
Abstract
Objective:
The purpose of this study was to evaluate dentinal microcrack formation during root canal treatment using Mtwo NiTi rotary instruments and MicroSeal filling technique.
Materials and Methods:
Forty-five single-rooted teeth were selected for the present study and divided into 3 different groups (n = 15): Group 1, in which root canals were instrumented with Mtwo rotary files; Group 2, in which root canals were instrumented with Mtwo rotary files and filled using the MicroSeal technique; and Group 3, that acts as a control group in which no instrumentation nor obturation were performed. Then, roots were sectioned 3 mm, 6 mm, and 9 mm from the apex and the cut surface has been observed under a stereomicroscope to check for the presence or absence of dentinal microcracks. Number of dentinal microcracks was registered for each group at different levels and data were statistically analyzed using the Chi-square test with a level of significance set at P < .05.
Results:
No statistically significant differences were registered among groups (P < .05). No microcracks were detected in Groups 1 and 3, while two dentinal microcracks were registered in Group 2.
Conclusions:
Mtwo rotary instruments and the MicroSeal root canal filling technique did not significantly induce dentinal microcrack formation.
Introduction
Biomechanical preparation of root canals is one of the main steps in achieving endodontic success. 1 It enables bacterial elimination, promotes removal of debris and facilitates filling of root canals in three dimensions, which is crucial in order to prevent bacterial growth. 2 Both instrumentation and filling procedures may be linked to the presence of dentinal microcracks, a clinical problem that reduces tooth resistance and facilitates vertical root fracture (VRF).3,4
VRF is one of the most frustrating complications of root canal treatment, which often results in tooth extraction. 5 Root fracture might occur as a result of a microcrack that propagates with repeated stress application by occlusal forces 6 and is usually the consequence of the propagation of a pre-existing defect. 7 For this reason, in the last years several studies have been conducted on the potential causes of cracks origin and propagation.
A lot of predisposing factors may be involved in the origin of VRF, including root canal anatomy, 8 loss and change of dentin after an endodontic treatment, 9 filling techniques,4,10 small cracks, and aging. 11 Aging may also change the evolution of the crack, in fact in young people cracks spread throughout the intertubular dentin, while in old people throughout the peritubular dentin. 12
Mechanical instrumentation of root canals using NiTi rotary or reciprocating systems has been reported to be one of the causes that can create microcracks in root dentin, 4 because of the rotational force applied by these instruments to the root canal walls. Hand instrumentation, in fact, showed a less incidence of microcracks formation and propagation than mechanical instruments. 3 The extent of such a defect formation may be related to several factors, such as the tip design, the cross-sectional geometry, a constant or progressive taper, a constant or variable pitch, and the type of flutes. 13 More recent studies have, instead, demonstrated a lack of causal relationship between root canal instrumentation and the type of root canal instrumentation and the presence of dentinal microcracks.14,15
The association between obturation and cracks has been widely studied,4,10,16,17 because the use of forces during the condensation techniques may alter the dentine structure ultimately leading to a root defect or fracture. Several authors studied the incidence of dentinal microcracks after filling of root canal using the cold lateral compaction technique, reporting that it resulted in more incomplete fractures compared to the unprepared root canals4,10,18 and more dentinal defect than the instrumentation procedure only, mostly in the middle and coronal third of the root. 17 Furthermore, there are statistically significant positive linear correlations between fracture load and root width, canal width, canal taper, ratio of canal width to total root width, and number of accessory cones placed. 19
Other authors reported a possible relationship when a vertical compaction technique was used, 4 maybe for the “wedging effect” generated in the canals by a big plugger that can touch the dentinal canal walls, defined by Blum et al 20 as the rod of a hydraulic jack and the vertical force applied by this rod induces in the cylinder (the canal) a hydrostatic pressure that is relatively equal in all directions.
There are several methodologies in literature which have been used to study microcrack formation. The use of a stereomicroscope with low magnification (5×) may not be enough to observe microcracks, 21 as these dentinal defects are difficult to be detected with this methodology because in most of the cases the dentinal surface is not regular and color variations often occur due to dentin deposition or presence of isthmuses, 14 which may be considered as dentinal defects. 22
The use of endoscopy with different magnification present a higher sensitivity for complete canal cracks than for incomplete dentinal microcrack. 23 Vibrating the dentinal crack surfaces using an ultrasonic scaler to generate frictional heat is another methodology of investigation, with the registration of the heat with an Infrared thermography (VibroIR). A further method is the scanning electron microscopy (SEM), but it is a destructive methodology that requires an elaborated specimen preparation which may change the actual status of the tissue.11,22 Finally, the transillumination is the detection method that show whether a crack is present and is the most common modality for crack diagnosis in clinics but can promote high-level dramatization of all defect. 24 For this reason, the same author suggested the additional use of staining agents like methylene blue.
