
Abstract
Aim:
The aim of the study was to assess the oral health status and treatment needs among intellectually disabled (ID) people in Madurai city.
Objectives:
To evaluate the oral health status and treatment needs among ID people in Madurai city.
Materials and Methods:
A cross-sectional survey was conducted on 133 ID people obtaining training at special schools in Madurai. After obtaining the parental consent of the participants, oral health was assessed using World Health Organization (WHO) proforma 1997 and oral hygiene level was assessed using Simplified Oral Hygiene Index (OHI-S). Statistical analysis was done using Statistical Package for the Social Sciences (SPSS Inc., Chicago, IL, version 22.0 for Windows).
Results:
The result of the present study shows higher prevalence of oral problems in mentally retarded subjects with 31.6% periodontal disease, 49.6% dental caries, and 39.1% poor oral hygiene status, among the study participants.
Conclusion:
This study gives sufficient evidence to suggest that the oral health status of this disabled population was poor, and there was an increased unmet dental treatment needs.
Keywords
Introduction
Today’s children are tomorrow’s future. The choices we make while raising our children determines the outcome of our future. To give good future to children, the first and foremost thing is to provide good health. The overall health of the body is determined by the oral health. So it is essential to maintain the oral health of the children. To maintain the optimal oral health of a normal child, the parents face significant challenges in their daily life. Children need to be helped and taught about daily oral care, and they need to be brought to the dentist for regular check-ups, cleaning, and fillings or other dental treatment, if needed. The child’s age, developmental disabilities and/or special health care needs may make it difficult or impossible for a child to perform daily oral care for themselves. Hence, family members/caregivers may need to assist with or perform these tasks for them. 1 These challenges increase multifold, when a parent tries to optimize the oral health of a special child. Mental retardation (MR) has been defined by the American Association of Mental Deficiency (AAMD) as a deficiency in theoretical intelligence that is congenital or acquired in early life. The AAMD classifies retardation into four categories according to intelligence quotient (IQ): mild, moderate, severe, and profound retardation. An individual is classified as having mild MR, if his/her IQ score is 50–55 to about 70; moderate retardation, if his/her IQ score is 35–40 to about 50; severe retardation, if his/her IQ score is 20–25 to 35; and profound retardation, if his/her IQ score is below 20-25. Developmental disabilities can develop due to a variety of conditions which include cerebral palsy, Down’s syndrome, MR, autism, seizure disorders, hearing and visual impairments, congenital defects, and even social or intellectual deprivation. 2 The people with Developmental disabilities were also known as handicapped. The World Health Organization (WHO) has defined a handicapped person as “One who over an appreciable period is prevented by physical or mental conditions from full participation in the normal activities of their age groups including those of a social, recreational, educational and vocational nature.” 3 According to WHO estimates, individuals with disabilities comprise 10% of the population in developed countries and 12% in developing countries. This amounts to one member with disability per 7-8 households. Because of their special care needs, daily care of children with disabilities is different from that of children with normal abilities, who can usually manage their own oral health. 4
The recent NSSO report suggests that the number of disabled persons in the country is estimated to be 18.49 million, accounting for about 1.8% of the total population, while the mentally retarded population amounted to 0.44 million individuals. 5
The oral health needs of individuals with intellectually disabled (ID) are complex and may be related to underlying congenital or developmental anomalies as well as inability to receive adequate personal and professional care to maintain oral health. Research suggests that people with ID such as MR, are more likely to have poor oral hygiene and periodontal disease, and possibly more likely to have caries than people without ID. 7
Dentists today understand the need to learn the subject of MR, although it has been observed that very few children with this condition seek the services of the dental professionals. 8 The primary aim of dental services for disabled people should be to prevent dental diseases, which require proper planning and implementation of services. The oral health of the disabled may be neglected because of the disability condition, a demanding disease or limited access to oral health care. Moreover, because of their level of function and their limited ability to undergo an oral examination, the disabled present specific challenges when their oral health is assessed. 3
Lack of services to these segments of population is the actual matter to worry and is the major drawback of dental services. Literature on assessment of dental diseases for mentally disabled subjects is very scarce as compared to that of normal population. Hence, an attempt is made to assess the oral health status and to provide the concerned dental treatment needs for the ID people in Madurai city.
