
Abstract
Aim:
This paper aims to develop the Turkish version of the dental environmental stress (DES) scale that can evaluate perceived DES in Turkish dental students.
Materials and Methods:
A methodological study was conducted to adapt the DES scale to Turkish language in Gaziantep University, Faculty of Dentistry. The study group consisted of 392 students in the academic year 2018/19. The students were surveyed using the DES scale, translated into Turkish language. The demographic characteristics were analyzed by using descriptive statistical analyses. Kaiser-Meyer-Olkin and Bartlett’s Test of Sphericity were employed to evaluate the suitability of the dataset. Exploratory factor analysis was performed to assess construct validity. Depression Anxiety Stress Scale-21 was used to predict the power of the scale. In reliability analysis, the instrument’s internal consistency and corrected item-total correlation, Cronbach’s α reliability were studied.
Results:
Content Validity Index of the scale items was found to have a high validity range of 0.97. Two items with an estimate value less than 0.4 were excluded and 30 items yielded five factor. Five factors having eigenvalues greater than 1.0 explained 52.299% of the total variance. Each factor showed adequate internal consistency. Factor loadings ranged from 0.46 to 0.77. In the concurrent validity, significant positive relationship was found between DASS-21 and Turkish DES.
Conclusion:
According to psychometric properties, the Turkish version of the DES presented good results, thus it could be a valid instrument to assess the perceived stress in Turkish dental students.
Keywords
Introduction
Dentistry is a highly stressful profession that attracts the attention of researchers. 1 86% of professionals are admitting their life to be very or fairly stressful. 2 The objective of dentistry faculties is to provide dentists of the future with sound theoretical knowledge as well as good clinical and human skills. Students are exposed to various stress factors in the process. 3 Dental students encounter noticeable stress throughout their education and experience higher levels of distress than the general public 4 because of the highly stressful nature of dental education. Earlier studies have already indicated a markedly high level of psychological disturbance among dental students. 5 In addition, intense interactions between the patient and the clinician may precipitate a state of burnout, consisting of depersonalization, reduced personal accomplishment, and emotional exhaustion. 4 Studies furthermore indicate that increasing stress may result in decreased performance by students; high levels of stress may also result in a wide variety of physical and psychological complaints. 4 Dental students are expected to acquire a range of competences, such as the acquisition of theoretical knowledge, clinical competences, and interpersonal skills according to the curriculum and become a liable dentist in the period of their education. 6
Numerous studies of a similar kind have been performed at various dental schools worldwide. Analogously, literature search revealed that undergraduate dental students around different countries show occupational stress. Stress factors affecting clinical students are reported to mimic the factors of dental practitioners. The majority of these studies have been carried out by means of surveys that utilize the dental environmental stress (DES) questionnaire and have reported significant increase in stress amongst dental students.7–9
The need for unique scales for specific groups is increasing day by day. Stress scales have been developed over the last two decades for professionals, students, and patients. The stress factors that dentistry students are exposed to were generally determined using the DES scale developed by Garbee et al. (1980). 10 Even though perceived stress of dental students is researched thoroughly, Turkish perspective has not been examined closely. The support levels of Turkish dentistry students were also determined using standard and nonvalid measurement tools such as Turkish translation of the questions of this scale in the form of a questionnaire and item addition and removal. This has led to different results, evaluations, and interpretations.
In the literature, there is no scale used to measure the stress experienced by Turkish dental students. Therefore, this study aims to develop a scale that can evaluate perceived DES in Turkish dental students and prove its validity and reliability in our society.
Materials and Methods
A methodological study was conducted to adapt the DES scale to Turkish language in Gaziantep University, Faculty of Dentistry. The data were collected between February and March 2019. The inclusion criteria were being a student in the dental faculty during the dates on which the study was conducted and being willing to participate. All of the students (392 students) of Gaziantep University, Faculty of Dentistry, in the academic term 2018/19 (80 are in their first year, 98 are in their second year, 81 are in their third year, 68 are in their fourth year, and 65 are in their fifth year) were involved. All the students were informed about the scope of the study and asked to participate voluntarily (n = 392). The students who were missing (n = 64) or who refused to participate (n = 20) were excluded. There was no evidence of sampling bias.