Another destructive methodology is the sectioning technique, one of the most used in the endodontic researches. It employs direct observation of teeth by microscopy or stereomicroscopes after sectioning the root with a saw at different levels, photographed using magnification from 8× to 1005×.4,10,25 The sample is cut at specific levels of the root, embedded, or not, in acrylic resin or glued to a standard base. However, the evaluation of few slices per sample allows the possibility of missing microcracks before or next to the specific cut and is unable to assess the presence of longitudinal defects. 26 As other destructive methods, the pre-operative condition of the dental structure is unknown. 15
A nondestructive and reproducible methodology is the micro-computed tomography (MCT) that can be applied for 2D and 3D assessment of root anatomy and microcracks observation. 14 This is a nondestructive method with or without the use of contrast agents, highly accurate, with a possible evaluation of pre- and post-treatment changes in root structures; however, scanning and reconstruction procedures take considerable time and is expensive.
The aim of the present study was to evaluate dentinal microcracks formation during root canal treatment performed using Mtwo rotary instruments and MicroSeal filling technique. The null hypothesis tested was that there is no significant difference in dentinal microcracks formation with respect to an untreated control group.
Materials and Methods
A total of 45 single-rooted intact extracted teeth completely formed premolar teeth of similar dimensions were selected for this study and stored in 0.1% thymol in distilled water. All roots were inspected under a stereomicroscope at 10× magnification to detect the presence of any preexisting crack or fracture, and specimens with such findings were excluded from the study and replaced. The coronal portion of each specimen was flattened using a diamond-coated bur under water cooling to obtain similar lengths, the access cavity was opened, canal patency was established with a #10 K-file (Micro-Mega, Besancon, France) in each root, and the working length established was 0.5 mm short of the point when the file appeared at the apical foramen.
The specimens were then divided into 3 different groups (n = 15). In Group 1, root canals were instrumented with Mtwo rotary files up to a final size of preparation of tip size 25/0.06 taper. Ni–Ti Mtwo instruments were used in a 16:1 handpiece (Anthogyr, Sallanches, France) in conjunction with a high torque endodontic electric motor (E-Go, Sweden & Martina, Padova, Italy) at 250 rpm in a simultaneous technique. 27 Instruments were each taken to working length with light apical pressure. As soon as the clinician felt a binding sensation, the instrument was withdrawn 1 mm to 2 mm so that it could be worked in a brushing action to selectively remove the interferences and to advance toward the apex. The instruments were used with lateral pressure in order to obtain a circumferential cut, and they were only allowed to rotate at length for three strokes. During shaping, each canal was irrigated between each successive instrument with 2.5 mL of 5.25% NaOCl using an endodontic syringe (Naxitip, Ultradent, South Jordan, UT, USA) placed as far into the root canal as possible without binding. The final flush was performed with 5 mL of 17% EDTA solution, rinsed out with 5 mL of saline solution.
In Group 2, root canals were instrumented with Mtwo rotary files as in Group 1 and filled using the MicroSeal technique (SybronEndo, Orange, CA, USA). After root canal preparation and irrigation, canals were completely dried and a standardized master point tip size 25/0.02 taper was fitted at the working length using a small amount of endodontic sealer (Pulp Canal sealer, SybronEndo) on its tip. A rotary spreader was used at 250 rpm to laterally condense the master cone up to 2 mm from apex. The canals were then completely filled with softened pre-heated gutta-percha delivered into the canal using a PacMac rotary gutta condenser (SybronEndo) at 7000 rpm up to 3 mm from the working length. The rotary spreader was then used to compact the warm gutta-percha up to 3 mm to 4 mm from the working length and the new created space was refilled again with pre-heated warm soft gutta-percha as described earlier in this article. 28
In Group 3, that acts as a control group, the roots were left intact and no instrumentation nor obturation were performed.
