
Abstract
Background:
Oral health is an integral part of general health. Good oral health helps people to communicate and enhances their dignity and personality. Oral health of soft drink factory workers depended on their working environment.
Aims and objectives:
To assess the oral health status and treatment needs of soft drink factory workers in Madurai city, Tamil Nadu, India.
Materials and methods:
A cross-sectional survey was conducted on 175 soft drink factory workers. Informed consent from the participants and ethical clearance were obtained. Data were collected by using WHO Oral Health Assessment Form for Adults, 2013.
Results:
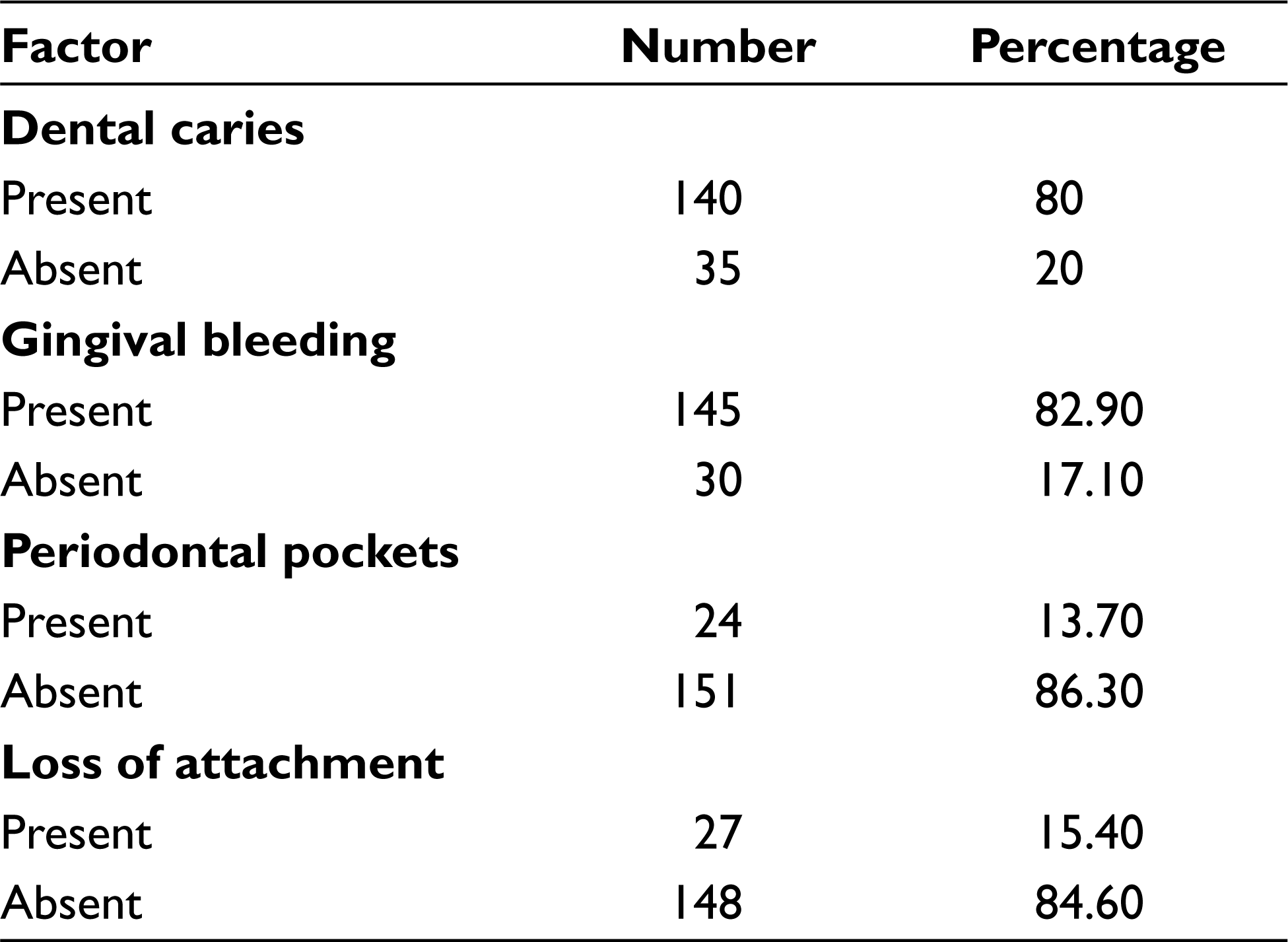
The result shows higher prevalence of oral problems with 80% dental caries, 82.9% gingival bleeding, 13.7% periodontal pockets, 15.4% loss of attachment, 54.9% fluorosis, and 50.9% dental erosion in soft drink factory workers.
