with respect to oral health status and systemic conditions, as very few studies have reported on demographic, systemic, and oral health status. 5 Oral health is poor in a majority of developing countries, and Pakistan is no exception. 6 In Pakistan, oral health care is available in both public and private sectors. Many nongovernment organizations or nonprofit organizations are providing services in both the health and education sectors. 7 The primary aim of this study was to assess the oral health status of the population attending a private teaching dental center that offers free treatment. The secondary aim was to observe the relationship of demographic risk indicators of age and gender with the oral health and systemic outcomes.
Materials and Methods
Study Type, Setting, and Sample
This cross-sectional study was performed at dental clinics of the University Medical and Dental College (UMDC) Faisalabad, Pakistan, during June 2017. Study participants (sample) were all patients reporting the dental clinics for checkup or treatment during the study period. Patients visiting the dental clinics hail mainly from Faisalabad. All patients were included in the study except those who gave incomplete information or refused examination as per data collection form. Informed consent was taken for all patients as per hospital requirement.
Data Collection
Data on all dental patients were collected from ‘patient data files’ for the 1 to 30 June period from the dental clinics and assessed for appropriateness and entry into the computer. Data collection form was designed for the study (by the first and second authors) and was based on the information recorded in the dental clinic data forms. This form includes the following 5 sections:
Section I includes sociodemographic characteristics (age, gender, marital status [see the Data Analysis section], education, occupation, and residence). Section II includes systemic conditions (diabetes, hypertension, coronary heart disease (CHD), hepatitis, respiratory condition, bleeding disorder, epilepsy, allergy, pregnancy, any medication). Section III includes oral/dental conditions (dental caries, filled teeth, missing teeth [only extracted teeth, excluding last molars and exfoliated], oral hygiene, calculus, gingivitis, periodontitis, tooth mobility, tempromandibular joint (TMJ) dysfunction, malocclusion, rosthesis, and oral lesion. Section IV records the patient’s present complaint(s). Section V records referral department for treatment. At UMDC dental clinics, dental patients are received and registered at reception.
Dental surgeons and trained assistants record the demographic, medical, and dental history of patients and perform oral examination for patients’ oral health status. Later on, patients are provided the required treatment. All the information so observed and gathered, are entered on the “data collection form.” Dental surgeons for oral examinations were trained and calibrated in the use of oral indices (calculus index, plaque index, mobility index, DMFT index, presence/absence of malocclusion) with the principal investigator (S.A.H.B.) of the study with an intraexaminer and interexaminer reliability of ≥.87. To avoid bias, the first and second authors of the study randomly reexamined few patients every day for the confirmation of recorded data and oral health status. The principal investigator performed the final evaluation of the recorded data.
Data Analysis
Patients with incomplete data were excluded. For this study, demographic variables of age and gender are used as independent parameters to compare status and relationship of systemic and oral/dental conditions among the study participants. The t test was applied for continuous variables and the c2 test for categorical variables; the Pearson correlation coefficient was also calculated. Age was subgrouped by a gap of 10 years. Functional dentition was calculated on presence of ≥20 teeth by subtracting missing teeth from 32 teeth. 8 Oral and systemic variables with less than 2% prevalence were excluded from analysis. SPSS (version 16; IBM) was applied for data entry and analysis. Significance level was set at P ≤ .050 (95% confidence interval). Variables (such as marital status and residence) were missing from many files and were therefore not included in the analysis.
Ethical Approval
Ethical approval was obtained from the management committee of the university dental clinics vide letter #UMDC-DC-178/17, dated April 26, 2017.
Results
This study provides descriptive analysis on patients’ demographic, systemic, and oral health characteristics noted from the patients’ data files. This convenience sample comprised of 1430 patients’ data files during the study period of one month. Data of 1177 patients were found suitable and complete for this study analysis.
