
Abstract
Aims and Objectives:
To assess the perception, practice, and attitude about dental ergonomics among dental students in Chennai.
Materials and Methods:
The study was carried out among 148 dental students in Chennai, Tamil Nadu, using a self-made validated closed-ended questionnaire.
Results:
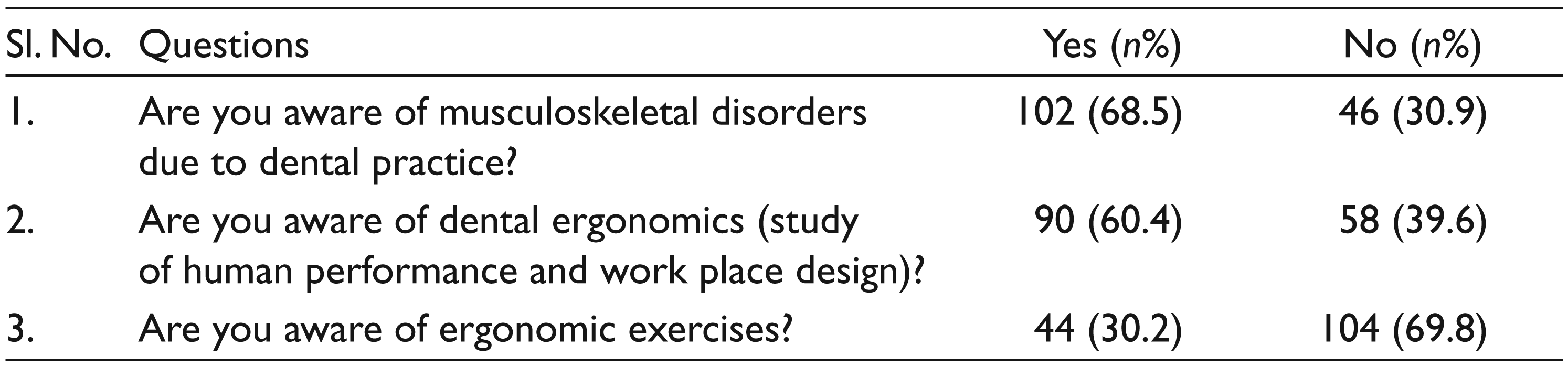
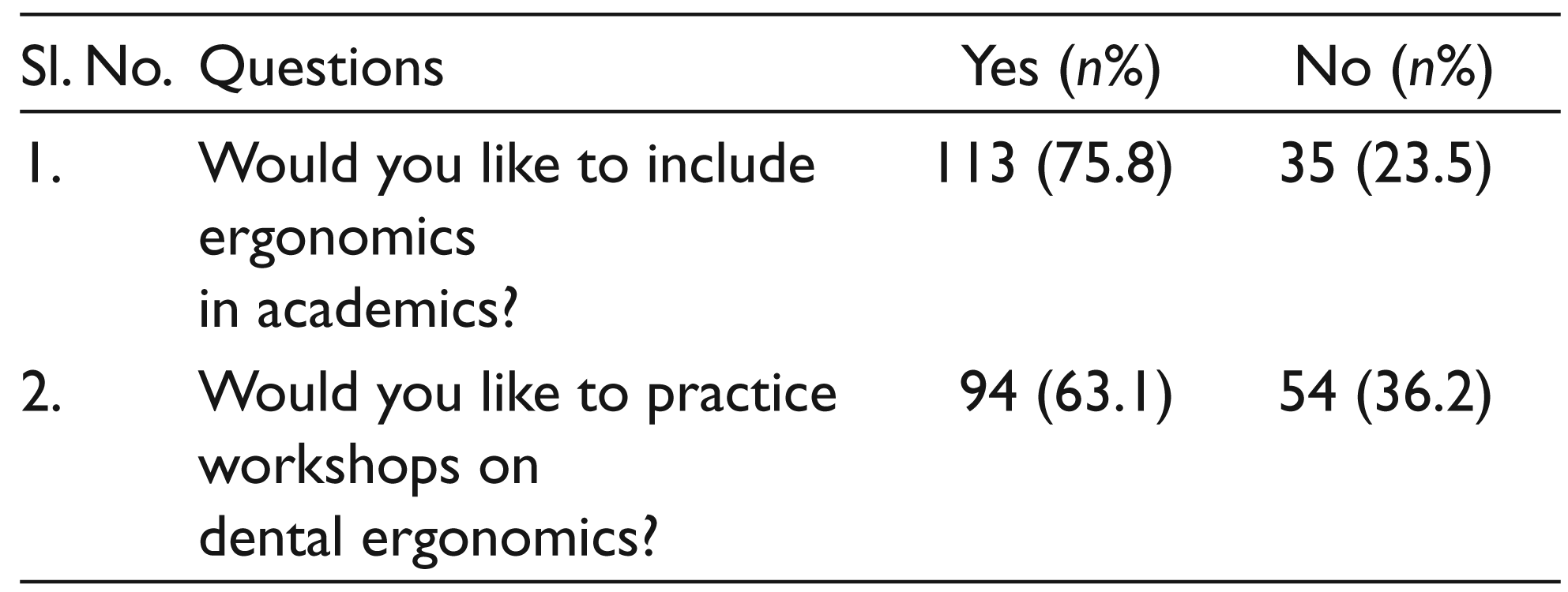
Among 148 dental students, 75 (50.6%) were undergraduate and 73 (49.4%) were postgraduate students. Of the study population, 38 (25.67%) had listed their general health problems which they thought were related to their profession, 102 (68.5%) were aware of musculoskeletal disorders, 90 (60.4%) were aware of dental ergonomics, and 104 (69.8%) were not aware of dental ergonomics. Of the dental students, 55% practiced both sitting and standing dentistry, and 43% of them practiced sitting dentistry alone. Only 22.8% of the dental students practiced 4-handed dentistry and 38.3% of them, who did not practice 4-handed dentistry swiveled themselves to face the area. A total of 113 (75.8%) dental students suggest to include dental ergonomics in their academic curriculum and 94 (63.1%) wanted to practice workshops on dental ergonomics.
Conclusions:
A majority of the dental students in this present study were aware of musculoskeletal disorders and dental ergonomics, but only a considerable number of them practiced dental ergonomics. This study recommends the need for including dental ergonomics in the academic curriculum.
Keywords
Introduction
The foremost priorities for dental professionals are to promote oral health and provide dental treatment in a safe environment. While treating the patients, dentists work with great precision in very small congested areas, under conditions where access to teeth for treatment procedures is very difficult, on a patient who is usually quite tense and nervous. These factors often lead the dentists to work in bad positions with tense muscles. Large bodies of literature1-6 show a relatively high prevalence of musculoskeletal disorders (MSDs) among dentists. The World Health Organization defines MSD as
A disorder of the muscles, tendons, peripheral nerves or vascular system not directly resulting from an acute or instantaneous event (eg, slips or falls). These disorders are considered to be work-related when the work environment and the performance of work contribute significantly, but are only one of a number of factors contributing to the causation of a multifactorial disease.7,8