The questionnaire was filled in 20 to 25 min by the students agreeing to participate in the study after the necessary explanations were given to them (purpose of the study, confidentiality of answers, and general information about the form).
The study sample comprised of 308 students, of which 24 were in their first year, 86 in their second year, 70 in third year, 68 in fourth year, and 60 in their fifth year. The strength of the sample (308) to represent the population (392) was 78.5%.
The instrument consisted two sections. The first section verified sociodemographic details and the second section comprised of the DES scale, which assesses the sources of stress associated with undergraduate course work and dental students’ training. Because of the low performance of scales with multiple choice questions, we adopted a four-point Likert type response measurement design when preparing the response options.
Data Collection
An introductory information form was used to determine the demographic characteristics of the students. The item pool of the scale, which was developed to collect research data, was obtained from the DES questionnaire 11 used by Turkish dentistry students and the original DES scale 10 consisting 25 items in five-point Likert style. Depression, Anxiety, Stress scale (DASS-21) 12 was used to predict the power of the scale.
Translation and adaptation of the DES was carried out by using the previously published guidelines. 13 To test item clarity, linguistic equivalency, and content validity, the translated version was submitted to a committee of twelve dentists. This committee presented the first version, which was validated by 50 students who represented five years of education. Students were provided an evaluation form to express any doubts or suggestions along with the first version of the Turkish DES. There have been no significant modifications regarding difficulties in understanding, and the last version was approved.
Evaluation of Data
The data obtained were analyzed using the program SPSS 20.0 (Chicago, IL, USA). The demographic characteristics of students were analyzed by using descriptive statistical analyses. Two-tailed tests with a significance level of 0.05 were conducted.
Kaiser-Meyer-Olkin (KMO) and Bartlett’s Test of Sphericity were used to evaluate suitability for factor analysis. Principal component analysis was carried out for the 32 factors composing the DES to highlight the substantial components (eigenvalues ≥ 1.0) and to reduce dimensionality of the scale. Factor loadings were used to present a correlation matrix to observe the correlation between items and factors. Also, a scree plot is originated from the obtained eigenvalues (Figure 1).
Factor loadings obtained from principal components analysis and Varimax rotation were evaluated and factor loading values lesser than 0.30 were excluded.
Internal consistency was examined using Cronbach’s α coefficient (95% CI) to evaluate the reliability of the scale. Internal consistency was also examined for each subscale to prove the unidimensionality of the subscales of the Turkish version of DES.
Results
The mean age of the students included in the study was 21.7 (±2.1). Most of the participants were females (59.1%), 27.9% were in the second year of their studies, and 99.3% were single.
Translation and Cross-Cultural Adaptation
Concerning the conceptual equivalence of items, as a result of literature review and discussions with expert professionals, some items of the DES scale were considered to be unrelated to the Turkish population and were therefore removed or changed.
Thus, the term “administrative responses to student needs” was replaced by “rules/regulations of the dental faculty and administrative responses to student needs,” “marriage relationship” by “difficulty in engagement/marital relationship,” “roommate relationships” by “lack of home atmosphere in living hostel,” and “patient care responsibilities” was replaced by “responsibility for comprehensive patient care.” Additionally, the items “child care, alcohol usage, drug usage, reconsideration of dentistry as proper career choice, and fear of flunking out of school” were removed. By removing item “reliability of professional dental laboratories in prompt return of cases,” item “difficulty in learning precision manual skills required in preclinical and laboratory practice” is preserved. Items’ “personal physical health” and “physical health of other family members” are combined as item “physical health of family members/personnel.” Items “difficulty of manual dexterity”, “lack of confidence to be a successful dental student,” “lack of confidence to be a successful dentist,” “risk of infectious diseases (HBV, HCV, HIV, etc.),” “fear of failing the year,” “fear of not having possibility to pursue a postgraduate program,” “fear of unemployment after graduation”, “lack of time for relaxation and recreation,” “completion of clinical and graduation requirements,” “amount of cheating in dental faculty,”, “lack of confidence in clinical decision making,” “shortage of allocated clinical time,” and “working on patients with poor oral hygiene” have been added. Two items with an estimate value less than 0.4 were excluded. Explanatory factor analysis results showed 30 items for the Turkish version of the DES scale.