Demographic Characteristics
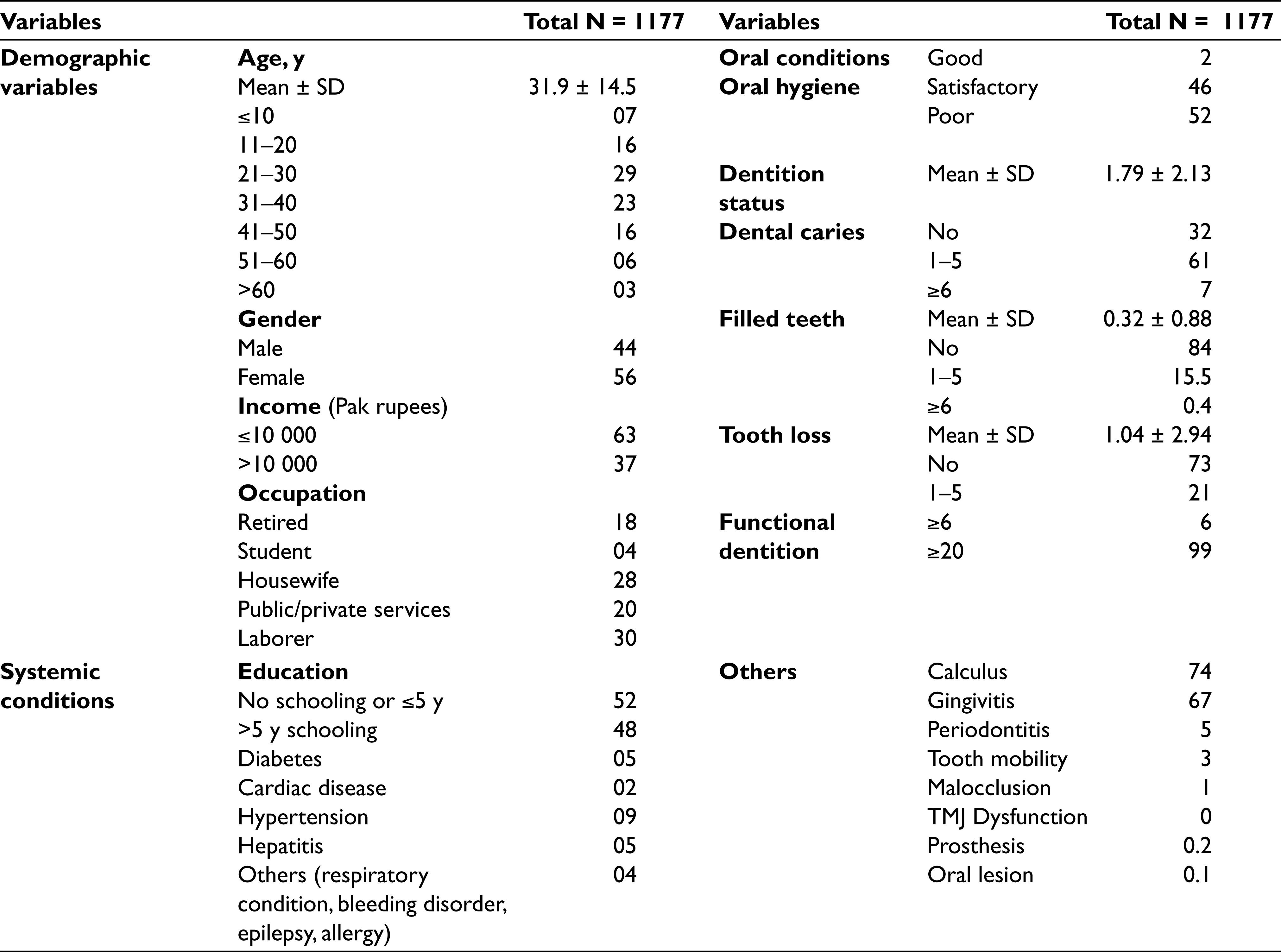
The average age of the sample was 31.9 ± 14.5 years. A majority (52%) of patients were 21 to 40 years old; 56% were females; 72% among the females were housewives; and 48% of the study sample had primary or higher school education. By age groups, a significant difference was noted among genders (P = .007; Table 1).