Conclusion:
The study suggests that the oral health status of these soft drink factory workers is poor and there is an increased need for their dental treatment.
Introduction
Oral health is not only important to our appearance and sense of well-being but also to our overall health. 1 Oral health is an integral part of general health. It is a state of being free from disease, disorder, pain, and infirmity of oral and perioral region. Good oral health helps people to communicate and enhance their dignity and personality, thereby improving the quality of life. 2 Poor oral hygiene, tobacco and alcohol consumption, unhealthy diet, and working environment are considered as the risk factors for the poor oral health. Working environment is the sum of external conditions which influences the health of working population. This environment is responsible for the exposure of the hazardous materials and accidents. Occupational diseases are caused by a pathologic adaptation of the individual to his working environment. 3 Occupational acid exposure is limited to the battery and galvanizing (Zn–Al industry) workers, soft drink manufacturers, and dyestuff container cleaners. These factory workers are prone not only to health hazards but also to oral problems such as dental caries, periodontal disease, and dental erosion. 4 India contributes approximately 80% of the global burden of occupational disease because of improper industrialization in our country. 5
In recent years, there has been an increase in the consumption of soft drink in all age group leading to mushrooming of soft drink factories. Oral health among the soft drink factory workers is severely affected. They suffer from dental caries, periodontal disease, gingivitis, and tooth wear. 6 Consumption of carbonated beverages is considered as the risk factor for the gastroesophageal reflux disease (GERD) and regurgitation which leads to dental erosion. 7
Studies related to oral health of the soft drink factory workers are limited. In this study, an attempt was made to assess the oral health status and treatment needs of the soft drink factory workers in Madurai city.
Materials and Methods
The present study is a cross-sectional study, conducted to assess the oral health status and treatment needs of soft drink factory workers in Madurai city. Madurai city has many small-scale soft drink factories among which Vadipatti soft drink factory is considerably the bigger one. Hence, conveniently this factory has been selected for the study. This factory consisted of 175 workers. All the workers have been included in the study after getting their consent. The study was conducted for a week in the month of October 2017. The study was approved by the Institutional Review Board, Best Dental Science College (Ethical no: BDSC2772017). Written permission was obtained from the head of the factory to conduct the study in their factory before commencing the study. Informed consent from participants was obtained before starting the study. There were two inclusion criteria: (a) participants who were willing to participate in the study; and (b) soft drink factory workers who were above 18 years of old. The workers who had any systemic diseases, difficulty in mouth opening by any reason, and those who were not willing to participate were excluded from the study.
A self-administered questionnaire was used to collect the demographic data such as age, educational qualification, socio-economic status, medical and dental history, and oral hygiene practices. The level of health literacy among factory workers was not measured, neither was there a mention of educational level through frequency distribution. To avoid self-administered questionnaire misinterpretation and to maintain universality of questionnaires response, the investigator asked questions to the participants in their local language like an interview.
After questionnaires, clinical examination was conducted by the investigator. The investigator was trained by a subject expert. Intraexaminer reliability was done to standardize the clinical procedures and to minimize the error which can occur during data collection. The intraexaminer reliability was 0.82 for caries diagnosis; 0.92, 0.9, and 1 were the values attained for the diagnosis of plaque, calculus, and bleeding on probing, respectively. The agreement for most assessments was expected to be 90%.