Face validity of the Turkish version of the DES assessed for 50 students represented 95% understanding of the items. These 50 students did not participate in the final assessments.
Content Validity Index
According to the experts’ findings, the Content Validity Index (CVI) values of the items ranged between 0.83 and 1.00, and the CVI value for all scale items was found to have a high validity score of 0.97.
Construct Validity
The KMO value of the draft scale with 32 items was 0.885 in terms of sampling adequacy, while the Barlett Test result was X² = 4276,085, df = 496, P <.001, and it was established that the dataset was appropriate for a factor analysis. Explanatory factor analyses were used to evaluate the construct validity of the scale.
Exploring the data structure revealed eight components (eigenvalues ≥ 1.0) explaining 62.954% of the total variance. Among these, five factors (eigenvalues ≥ 1.390) explained 52.299% of the total variance. The scree plot of eigenvalues suggested the domination of a single variance after the fifth component. Therefore, according to the eigenvalue scree plot, it was seen that 30 items of Turkish DES were organized into five components (Figure 1).
Construct 1: Ten0 items about “Academic Performance” explaining 29.377% of the common variance
Construct 2: Three items about “Professional Future” explaining 36.699% of the common variance
Construct 3: Five items about “Responsibilities with Patients” explaining 42.642% of the common variance
Construct 4: Six items on “Social Factors” explaining 52.299% of the common variance
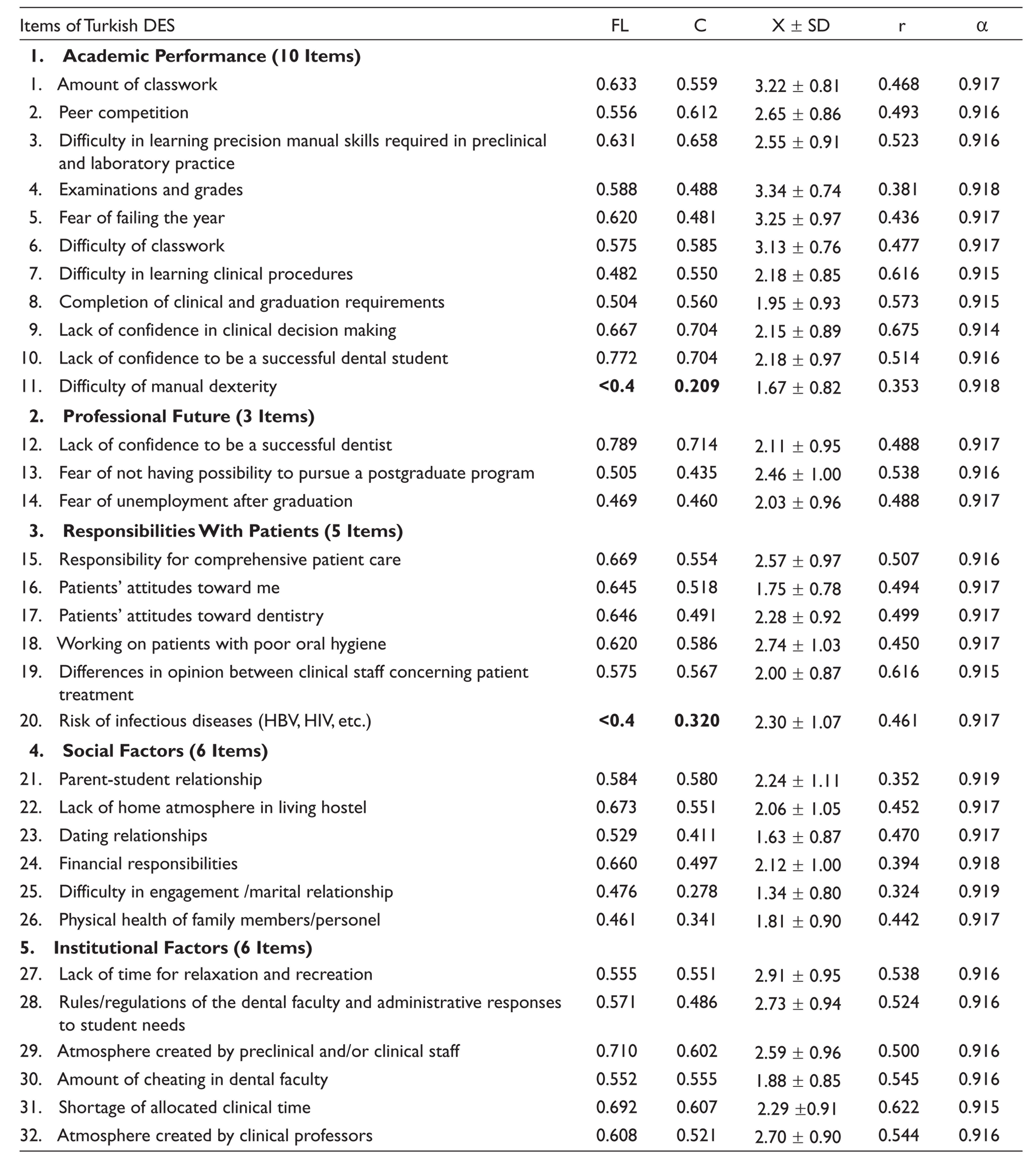
Construct 5: Six items on “Individual and Institutional Factors” explaining 47.955% of the common variance (Table 1).