Systemic Health Variables
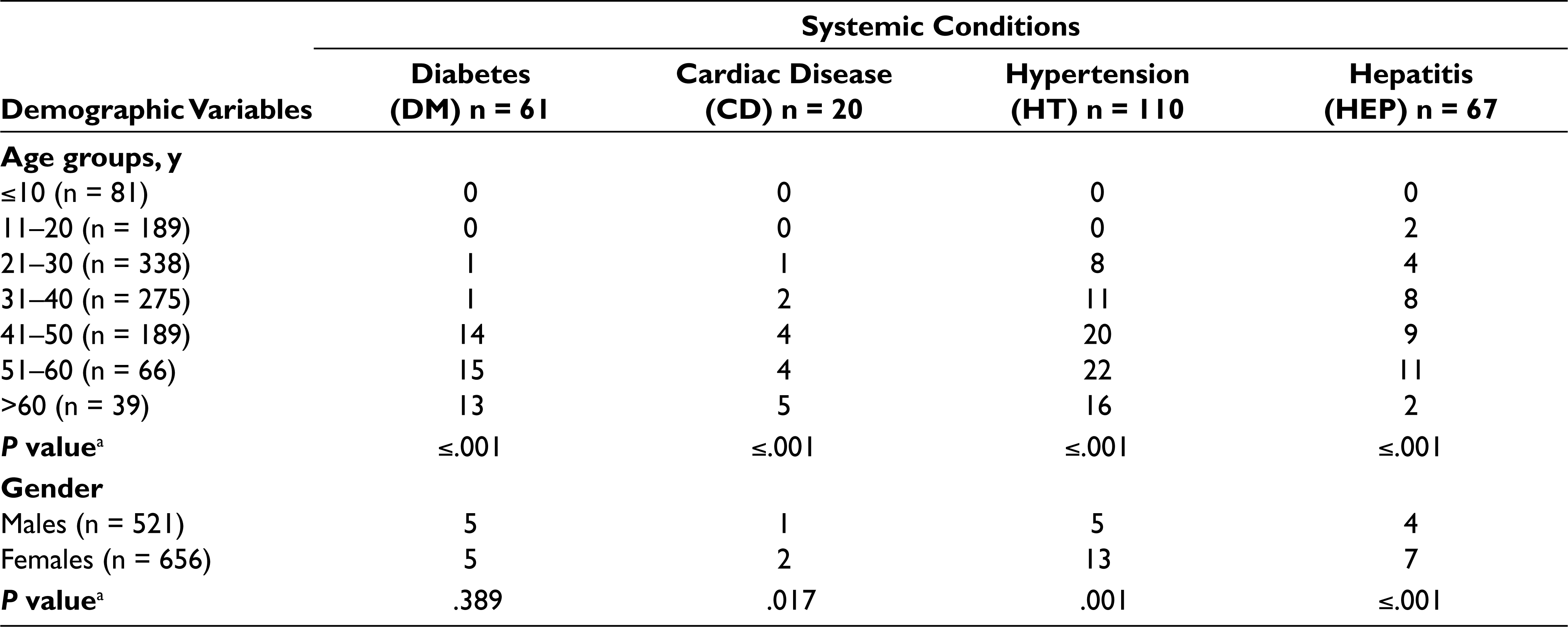
Seventy-five percent of this sample did not report any systemic ailment. Systemic conditions of hypertension, diabetes, CHD, and hepatitis showed a highly significant association with age groups (P ≤ .001). Cardiac disease, hypertension, and hepatitis were significantly higher in females (P ≤ .017). Coefficient correlation analysis showed a positive relationship among age and diabetes mellitus, cardiac disease, hypertension, and hepatitis. Gender was positively correlated with cardiac disease, hypertension, and hepatitis (Tables 1 and 2).
Oral/Dental Health Variables
Fifty-two percent of the study population was noted with poor oral hygiene and 68%—61% ≤5 and 7% ≥6—dental caries; 84% patients did not have fillings; 23% had tooth loss. Seventy-four percent of the study sample was presented with calculus; 67% with gingivitis; 5% with periodontitis; and 3% showed tooth mobility (Table 1).