Materials and Methods
The present study is a cross-sectional survey intended to evaluate the oral hygiene status, dental caries, and periodontal status among ID people in Madurai. The study was conducted during the period of August 2017 to September 2017. It included people diagnosed with intellectual disability and who were obtaining training at school for disabled people. Prior to the study, a pilot study was conducted among 10 ID subjects to check the feasibility in the month of August 2017, and according to the pilot study, the necessary changes were done in the main study.
Madurai city has a total of 11 schools for special children, among that 3 are daily care schools and rest were residential schools. The current study included only the daily care schools. The schools included were Sai Ram Special School, Bethsan Special School, and Akash Special School having a total population of 140 subjects. All the subjects attending the schools and whose parents gave consent were included in the study. Subjects who were uncooperative and who were absent for long duration were excluded.
Ethical clearance was obtained from the Institutional Review Board, Best Dental Science College, Madurai (BDSC/27072017). The nature and purpose of the study was explained to the school authorities (correspondent, principal, headmaster/headmistress), and written permission was obtained to conduct the study in their institutions. The informed consent was obtained from the parents/guardians of the study subjects.
Prior to clinical examination, the demographic data was collected. All the clinical examination was conducted by a single trained and calibrated examiner. Type III clinical examination (ADA specification) was performed under day light, on a regular chair and total aseptic condition. The examiner examined about 25 people per day were examined. Oral health assessment was done employing the WHO proforma 8 1997 and Simplified Oral Hygiene Index (OHI-S). 9
Statistical Analysis
The information collected were recorded in a master chart. Data analysis was done with the help of computer using Statistical Package for the Social Sciences (SPSS Inc., Chicago, IL, version 22.0 for Windows).
Using this software, frequencies and percentages were calculated for qualitative variables. Means and standard deviations were calculated for quantitative variables