Construct 3 “Responsibilities with Patients” has not been answered by preclinical students. The responses of preclinical students were evaluated over other factors.
Factor Loadings (FL), Communalities (C), Means (X ! SD), Corrected Item-Total Correlation (r), Alpha (α) Values of the Items
Concurrent Validity
DASS-21 was used to determine the concurrent validity of Turkish DES. Turkish DES and DASS-21 were correlated (r = 0.221 to 0.480 and P = .000; Table 2).
Correlations Between DASS-21 and Turkish DES

Reliability
The Cronbach’s α reliability coefficient of the final shape of the scale with 30 items was 0.919. This result shows that the scale has high reliability and contains a sufficient number of items. There is no item whose removal would make the total Cronbach’s α value greater than 0.919. Each item showed an adequate internal consistency with Cronbach’s α between 0.914 and 0.918. With this result, it can be said that every item in the scale is important, that reliability can be compromised if any of them are deleted, and that the scale has high reliability in its current shape.
With the item-total score correlation, the relationship between each scale item and the total score was examined, and the values of the scale ranged between 0.324 and 0.675. The minimum value required for the item-total test correlation is stated to be 0.30. 15 Thereby, the item-total score correlation coefficients for the scale is sufficient.
Table 1 illustrates the mean score of the items, item-total score correlations, and the significance levels. The correlation level of all items and factors to item-total score is very significant (P = .0001).