The highest level of dental caries was observed in the age group of ≤ 10 years, consecutively followed by the age groups of 31 to 40, 21 to 30, >60, 41 to 50, 51 to 60, and 11 to 20 years. The number of dental fillings was the lowest in the age group of ≤10 years; maximum fillings were noted in the 31- to 40-year age group. Twenty-seven percent showed tooth loss with a mean level of 1.04 ± 2.9. Highest tooth loss was noted in the >60-year age group. Functional dentition (≥20 teeth) was observed in 99% of the study population; the highest percentage (7%) with nonfunctional dentition was noted in the >60-year age group, and a significant difference (P ≤ .001) was noted in the >30- and ≤30-year age groups (Table 3).
There was a significant difference in the status of dental caries, fillings, tooth loss, oral hygiene, calculus, gingivitis, periodontal disease, and tooth mobility between age groups. Pearson coefficient correlation analysis showed a significantly positive correlation of age with oral/dental health variables (Tables 1 and 3).
Distribution of Participants (%) With Respect to Study Variables Observed in This Study
Age- and Gender-Related Status of Systemic Conditions Among Study Participants (%) of This Study
Age-Related Status of Oral Conditions Among Study Participants (Mean ± SD and %) of This Study
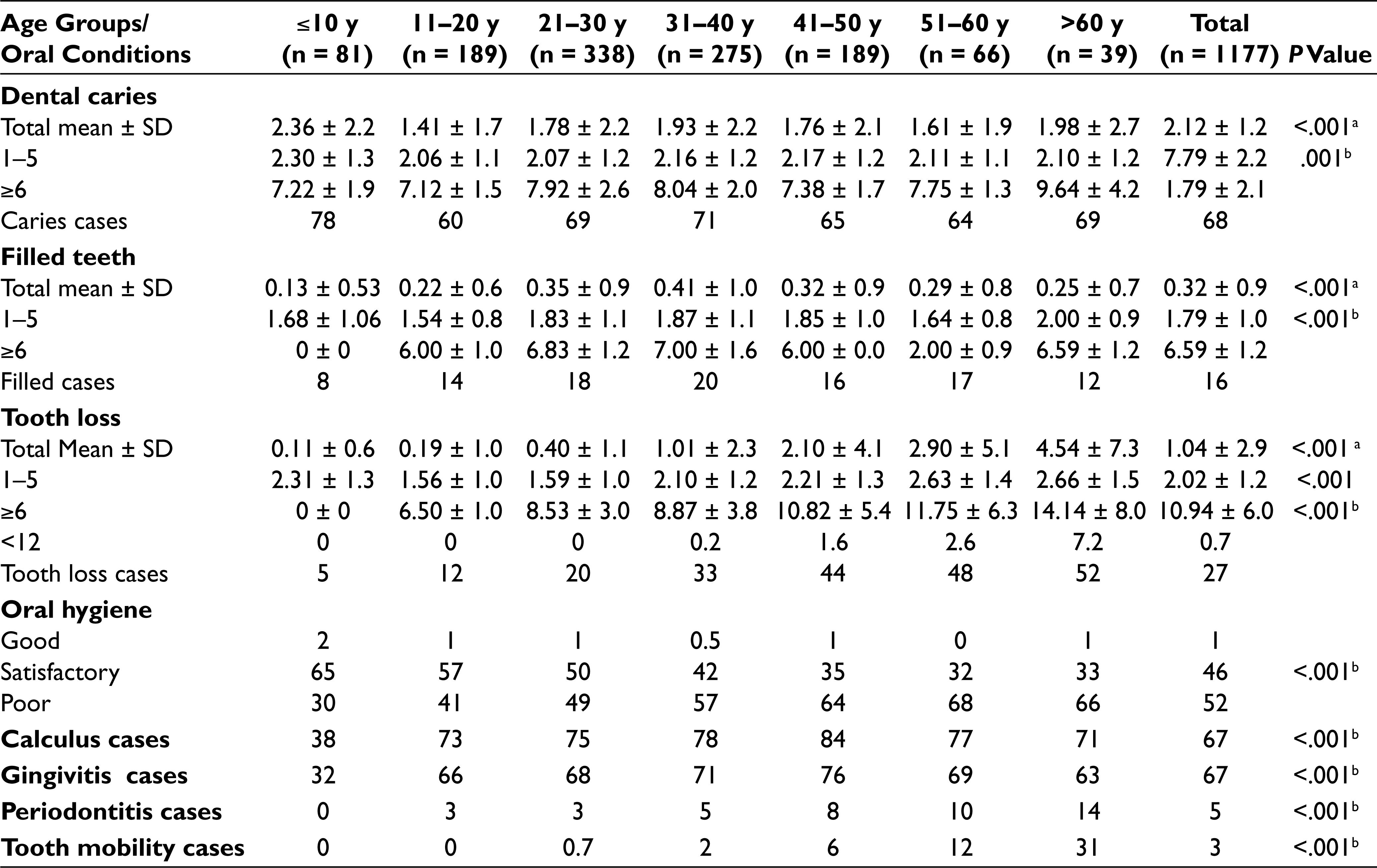
bThe c2 test.