Types of MSDs reported commonly among dental professionals include back problems,1,4 neck,2-4 shoulder,2-4 and hand and wrist problems 1 (carpal tunnel syndrome, 5 Guyon’s canal syndrome, de Quervain’s disease, and trigger finger). 6
Ergonomics is the science of setting the workplace and job demands, according to the capabilities of the working population. Dental ergonomics, when applied properly, ensures a major reduction in the prevalence of MSDs among dental professionals. 9 This study was undertaken with the aim to assess the perception and practice of dental ergonomics among dental students in a dental college and to suggest necessary preventive measures to develop MSD in their practice.
Materials and Methods
The present study was carried out among 148 dental students in Chennai, Tamil Nadu, India. Ethical clearance was obtained from the Institutional Review Board of Ragas Dental College and Hospital (RDCH /IHEC/Study No. C18), Chennai, Tamil Nadu, before the start of the study. A self-made validated closed-ended questionnaire was used for the study. The questionnaire comprised of 6 general questions (about age, gender, year of study, health problems participants have encountered in past years which they think are related [caused/aggravated/maintained] to their work as dentist, number of clinic hours they work per day, and whether they are right- or left-handed), 4 questions on knowledge (awareness about MSDs due to dental practice, dental ergonomics, ergonomic exercises, and ergonomic operator stool), 3 questions on attitude (including ergonomics in academics, attending workshops on dental ergonomics, and following ergonomic principles), and 8 questions on practice which focus on ergonomic principles while treating patients in clinical practice.
A pilot study was carried out to validate the questionnaire among 25 students before the start of the study. Face validity was checked by 5 professionals, and modifications were made in the questionnaire as per their suggestions. Internal consistency was also tested, and the Cronbach α value was found to be 0.86. The data collected in the pilot study was not used for the main study.