significant relationship. Student’s unpaired “t” test and ANOVA were used to test the significance of difference between quantitative variables. “p” value less than 0.05 denotes significant relationship.
Results
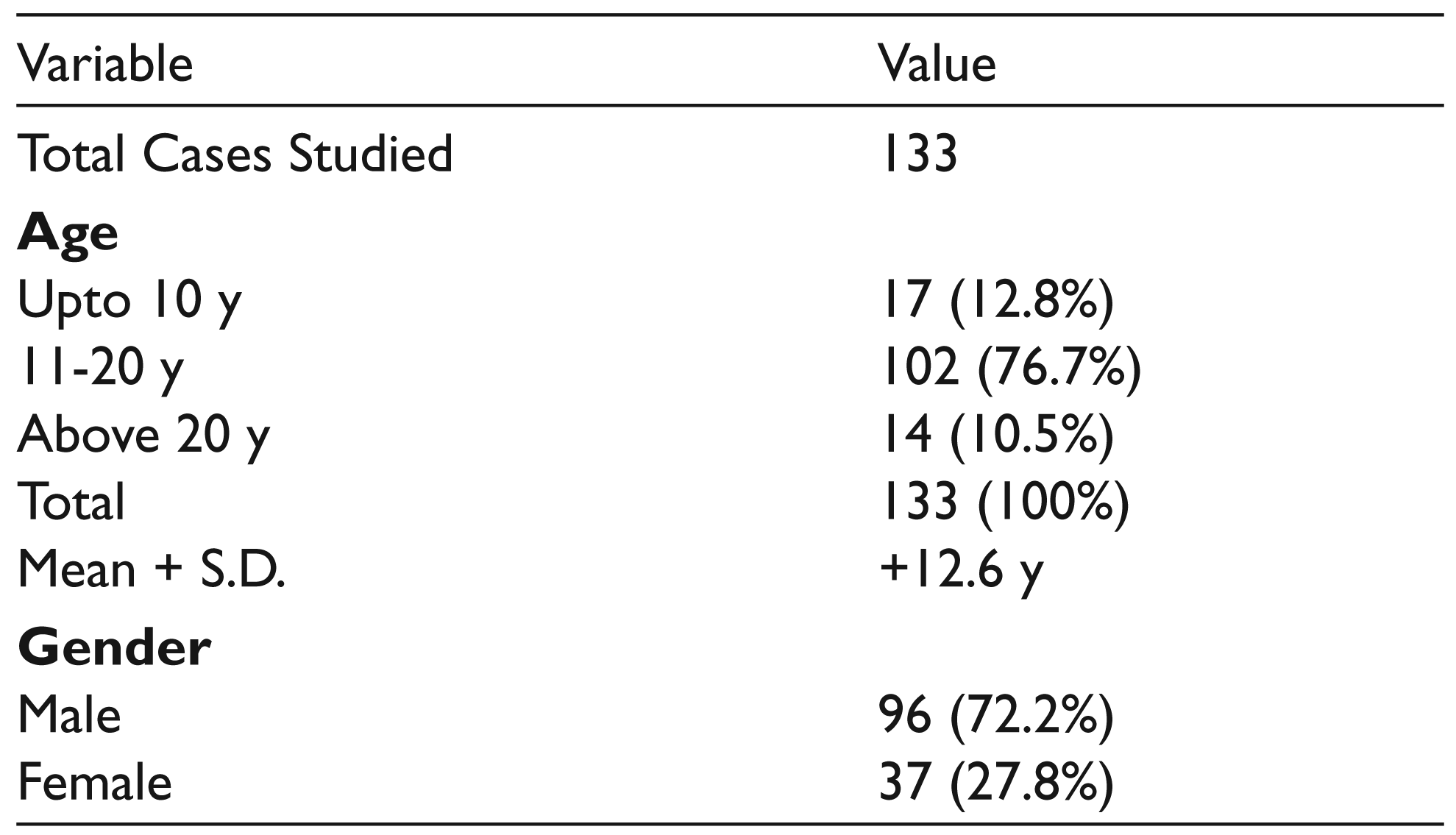
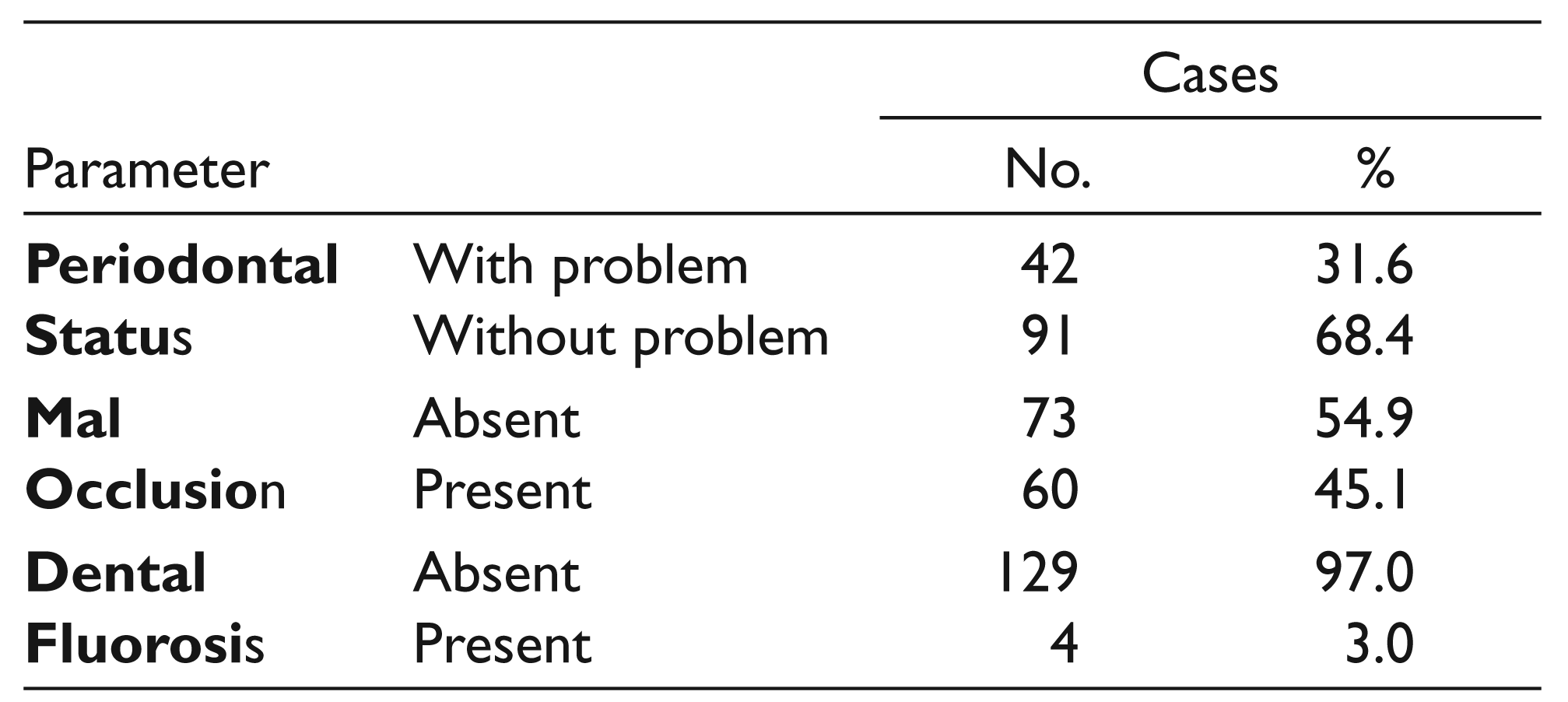
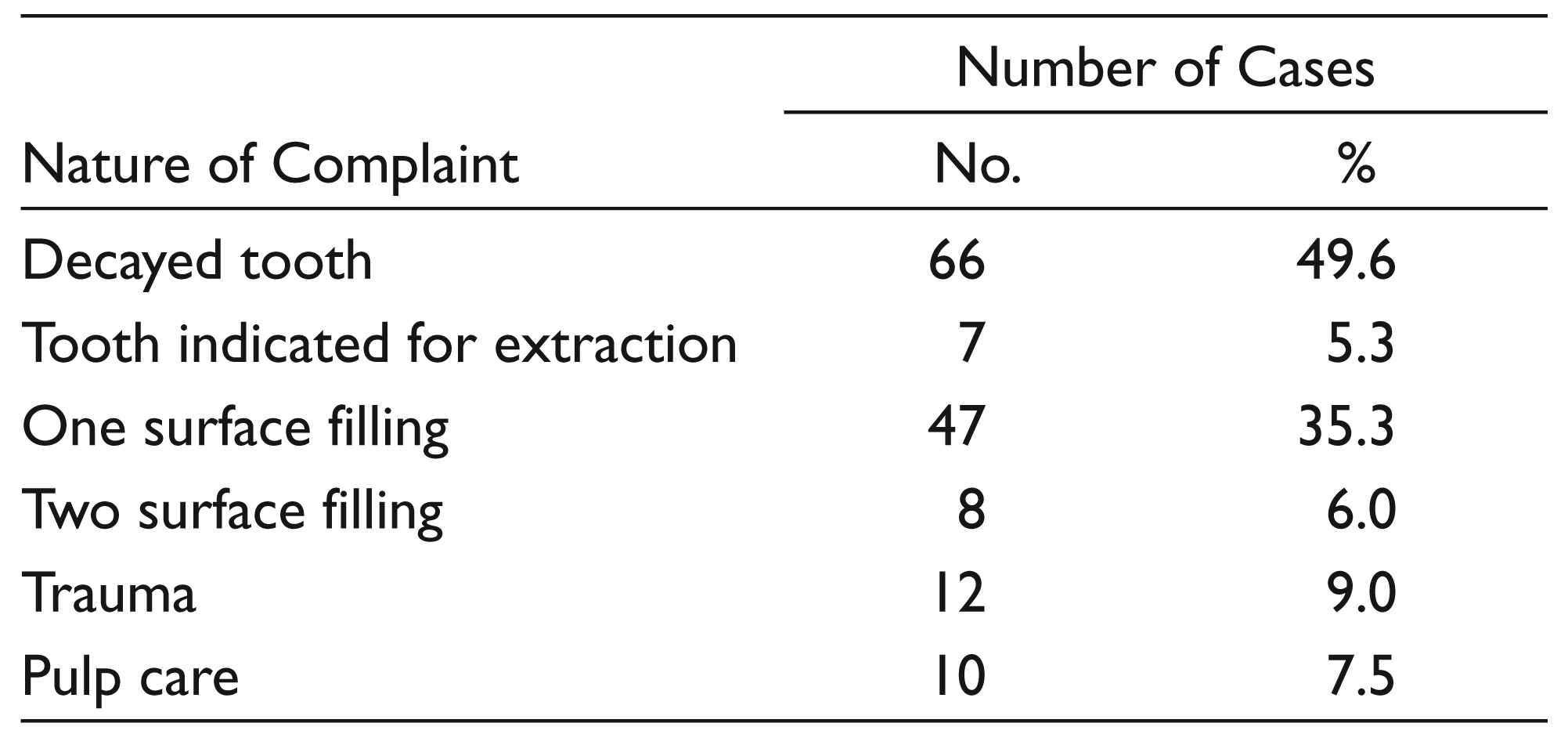
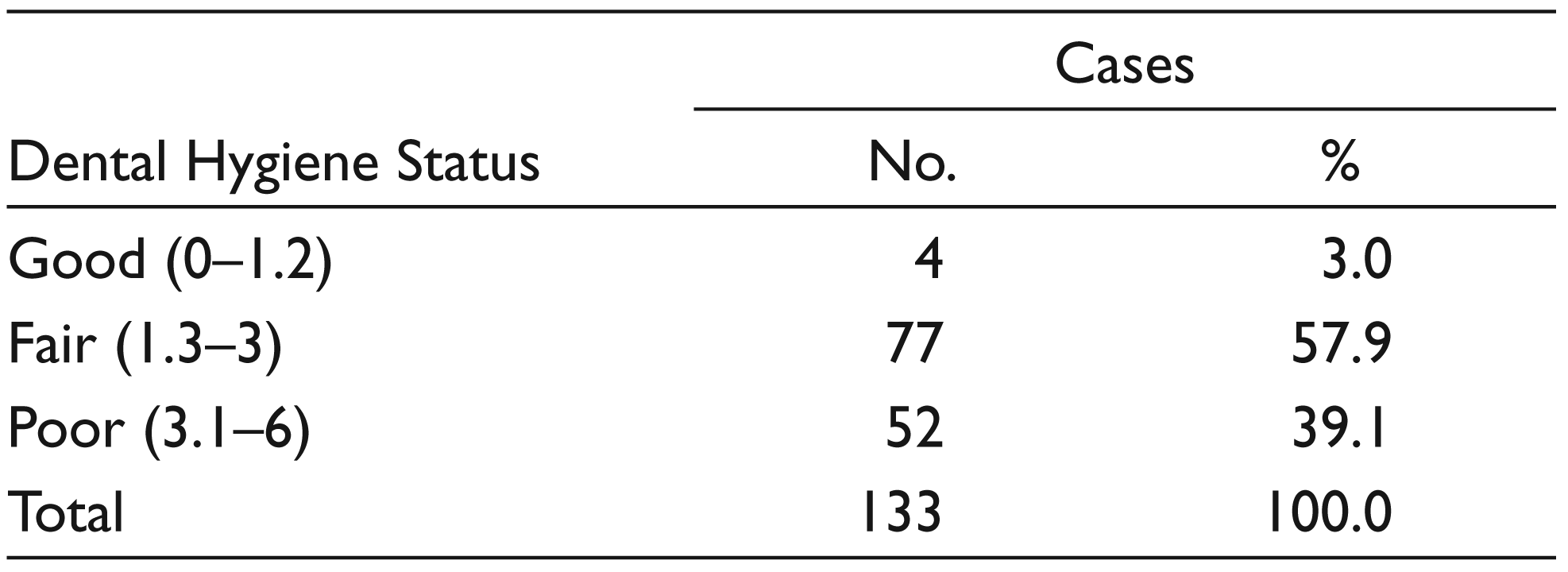
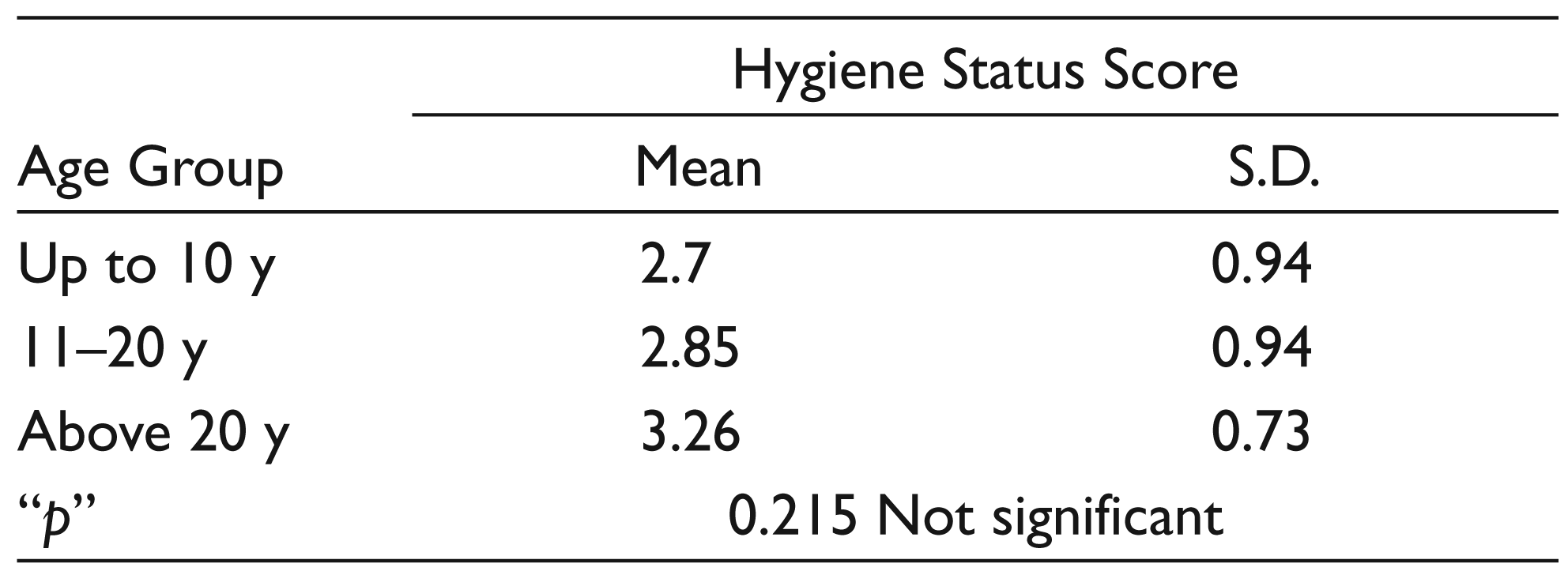
Table 1 depicts the demographic distribution of the study subjects. Majority of the subjects, 102 (76.7%), were 11-20 years old, the mean age was +12.6 years. The male subjects were 96 (72.2%) and the female subjects were 37 (27.8%). The study participants had normal extra oral finding and none of them had any enamel opacities. Table 2 shows the prevalence of periodontal status, malocclusion, and dental fluorosis. Almost all the study participants (97%) had dental fluorosis, whereas malocclusion and periodontal problems were observed among 45.1% and 31.6%, respectively. The dentition status and treatment needs are projected in Table 3.The prevalence of dental caries among the study subjects was 49.6%. Very few subjects required extraction, one surface filling, two surface filling, and pulp care therapy. Higher OHI-S score was observed among subjects above 20 years (3.26), but the difference was statistically not significant (p = 0.21) between different age groups. Majority of the subjects 57.9% had fair oral hygiene status followed by poor oral hygiene in 39.1%. No significant difference was observed between genders (Tables 4 and 5).