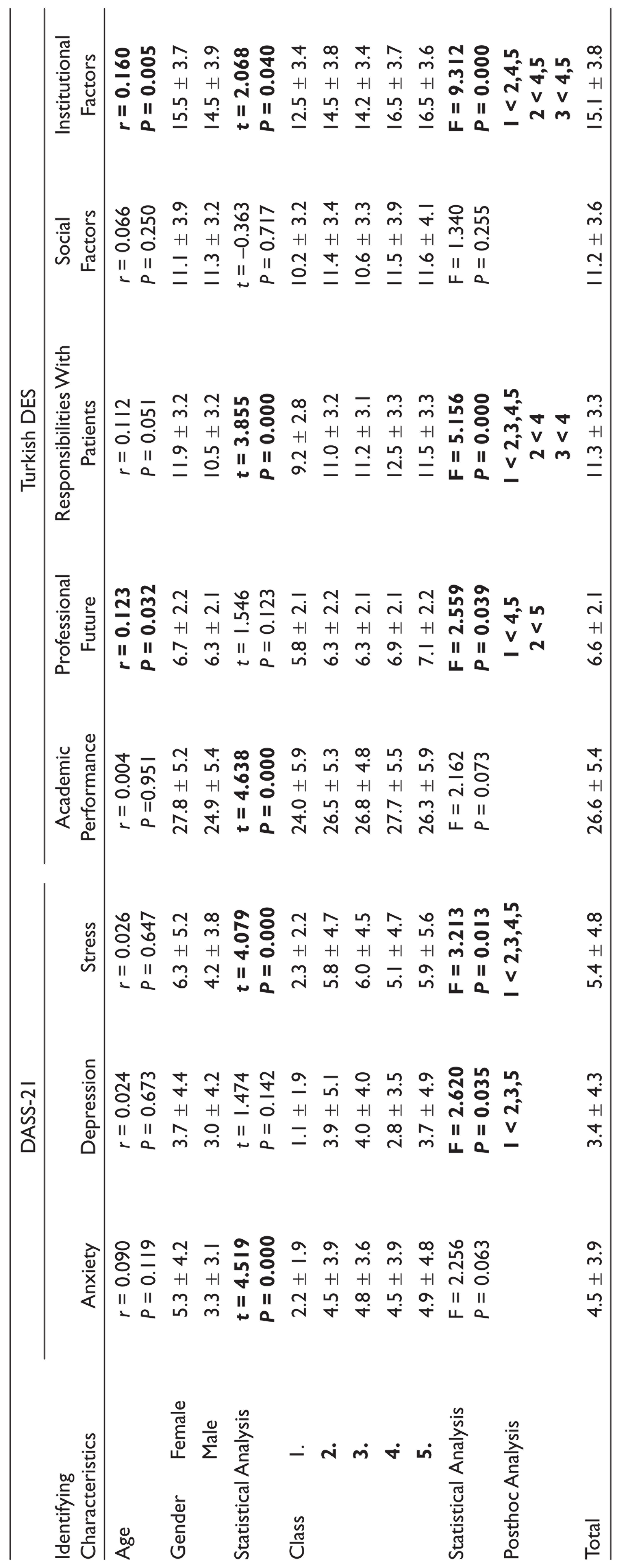
Comparison of Students’ Characteristics and Scores of DASS-21 and Turkish DES
Anxiety (5.3 ± 4.2), stress (6.3 ± 5.2), academic performance (27.8 ± 5.2), responsibilities with patients (11.9 ± 3.2), and institutional factors (15.5 ± 3.7) mean scores of female students are significantly higher than males (P < .05).
Depression levels of first class students are significantly lower than second, third, and fifth grade students (F = 2.620, P = .035).
Similarly, the stress levels of first graders are significantly lower than other grades (F = 3.213, P = .013).
When ‘Professional Future’ levels are examined, it is significantly lower for first graders than fourth and fifth grades and second grades than fifth grades (F = 2.559, P = .039). When the ‘Responsibilities with Patients’ levels are examined, the first grades are significantly lower than all other grades, second and third grades than fourth grades (F = 5.156, P < .001). When ‘Institutional Factors’ levels are examined, it is significantly lower than the first class's second, fourth, and fifth grades, and the second and third grades than the fourth and fifth grades (F = 9.312, P < .001; Table 3).
Comparison of DASS-21 and Turkish DES With Identifying Characteristics
Discussion
Stress management is a crucial need in dental education to minimize unwanted effects of stress on dental students and dentists. Identifying stress factors could help to develop stress management interventions. This study aims to provide an effective instrument for identifying environmental stress factors in dental education. 6 We performed cross-cultural adaptation of the DES to identify environmental stress factors of dental education in Turkey.