All the roots were stored for 2 weeks at 37°C and 100% humidity (in purified filtered water) to ensure complete setting of the sealer and to prevent dehydration
Sectioning and Microscopic Examination
All the roots were then included in acrylic resin in order to enable better sample handling and easier sectioning of the tooth, and then the blocks were sectioned with a saw machine (Micromet, Remet, Italy) perpendicular to the long axis 3 mm, 6 mm, and 9 mm from the apex using a diamond-coated bur (WS Flex 18C Waterproof, Hermes Schleifmittel GmbH, Germany) of 0.6 mm thickness under water cooling. 5 The sectioned surfaces were then impregnated with methylene blue dye and observed with a stereomicroscope from 10× to 40× magnification by two separate observers to check for the presence or absence of dentinal microcracks that were in contact with the canal lumen. Cracks not originating from the canal lumen were excluded from the study, since the instrument used for the endodontic treatment cannot cause any defects in the outer part of the root. Pictures were taken at different magnifications and disagreements were solved by discussion. Number of dentinal microcracks was registered for each group at different levels and data were statistically analyzed using the Chi-square test with a level of significance set at P < .05.
Results
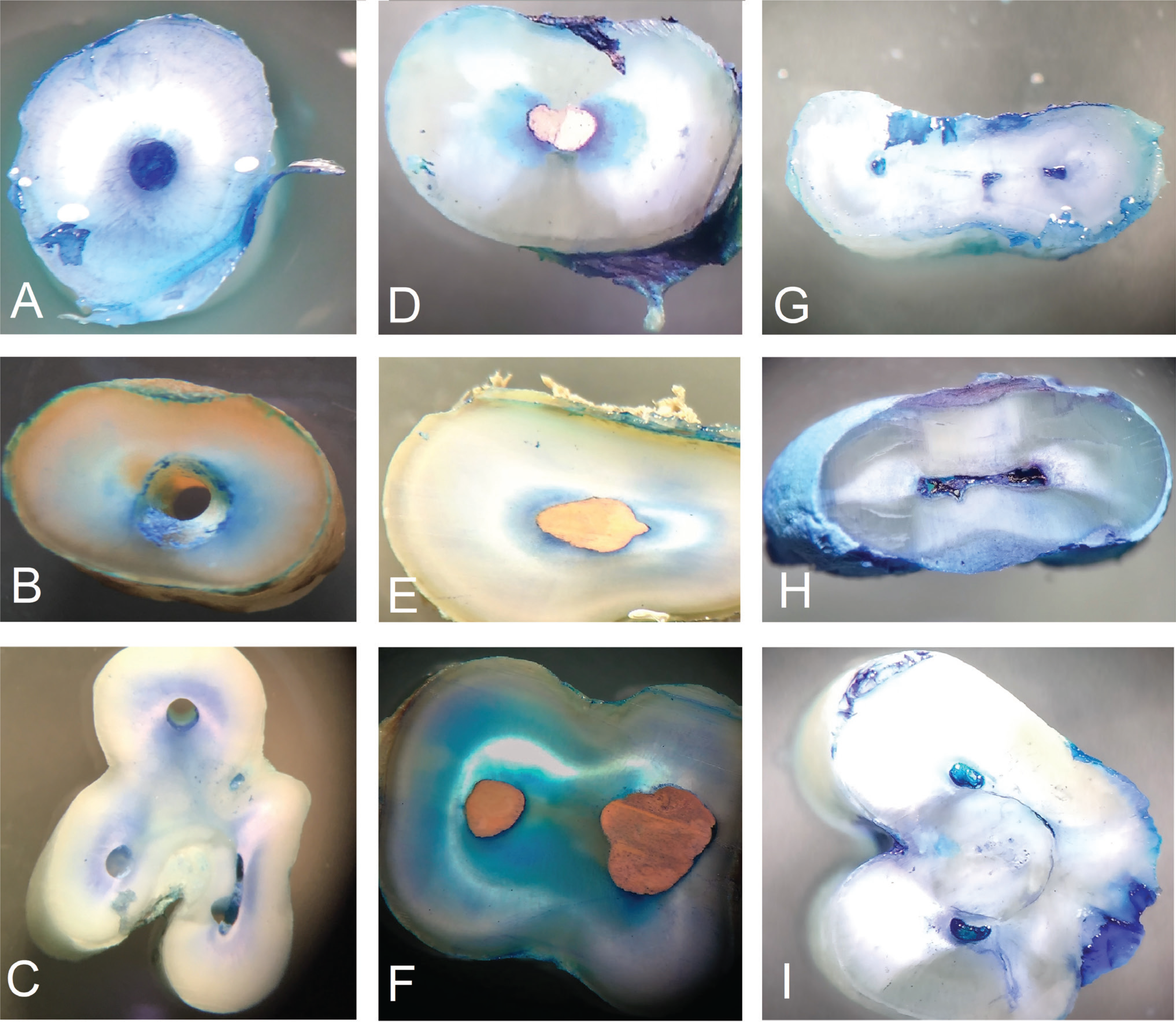
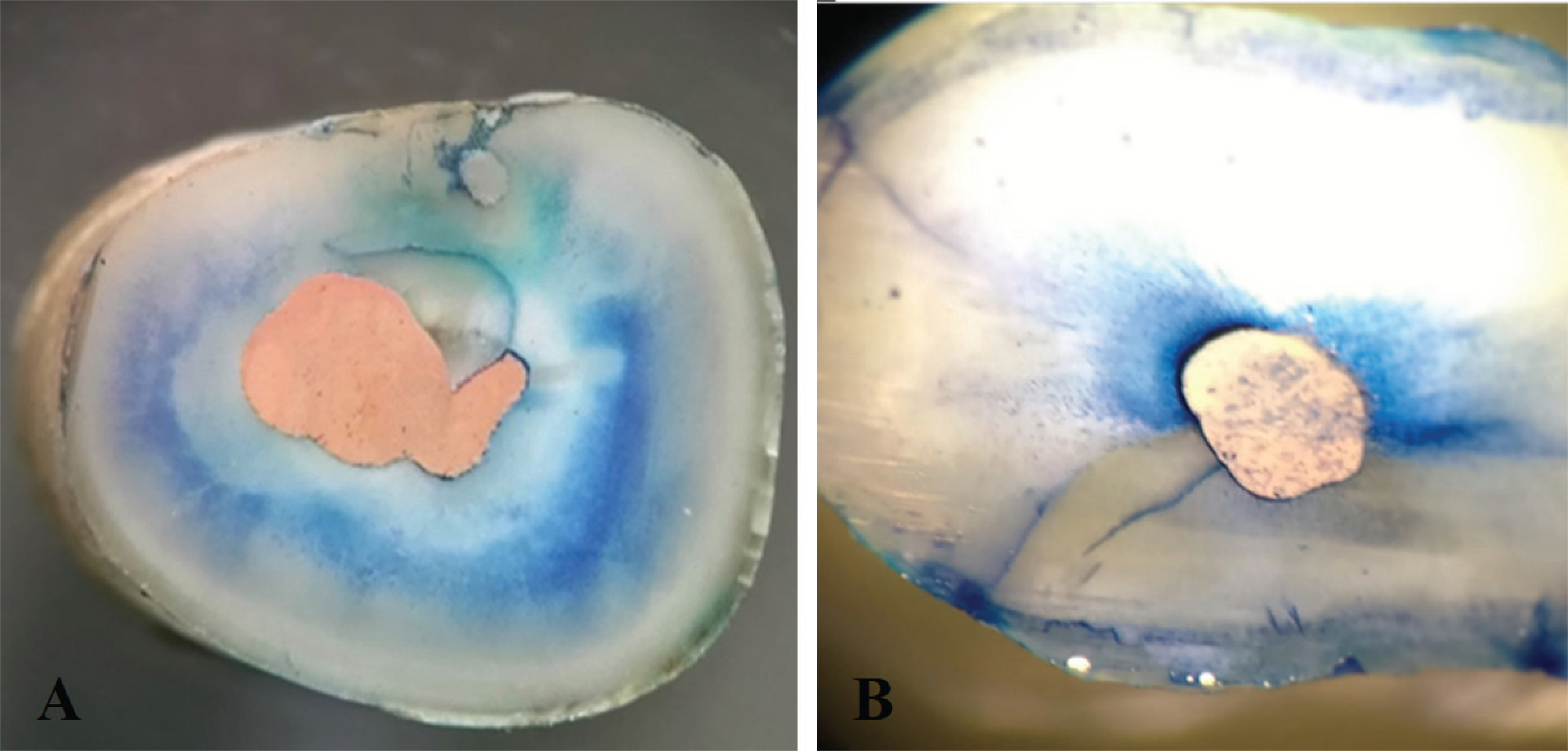
The results of the present study revealed no statistically significant differences among the three groups (P > .05). No complete fractures of the roots were observed in all groups. Sections obtained from the teeth of Group 1 (instrumentation only) and Group 3 (untreated specimens) did not present any microcrack in conjunction with the root canal lumen (Figure 1). However, microcracks were found in 2 cross sections from the specimens of Group 2 (instrumentation and obturation), one at 6 mm middle level and the other at 9 mm coronal level (Figure 2).