Demographic Distribution of the Study Participants.
Periodontal Status, Malocclusion and Dental Fluorosis Status of the Study Participants.
Dentition Status and Treatment Needs among the Study Subjects.
Oral Hygiene Status of the Study Participants.
Association Between Age and Hygiene Status Score of the Study Participants.
Discussion
Maintaining good oral health is particularly challenging among individuals with disabilities because of increased oral health risks due to underlying disease, limitations on access to care, and competing demands. The lack of oral hygiene has been implicated as a fundamental factor in the development of periodontal diseases and dental caries in ID subjects. Hence, the present study was conducted to assess the oral health status and treatment needs among the ID in Madurai. Majority of the studies were conducted in northern part of India, few study have been attempted in southern part of India. Hence, the present research was conducted in Madurai district, Tamil Nadu, and this was the first research among ID in Madurai. In the present study, daily care special schools were included to assess the oral health of the subjects from the natural home set-up. The important findings of the present study was that the ID subject had poor oral health status with the fair oral hygiene status of 57.9% and poor oral hygiene status of 39.1%. The previous study done by Bhowate et al. 11 , in which he concluded that the fair clinical level of oral hygiene was 60% among the mentally challenged individuals, was in line with the present study where the fair oral hygiene was 57.9%. Jain et al. 5 and Jain et al. 4 reported poor oral health among the mentally retarded population which is in agreement with the present study. A study conducted by Anders et al. 7 concluded higher prevalence of periodontal disease among the ID people, which is in agreement with the present study where 31.6% of ID subjects had poor periodontal status. Bharathi et al. 6 conducted a study from which he concluded that there was high prevalence of malocclusion among the special school children (66.4%), which was in line with the present study (60%). In the previous study done by Kumar et al., 12 the dental caries present in the ID subjects was 89.2% which was very high when compared to the present study. In the study done by Karadag et al., 13 he included the parents of the ID children. In the study, he concluded that oral health status of the differently abled children was poor which is in line with the present research. In a previous study done by Diab et al., 14 he concluded that the preventive and treatment programs to improve the oral health status of institutionalized ID subjects are needed. Hatton et al. 15 states that greater attention should be given to the ID people in their day-to-day life. The limitations of the present study were autism and cerebral palsy people who were not included in the study, and only the daily care schools were taken into the study, residential schools were not included.
Recommendations
These schools can be adopted and treatment can be done for those who are in need of dental care.
Interventions can be given after the health education for the parents and caregivers, and the evaluation of improvement in oral health status can be done.
For future research: The residential special needs schools can be taken into the consideration.
Conclusion
The present study reveals the higher prevalence of oral problems such as periodontal problems, dental caries and poor oral hygiene among ID, and increased unmet dental treatment needs. It highlights that the ID people need extra care regarding the oral hygiene, which can be achieved by educating the teachers, parents, and caregivers of the ID people. Health professionals should be aware of the impact of mental illness on oral health. Health professionals should support and provide all positive services to this population.