Gender differences for status of calculus, gingivitis, periodontitis, and tooth mobility were insignificant. Pearson coefficient correlation analysis showed a significantly positive correlation of gender with oral/dental health variables (Table 4).
Gender-Related Status of Oral Conditions Among Study Participants (Mean ± SD and %) of This Study
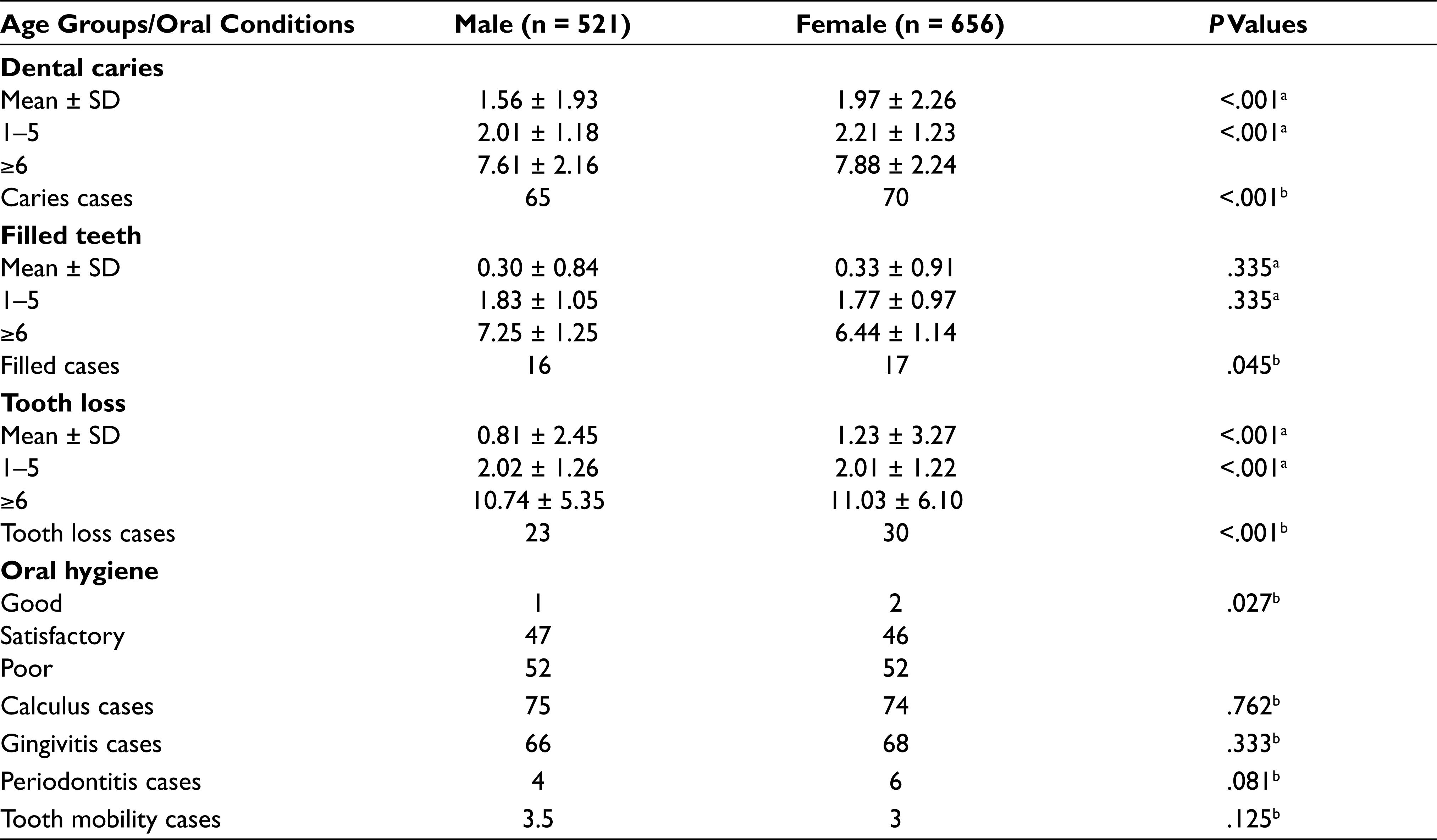
bThe c2 test.