The questionnaire was distributed to the final-year undergraduates, house surgeons, and postgraduates in clinical departments at Ragas Dental College and Hospital, and the data was collected. The purpose of the survey was explained to the participants, and those who were willing to participate were alone included. Informed consent was obtained before the start of the study. The data collected was entered in a Windows Excel spreadsheet and the frequency distribution of the data was calculated.
Results
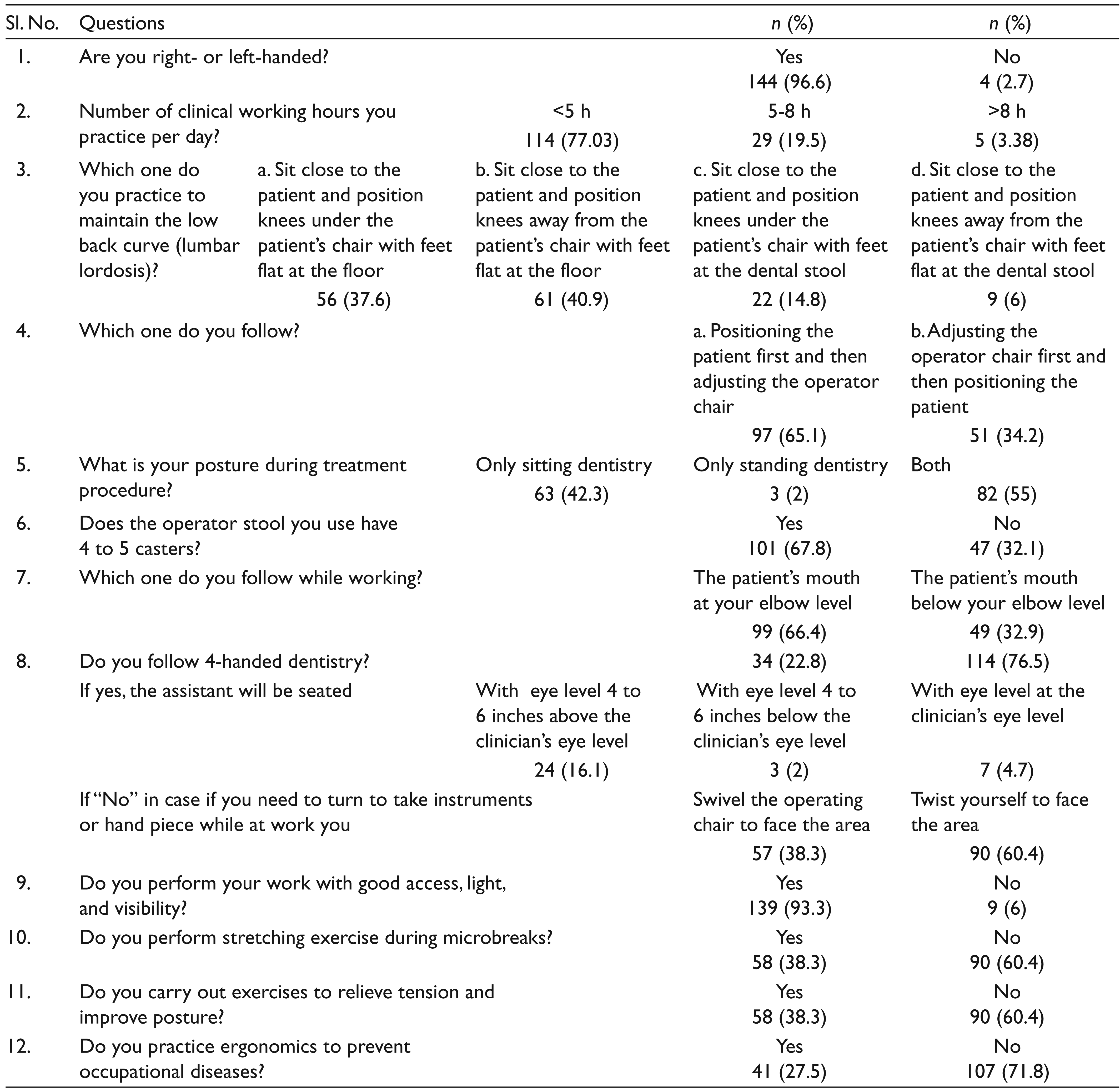
The mean age of the study population was 24.5 ± 3.7 years. Out of 148 participants, 67 (46%) were males and 81 (54%) were females. A total of 75 (50.6%) were undergraduate dental students and 73 (49.4%) were postgraduate dental students. Of the study population, 38 (25.67%) had listed general health problems that they encountered over the past years, which they thought were related (caused/aggravated/maintained) to their profession. Of those, the majority, 14 (9.45%), complained of neck pain followed by 6 (4.05%) who complained of back pain. Of the total participants, 144 (97.30%) practiced right-handed dentistry and 4 (2.70%) left-handed dentistry. Of the study group, 114 (77.03%) spent less than 5 clinical working hours, 29 (19.59%) spent 5 to 8 hours, and 5 (3.38%) spent greater than 8 clinical working hours. Of the study population, 63 (42.3%) practiced only sitting dentistry, 82 (55%) both sitting and standing dentistry, and 3 (2%) only standing dentistry. A total of 98 (66%) of the dentists first positioned the patient and then adjusted the operator stool. Of the dental students, 101 (67.8%) used the operator stool with 4 to 5 casters.