To the best of our knowledge, this is the first study to develop a perceived stress scale suffered by Turkish dental students. The previously available tool for assessing perceived stress among Turkish dental students was the DES questionnaire. However, questionnaires are nonstandard data collection tools. Fort this reason, it is necessary to use scales with a high degree of validity and reliability that are based on sound theoretical foundations. DES is adapted to different languages and cultures previously.16–20 Similar to this our study revealed satisfactory results suggesting appropriate cultural adaptation of the Turkish version of the DES scale.
Factor analysis identifies organization of the construct of the sample instead of hypothetical divisions, by reducing large number of variables into fewer number of factor.
Factor analysis is a technique that is used to reduce a large number of variables into fewer numbers of factors. 16 DES was subdivided into seven subscales, 21 while this study identified five subscales for Turkish version of DES. Reliability results differed in Turkish cultural adaptation.
The validation process of Turkish DES showed that Turkish version of the scale is reliable. The psychometric properties of the Turkish DES were satisfactory showing that the scale is reliable and valid. Also, Turkish DES showed significant consistency to previous reports.17,18,20
In scale development/adaptation studies, the number of samples must be adequate to perform a factor analysis. Tinsley and Kass (1979) argue that if the number of samples is below 300, the number of items should be five to ten times the number of samples, and if the number of samples exceeds 300, stable results can be achieved independently of the number of items. 22 This study was performed with 308 students, about 10,25 times the 30-item scale, and, in accordance with the literature, it was decided that the sample of 308 students for which the 30-item draft scale is intended to be applied was adequate.
The standardization of a scale and its ability to produce appropriate data depend on the reliability of the measurement values and the degree to which it can accurately measure the characteristics it is intended to measure validity. In terms of validity, it is important that the scale is objective, distinctive, comprehensive, easy to apply, and scorable. CVI value 0.97 shows a high content validity and this result can be interpreted as indicating that each item of the developed scale measures the concept intended to be measured. 23
Various DES adaptations of different countries reported that female students experienced higher stress in the Anxiety, Stress, Academic performance, Responsibilities with patients and Institutional Factors subscales regarding the relationship of gender and perceived sources of stress in accordance with Turkish DES.1,6,9 These higher rates might be based on different reaction patterns of females to stressful events. 24
In parallel with other studies, the results show that there is an increase in general student stress factors as the student progresses in the program.21,25 Stress factors in the advancing grades mainly consisted of “professional future,” “responsibilities with patients,” and “individual and institutional factors.” As confirmed by various studies, upper grade students face future concerns and have uncertainties about their dental education. 16 The increase in stress factors related to academic and clinical evaluation for years after the first year may be because of the clinical education evaluation process. The dental education should help students to be more confident about the professional life.
This study has a limitation about participants which were limited to one dental faculty making it difficult to generalize the results. Also, psychological aspects of the perceived stress was not investigated. In addition to this, longitudinal studies are needed to follow students throughout their curriculum.
Conclusion
In conclusion, this study is the first to develop and validate a scale for measuring the perceived dental environmental stress among Turkish dental students. This scale fills in the gap in the objective assessment of stress factors in dental education. Achievements of construct validity shows the advantages of using the Turkish version of the DES to realize stress factors in dental education.
On the basis of these results, this scale with verified reliability and validity is recommended for investigators who wish to measure perceived dental environmental stress suffered by dental students.
Footnotes
Future Scope
Further research may allow the instrument to be improved and understood. Also the scale could be generalized by applying to larger samples.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Aspects
Ethical Consent Forms (Number: 358) were received from the University Clinical Trials Ethics Committee and permission was obtained from the students enrolled in the survey study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Declaration of Consent (If In-vivo Study/Case Reports)
The students were asked to participate voluntarily. Informed written consent was obtained from participants and they were fully informed. Participants were given freedom to withdraw from the study at any time.