Table 5 presents relationship and odds ratios of systemic and oral conditions with highest risk ratio of 3.78 (2.07–6.90) for tooth mobility and cardiac disease and 2.13 (1.44–6.90, P ≤ .001) for diabetes mellitus. Pearson coefficient correlation analysis showed a significantly positive correlation of gender with oral/dental health variables.
Distribution of Study Participants (%/P Values/Odds Ratios [95%CI]) With Respect to Systemic and Oral Conditions
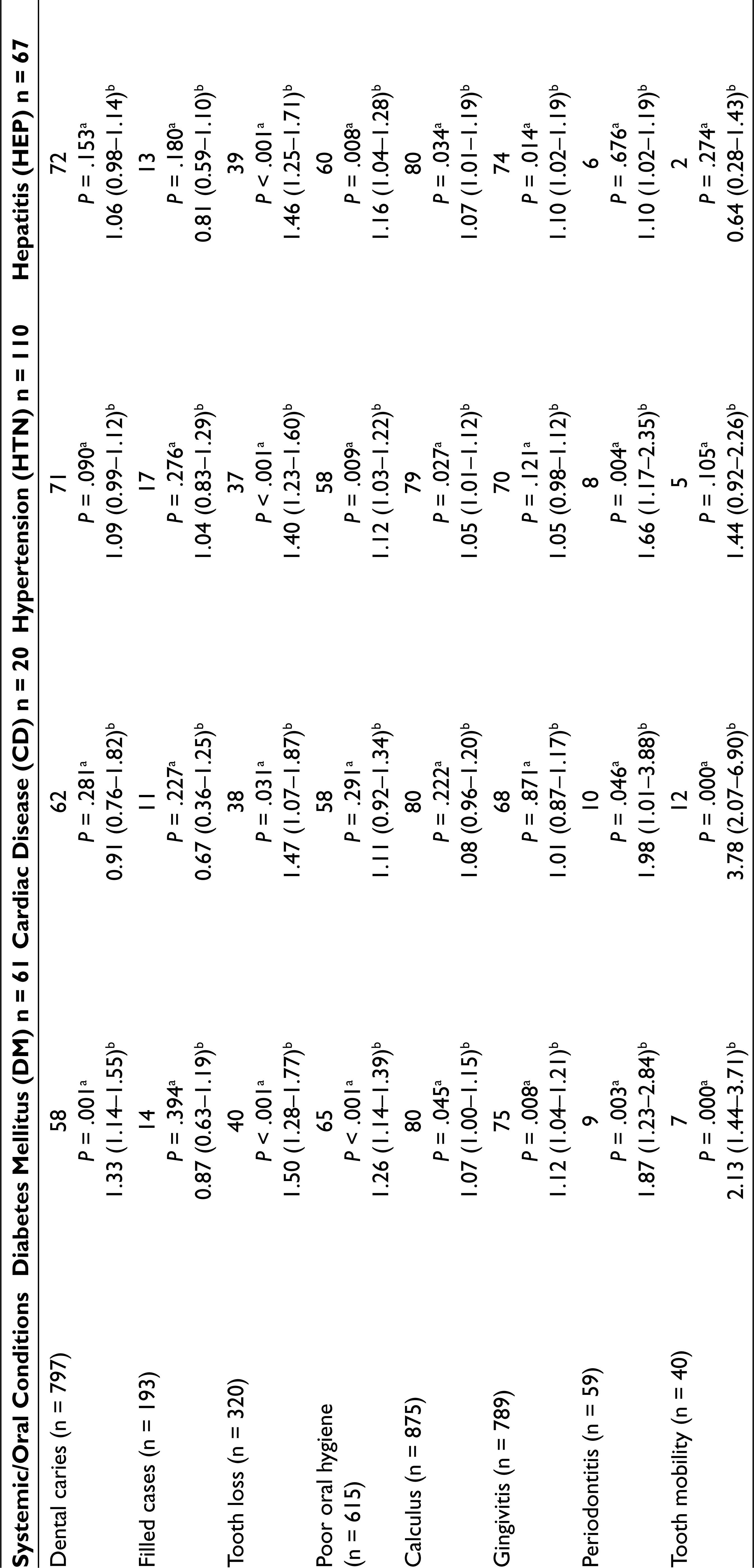
bOdds ratio.
Table 6 presents relationship and odds ratios of demographic and oral conditions with the highest risk ratio of 3.61 (3.15-4.16, P <.001) for tooth loss and age group >30 years.
Odds Ratios (OR) (95% CI) of Oral Conditions for Demographic Risk Factors

Discussion
Social and demographic factors have a strong impact on oral disease patterns. An evaluation of these factors has implications for policy makers and dental public health professionals to develop programs for the improvement of oral health care. 9 This study, with a sensible sample of patients attending a free private dental center, provides important information on the prevalence of oral conditions, demographic parameters, and systemic conditions. Aging and gender are dramatically changing the population profile of developed and developing countries 10 ; therefore, we used these as predictor variables to study their association with oral conditions in this study. Findings of this study regarding sociodemographic variables, systemic factors and oral health status are comparable with other similar studies.2,4,6,11-17 These studies have reported poor oral health in different populations (India, Brazil, Rhode Island, and the USA) of the world. This study confirms findings of these studies by presenting poor oral hygiene, high dental caries, less fillings, more gingival and periodontal diseases, but low tooth loss level.
A majority (52%) of this sample was noneducated, many more females and males belonged to the low-middle class. In a recent study, 18 individuals from lower-income and -education groups consistently experienced higher burdens of untreated dental decay and poorer self-rated oral health. Females were more conscious of their oral health, thus showing a major representation in this sample. Demographic and clinical characteristics of 23% children and adolescents of this study are comparable with those of other studies.6,19, 20