Of dental students, 99 (66.89%) placed the patients’ mouth at their elbow level while treating the patients. Only 22.8% of the study population followed the 4-handed dentistry, of which 16.1% made their assistants sit with their eye level 4 to 6 inches above the clinician’s eye level. Of those, who did not follow 4-handed dentistry, 38.3% swiveled the operating chair in case they needed to turn to take instruments or a handpiece while at work and 60.4% twisted themselves to face the area.
Tables 1, 2, and 3 show the dental students’ perception, practice, and attitude about dental ergonomics, respectively.
Perception about MSDs and Dental Ergonomics
Clinical and Dental Ergonomics Practice among Dental Students
Attitude about Dental Ergonomics among Dental Students
Discussion
Research studies1-6 highlight a higher prevalence of work-related MSDs among dental professionals and dental students. Occasional backache or neck ache is not a cause for alarm, but if there is regularly occurring pain or discomfort and if it is ignored, the damage can lead to an injury or a career-ending disability. In India, according to the Dental Council of India norms, dental students are exposed to clinical work in their third year of the dental degree course. 10 Dental students start performing general dentistry procedures such as scaling, restorations, extractions, and prosthetic replacement of missing teeth from the third year without the use of a dental assistant. All auxiliary procedures such as maintaining the sterile work area, mixing dental materials, and X-ray processing are performed by the students alone. The nature of their work might result in MSDs in many parts of the body depending on the location and the type of work they perform. In dental colleges, where the study is conducted, the dental equipment consists of adjustable doctor’s stool with 4 to 5 casters, an adjustable patient treatment dental chair, which can be elevated and reclined for treating patients, and an overhead operating light that can be placed for proper visualization as needed at various angles. Hand instruments and dental materials are positioned and retrieved in front of the dental students. Students are trained sitting dentistry and standing dentistry.
While standing, the human spine when viewed from the side has 4 natural curves as follows: cervical lordosis, thoracic kyphosis, lumbar lordosis, and sacral kyphosis. These curves are interdependent. Any change in 1 curve will change the curve above or below it. The sacral curve movement is limited as it is composed of 5 fused vertebrae. The lumbar and cervical curves are more mobile and can be damaged more easily. When these curves, especially the lumbar curves, get flattened or exaggerated, the spines have to depend on muscles, ligaments, and soft tissues to maintain erect, causing tension in these structures, and also causes the nucleus in the spinal disk to migrate posteriorly toward the spinal cord. In the later stage, the posterior wall of the disk will become weak, resulting in disk herniation. 11 Hence, dental students and dental professionals should know about strategies they can use to maintain the natural curves.
Studies12,13 reveal that dentists who practice sitting dentistry alone experience severe low back pain than those who practice both standing and sitting dentistry alternatively. In the present study, it is found that about 55% of the dental students practice both sitting and standing dentistry, and 43% of them practice sitting dentistry alone. Some clinical departments where dental screening, dental restorations, and oral prophylaxis are done, the students are made to sit and treat patients, and other departments where minor surgical, tooth impression procedures are carried out, the students are made to stand and treat the patients. Treating patients in a standing posture uses different muscle groups than that in a sitting posture. Alternating between these 2 positions will let one group of muscles to rest while other group of muscles work. Hence, alternating between sitting and standing postures will be effective in preventing muscle injuries.