ADA Specification Type III examination was performed. The subjects were seated comfortably on an ordinary chair and examined using natural light. Oral examinations were conducted using a plain mouth mirror and a CPI-probe. The examinations were carried out without cleaning or drying of the teeth and the instruments used consisted of a number 4 plane dental mouth mirror, dental tweezers, and a specially designed lightweight CPITN-C probe (clinical). The oral health status was assessed using WHO Oral Health Assessment Form, 2013. All the examinations were carried out under aseptic condition. 8
Statistical Analysis
The collected data were compiled. Data analysis was done with the help of computer using Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, version 22.0 for Windows). A p-value less than 0.05 denotes significant relationship. Since it is a descriptive data only, frequency distribution has been mentioned.
Results
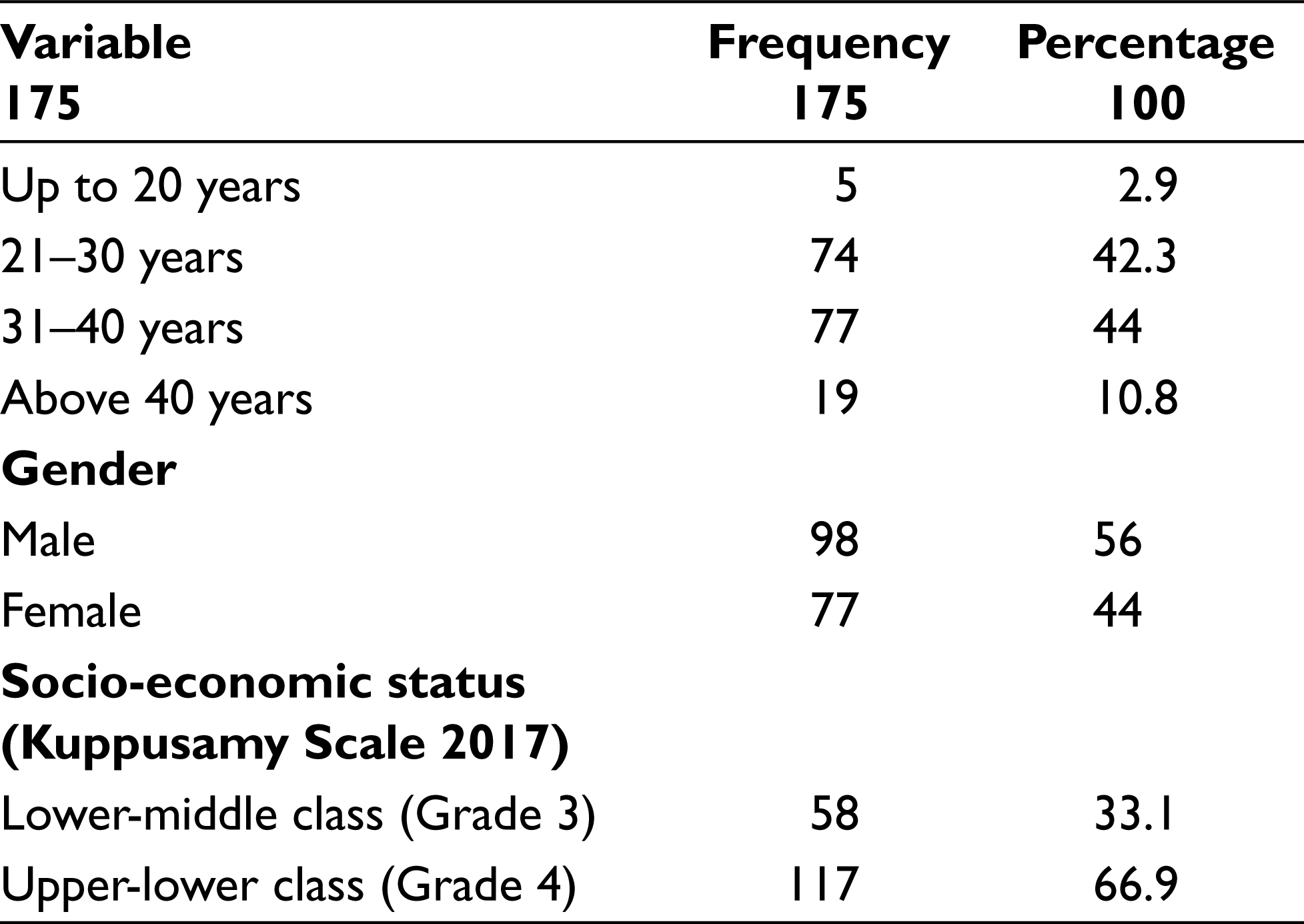
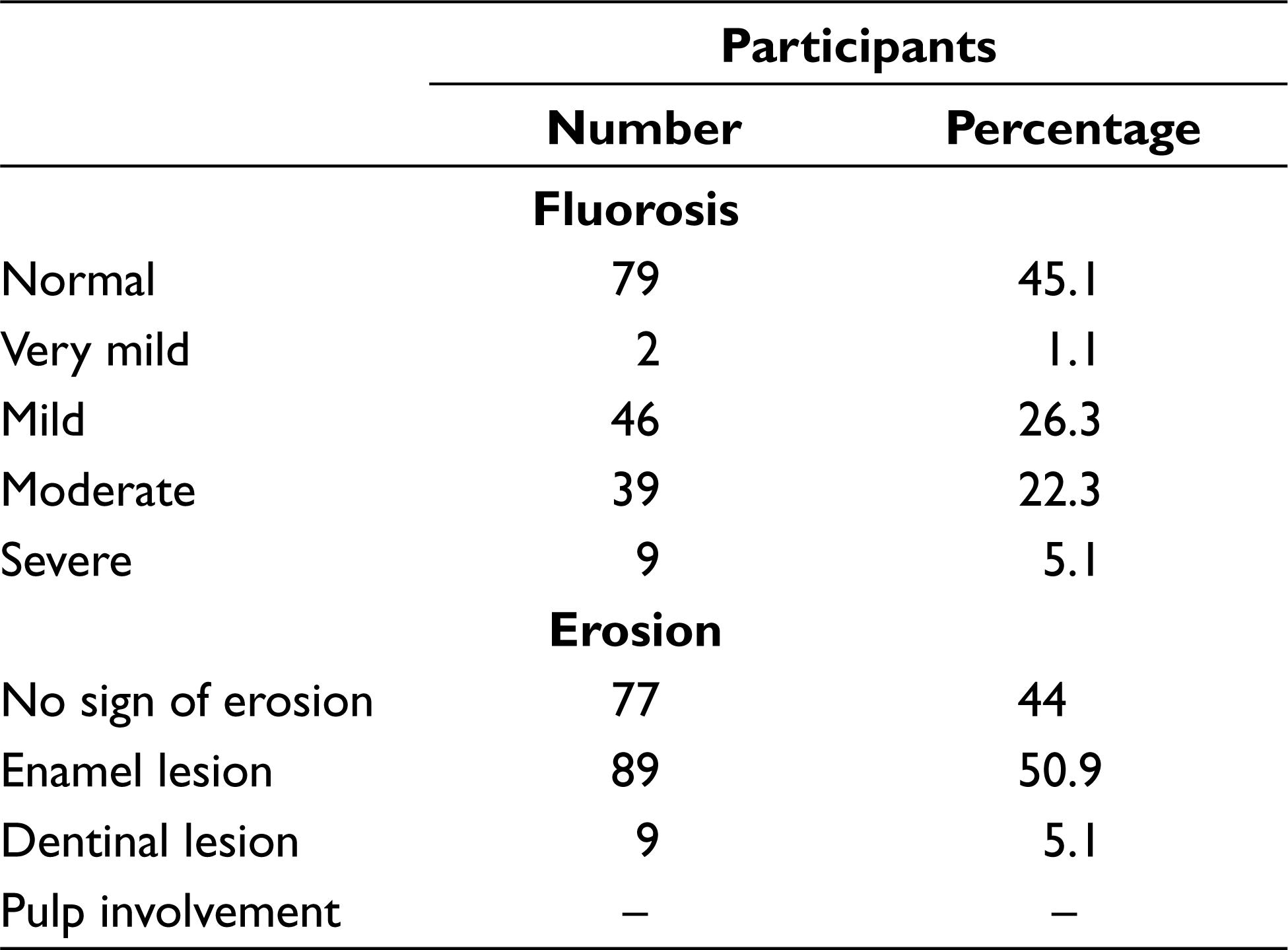
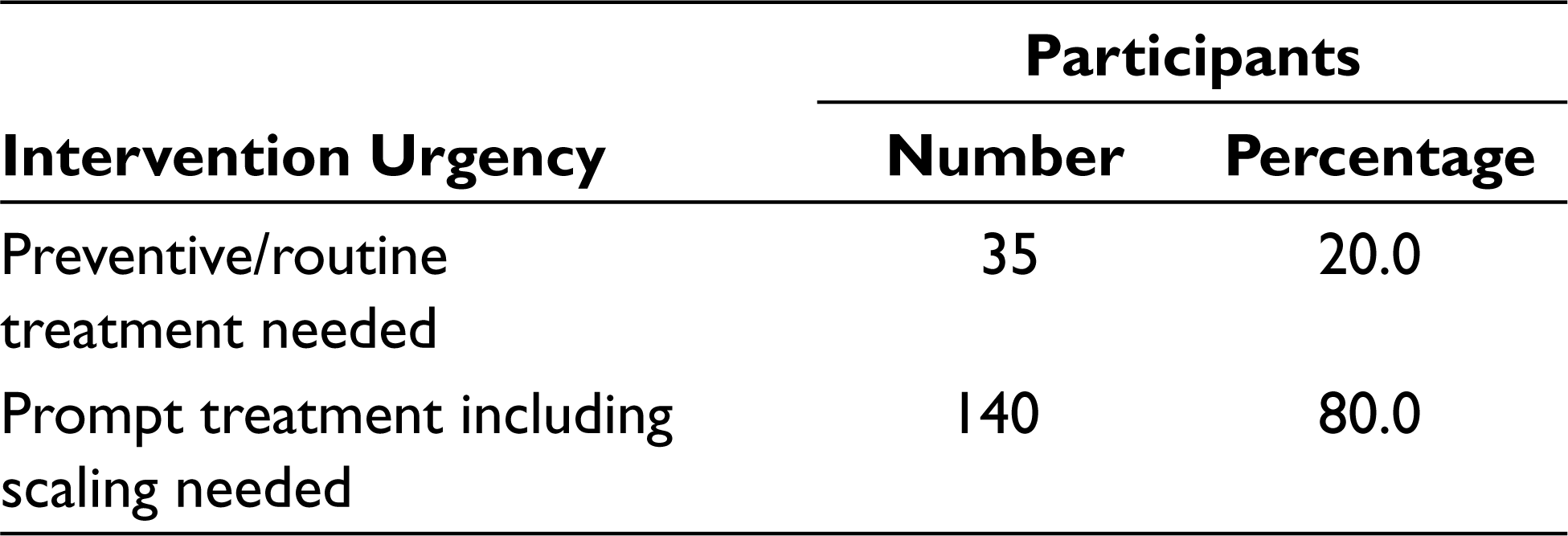
Majority of the workers in this study were in the age group of 31–40 years (44%). Most of the study participants belonged to upper-lower class (66.9%; Table 1). The study shows that 140 participants (80%) out of 175 were affected by caries. About 82% of the participants were affected by gingival bleeding. In regard to the periodontal pockets and loss of attachment, 13.7% and 15.4% of the participants were affected, respectively (Table 2). An assessment of dental fluorosis on the workers revealed that 45.1% (79) were affected by normal level of fluorosis, 1.1% (2) were affected by very mild level of fluorosis, 26.3% (46) were affected by mild level of fluorosis, 22.3% (39) were affected by moderate level of fluorosis, and 5.1% (9) were affected by severe level of fluorosis (Table 3). About 50.9% (89) of the participants were affected by enamel erosion (Table 4). A majority (80%) of the participants needed prompt treatment and scaling and the remaining (20%) required preventive measures.