The percentage (52%) of patients of this study with poor oral hygiene is in concordance with 43% of patients observed by Vadavadagi et al. 11 In this study, males of had poor oral health than females, which is in concordance with a study by Lintula et al. 21 Prevalence of calculus (73%) and gingivitis (66%) among adolescents in this study is similar to a current study from Saudi Arabia that reported moderate to high calculus and gingival bleeding among children. 22 A Spanish study has reported calculus prevalence at 59.3% in the adult population. 23
Low periodontal disease status of this study is comparable with that of another study 24 ; however, the relationship between an individual’s age and periodontal disease is still imprecise 4 ; a steady increase in periodontal disease with aging was observed in this study. Gender difference in periodontitis status in this study was insignificant (P = .081), with females showing a slightly higher level, whereas the study on the Spanish population has shown significant gender differences, with males showing higher levels. 23
Age was noted as the strongest predictor of dental caries, tooth loss, and periodontal disease in this study. Dental caries and tooth loss are important oral health indictors for adults and key measures for monitoring progress toward oral health promotion goals. 25 The global prevalence of caries among 6-year-old children is decreasing; however, considerable variations among children in different countries are observed. 26 A study in China has reported 55% (DMFT 2.7) prevalence of dental caries in children aged 5 years. 27 This study revealed an extremely high prevalence of caries among children at the age of 6, that is, 2 to 3 times higher than in Western Europe, but similar to the findings from developing countries.28,29 A Russian study 26 has reported on an average 5.48 decayed teeth, 0.44 missing, and 0.79 filled teeth; the present study has shown 78% caries prevalence, on average 1.79 decayed, 0.32 missing, and 1.04 filled teeth. High caries trend in this study may be due to modernization or increased use of junk foods in developing countries like Pakistan. Women show fewer dental caries, as reported by few studies,10,30 whereas Kida et al 31 reported high caries prevalence in women, and a similar high level of caries is noted in this study.