Sitting posture problems can be avoided by adjusting the operator stool first and then adjusting the patient’s chair. 11 One common mistake dental professionals make is that they make the patient sit and adjust the patient’s chair first and then adjust their stool to accommodate their patients. This is seen in our study with 66% of the dental students adjusting the patient’s chair first and then their operator stool. They are being either trained with this practice or they are not aware about the hazards of the improper adjustment of the operator stool.
The present study shows that only 22.8% of the dental students practice 4-handed dentistry, and 38.3%, who do not practice 4-handed dentistry, swivel themselves to face the area. Dental students have to work in precision without the use of any dental auxiliary. The operatory design makes the dentist to perform extensive trunk twisting movements and shifting vision to retrieve instruments. For the dental students, 4-handed dentistry can be encouraged by making the dental assistant sit at 4 to 6 inches above the clinician’s eye level.11,14 If in case this is not possible, the dental students should be informed to position the instruments within easy reach, and if in case the treatment procedure involves the dental students to turn to retrieve instruments or handpieces, the dentists should swivel their dental stool to face the area rather than twisting their trunk. 11
Forward heard posture is common among dentists as a result of holding their neck and head in an unbalanced forward position for better visibility during dental treatment. This affects the cervical lordosis curve; the vertebrae cannot support the spine properly, and the muscles of the cervical and upper thoracic spine have to contract constantly to support the weight of the head. This can result in tension neck syndrome. 15 Use of magnification systems like operating telescopes or loupes will decrease neck and low back pain, as they help dental operators to maintain healthier postures.11,16 Dental students in dental colleges are not introduced and encouraged to use these magnification systems. The reason might be an increase in the cost of operating telescopes or lack of awareness about MSD caused by the posture.
Studies17,18 show that maintaining lumbar lordosis while sitting will reduce low back pain. This can be achieved by tilting the dental operators stool seat angle about 5° to 15°. This will place the hips slightly higher than the knees and allow closer positioning to the patient. Chairs that cannot be tilted can be replaced by an ergonomically designed wedge-shaped cushion. 11 In dental colleges where this study was conducted, the operator stool was adjustable upward and downward, but the tilting of the chair was not possible. This can be a reason for the dental students to experience pain or discomfort for the past one year.
Sitting closer to the patient and positioning operator’s knees under the patient’s chair, if possible, will also help in maintaining low back curve. 11 This can be possible by using a saddle style operator stool. 19 However, in an academic setup where such ergonomic stools are not available, the dental students can be trained to adjust the chair so that their hips are slightly higher than their knees and their weight is distributed evenly by placing their feet firmly on the floor. Only 14.86% dental students in this study sit close to the patient, positioning their knees under the patient’s chair with their feet flat to the floor. It is found in this study that majority, that is, 41.22% of the dental students sit close to the patient and position knees away from the patient’s chair with their feet flat at the dental stool. Placing the feet at the dental stool while treating patients might be a cause for low back pain in 6 (4.05%) students.
Studies4,6,9 report that the increase in MSD among dentists may be due to longer work periods without breaks. It is difficult to avoid prolonged static postures by the majority of the dentists. Stretching exercises performed in the reverse direction of awkward prolonged static postures may prevent pain and MSDs.11,20,21 Stress can also cause muscular tension. Practicing stretching exercises during microbreaks 21 and yoga 22 daily to relieve stress can also reduce MSDs. About 60% of dental students do not practice it. The reason may be the lack of awareness about MSDs and measures to prevent it.
Researches5,18 conducted in the Indian scenario have reported a higher prevalence of full-time and part-time dentists. Research among dental students is limited. This study shows little light on the MSDs dental students encounter, with 25.67% of the dental students listing out general health problems that they have encountered in past years might be (caused/aggravated/maintained) due to their profession. However, larger studies in future, highlighting the prevalence of various MSDs among dental students, might alarm the dental community to practice preventive measures at the earliest. The major limitation of the study is including samples only from 1 dental institution.
About 69% of dental students in this present study are aware about MSDs among dentists. Approximately 61% are aware about dental ergonomics which was quite satisfactory. These results are in accordance with the studies conducted by Garbin et al 23 and El-sallamy. 24 More than 50% of the dental students practice dental ergonomics while treating patients.
An increase in the prevalence of MSDs among dental practitioners recommends the need of concentrating more on the practice of dental ergonomics. According to the syllabus proposed by the Dental Council of India, there is no disciplinary syllabus on ergonomics under both undergraduate and postgraduate syllabi. It will be better for future dentists if dental ergonomics gets included in the academic curriculum.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.