Demographic Details Among Soft Drink Factory Workers in Madurai
Oral Health Status Among Soft Drink Factory Workers in Madurai
Dental Fluorosis and Dental Erosion Among Soft Drink Factory Workers in Madurai
Intervention Urgency Among Soft Drink Factory Workers in Madurai
Discussion
Workers or laborers form a major portion of population in any country. It was estimated by World Health Organization in the year 2007 that the global labor force was half of the world’s population (about 3,300 million). The officially registered working population includes 60%–70% of the world’s adult males and 30%–60% of the world’s adult females. 5
Many occupations expose the workers to hazardous working environments such as acids, chemicals among battery and galvanizing (Zn–Al industry) workers, munitions manufacturers, soft drink manufacturers, and dyestuff container cleaners. In recent years in India, there has been an increase in the consumption of soft drink in all age groups, directly leading to increase in factories manufacturing soft drinks. Occupational acid exposure in factories might also increase the risk of dental caries and dental erosion. 6
The present study was undertaken as an attempt to describe the prevalence and nature of oral health problems among workers in soft drink factory in Madurai city. Literature review revealed limited studies in this area, thus comparison is limited. The survey comprised of all workers in soft drink factory with a response rate of 100%. 6
In the present study, a total of 175 factory workers were included. The sample consisted of 98 males (56%) and 77 females (44%) with age ranging from 20–45 years. This distribution is similar to a study conducted by Sandeep Kumar et al 6 which had 51% male and 49% females wherein the majority belonged to low-income group with primary education, 9 which is in line with the current study where the majority (66.9%) belonged to lower-upper class. The dentition status was recorded using WHO proforma (2013). According to it, the prevalence of dental caries in soft drink factory of Madurai is 80%. In a study conducted in India by Rajkumar Maurya et al, the prevalence of caries was 67% and the mean DMFT was 4.09. Decayed teeth had the highest DMFT index of 67%. 10 A previous study suggested high prevalence of caries which was probably due to frequent exposure to sugar-sweetened soft drink and inadequate oral hygiene practices. The present study result shows high prevalence of periodontal disease among the study population with gingival bleeding among 82.9%, periodontal pockets among 13.7%, and loss of attachment among 15.4%, which could be as a result of inadequate oral hygiene maintenance due to lower literacy rate.
Sudhashu Sanadhya et al shows that severe fluorosis was the most prevalent (n = 232; 23.7%) form of dental fluorosis observed among the study subjects. Only 5.5% of the participants had questionable fluorosis. A significant relationship between dental fluorosis and gender was evident (p = 0.001). Females had a significantly greater prevalence of dental fluorosis (71.7%) as compared to males. 11 In the present study, the dental fluorosis prevalence (n = 175) among the study participants was 54.9% among which 1.1% (2), 23.4% (41), 22.9% (40), and 5.7% (10) had very mild, mild, moderate, and severe level of fluorosis, respectively. The high prevalence of dental fluorosis and lower mean dental caries score can be attributed to the water fluoride concentration in the area which range from 0.28ppm to 3.6ppm.
Kumar et al shows that workers working in these small-scale soft drink industries were regularly consuming soft drinks. Studies have also shown higher prevalence of dental erosion among people consuming soft drinks frequently. 9 The present study shows that the prevalence of dental erosion is high in the soft drink factory workers. It reveals that 50.9% (89) and 5.1% (9) of the workers were affected by enamel lesion and dentinal lesion, respectively, which could have occurred due to exposure to carbon dioxide gas in the working environment and increase in the consumption of soft drinks among the workers.
Roman and Pop 12 shows that the most prevalent treatment need was oral prophylaxis, which is in accordance with the present study. It shows that intervention urgency for dental treatments needed preventive/routine treatment among 20% (35) of the workers and 80% (140) of the workers needed prompt treatment including scaling and restorations.
Limitation of this study include its convenience sampling from one soft drink factory. Future research should be done in large scale to assess oral health of such workers along with treatment protocols.
Conclusion
Prevalence of dental caries, gingival bleeding, dental fluorosis, and tooth erosion is high among the soft drink factory workers of Madurai city. Exposure to carbon dioxide gas is the reason for the development of dental erosion. High proportion of affected workers indicates hazardous effect of working environment. About 80% of the soft drink factory workers needed prompt treatment which includes scaling and restorations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.