In terms of untreated decay, this study conforms to another study, 4 with men having fewer fillings. Women pay more attention to their oral health.32,33 The proportion of unmet restorative needs for the population of a study 6 was 60%, and this finding conforms to this study. Another study by Al-Haddad et al 34 has also confirmed high need for restorative treatment, noting significantly higher need in females. Batista et al 35 have explained the association of untreated caries and poor oral health with low oral health literacy, which conforms to low education status of the participants of this study.
Thirty-seven percent of this study sample had tooth loss (mean 1.04 ± 2.94), which conventionally increased with age. This finding is comparable with findings from other studies, such as mean levels of 2.2 ± 2.6 reported from Tokyo 36 and 57% from Rhode Island. 16 The study by Vadavadagi et al 11 on patients aged 18 to 35 years attending a teaching dental institute in India reported a tooth loss in 75%. The present study also shows a highly significant association between gender and missing teeth that are similar to findings from other studies.11,37 In India, 14 16.5% of 5- to 10-year-old children have shown tooth loss with no gender difference, in comparison with 5% in this study. Age, gender, low family income, and rural residence have been associated with tooth loss, with women showing more teeth loss.26,38,39 Age is the most commonly reported factor associated with missing teeth; older people have exhibited more missing teeth,40,41 and the likelihood of having this risk factor increased with extent of tooth loss was maintained among middle-aged and older adults in this study, which is also in consonance with a study reported by Urzua et al. 42
Functional dentition observed in this study does not conform to another report from a developing country. 43 Demographic determinants are associated with functional dentition. 15 This study shows that younger adults have more functional dentition than adults do. Epidemiologic data from Brazil indicated poor oral health, including high prevalence of edentulism, dental caries, and widespread tooth loss without prosthetic treatment. 14 Prevalence of oral conditions of TMJ dysfunction, oral lesions, prosthesis, malocclusion, and systemic factors of asthma, bleeding disorder, epilepsy, and pregnancy was very low (less than 2%) among this study sample and insignificant with respect to age and gender comparisons.
Although cross-sectional studies, as a measure of associations at one point in time has the inability to establish the causal relationship, but identify the factors associated with condition(s) under study4,15; therefore, findings of this study may be generalized to estimate the prevalence of oral disease in the Pakistani population. The association of sociodemographic determinants with oral health status and the role of oral health in quality of life have been imagined as a multidimensional field. 44 Therefore, considering the constant change in these determinants over life span and being very helpful in investigating potential causes of oral diseases, regular conduction of studies is warranted to understand the changing patterns of diseases within and between different populations.
Strengths and Limitations of the Study
With a reasonable sample size, this study provides a better understanding of the status of dental patients in Pakistan. A majority of patients were observed with unmet dental needs, a persisting issue in developing countries. Oral diseases show strong relationship with diabetes mellitus, cardiac disease, and hypertension. Being an observational study, this fails to show any causal relationship between study variables.
Conclusion
Age and gender remain strong predictors for both oral and systemic conditions. Poor oral health and tooth loss showed a strong relationship with chronic systemic conditions. Poor oral hygiene and dental caries were significantly higher in middle-aged groups, with periodontal condition and tooth loss aggravating with progressing age. Hypertension, diabetes, CHD, and hepatitis were significantly higher in females.
Footnotes
Ethical Approval
Use of record of dental patients for this study was approved by the UMDC administration vide letter # umdc-dc-178/17 dated 26 April 2017.
Acknowledgements
Services of dental staff and management of the University Medical and Dental College (UMDC) are highly acknowledged for supporting the study conduction.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.