Discussion
Some endodontic instrumentation methods might induce dentinal defects. In vitro studies reported that the frequency of microcracks was lower in teeth instrumented using hand file than in those using mechanical instrumentation.3,22 In the last decades, many new NiTi rotary and reciprocating systems have been developed and introduced in the market. There is a potential relationship between the design of NiTi instruments and incidence of microcrack formation, as it has been demonstrated that file design may affect apical stress and strain concentration during root canal instrumentation. 13
In the present study, no significant differences among the 3 groups were found, thus the null hypothesis may not be rejected. The incidence of dentinal microcracks found in the present study was lower than that previously reported in existing literature, with a percentage ranging from 10% to 60%.3,8,9,29 However, such a percentage of dentinal microcracks should suggest similar findings for VRF, which represent their evolution. On the contrary, in the literature VRFs are observed in only 2-5% to 10.9%30 and 20% in extracted endodontically treated teeth. 31
Images showing samples without microcracks from the 3 groups analyzed at the 3 different sectioning levels. From left to right the columns of instrumented teeth (Group 1, Figures A, B, C), instrumented and obturated teeth (Group 2, Figures D, E, F) and the untreated specimens (Group 3, Figures G, H, I); from up to down the rows of 3 mm, 6 mm, and 9 mm apical, middle, and coronal levels.
Among these studies, Jindal et al 12 have also evaluated Mtwo instruments, reaching a percentage of microcrack of 60% that disagrees with the findings of the present study. In fact, in the present study the higher percentage of microcracks was registered in Group 2 (4.44%), which corresponded to only 2 defects, one in the middle third and one in the coronal third. This finding may be attributed to the sum of the filling procedure to the instrumentation step, as it is the only difference with Group 1, in which no defects were registered. Yoldas et al 25 reported various degree of fracture rates, from the absence of fracture in roots instrumented with hand files and control group (unprepared) to 31 microcracks in canals mechanically prepared using NiTi rotary files, being this the last finding in disagreement with the present study where no defects were observed in root canals prepared using Mtwo instruments.
Rahman et al 21 investigated root defects as complete, partial, or other (external fractures) in unprepared and prepared canals; considering mechanically instrumented roots, the number of microcrack was 2, which is the same number of dentinal defects observed in instrumented and filled canals in the present study. Other previous studies conducted by means of Micro-CT nondestructive analysis of the samples confirmed the results of the present study, with pre-operative values of presence of cracks similar to the postoperative ones.14,15
Images showing the two dentinal microcracks found in Group 2. (A) Coronal 9 mm section and (B) middle 6 mm section.
Several authors studied the influence of dentinal microcrack after root canal cold lateral compaction technique,4,10,16–18 while no studies have investigated a possible association between microcracks and the MicroSeal filling technique that uses a rotary spreader to compact guttapercha. 28 Onnink et al 18 reported that root canal preparation and lateral compaction resulted in more incomplete fractures compared to the unprepared root canals and that the incidence of fracture in the obturation groups was not significantly different from that in the group in which root canals underwent root canal preparation only, that is in agreement with the results of the present study.
Shemesh et al 4 stated that the unprepared canals had no dentinal defects, while roots with prepared canals had significantly more defects, that is in disagreement with the results of the present study. Considering the filling technique, the number of microcrack in canals filled with the lateral compaction technique was significantly more frequent than in the unprepared group, as further reported by the same authors, 10 but not respect to the instrumented group, that agrees with findings of the present study. In another study, Barreto et al 16 reported that the lateral compaction group did not show statistically significant more microcracks than the instrumented group, in agreement with the results of the present study. Furthermore, Capar et al 17 reported that root canals filled with cold lateral compaction technique presented dentinal defects mostly in the middle and coronal third of the root, as found in the present study.
In all the previously reported studies, stainless-steel hand/finger spreaders were used for the cold lateral compaction technique; the MicroSeal filling technique investigated in the present study utilizes a rotary NiTi spreader to perform the compaction phase. There are several reasons why a NiTi rotary spreader is preferable to a stainless-steel hand/finger spreader: The potential for VRF in curved canals during lateral condensation may be minimized by using NiTi spreaders, 32 NiTi spreaders penetrate deeper into the canal and produce less force on the dentinal root wall, 33 but there was no evidence of a significant difference in microleakage of root canal fillings performed using these two different spreaders. 34
A great difference has been registered among the studies published on this topic. 35 It may be related to the different methodologies used and the difficulty to standardize such studies, which increase the possibility to register false positive results. Furthermore, it is not always clear. 35 The storage method of the samples is also crucial because a dehydrated tooth will have a reduced resistance to the forces applied on each direction during the instrumentation and filling procedures or the analysis through cutting or scanning the samples. 36 It has been also reported that in a well-hydrated root, there was not an increase of residual microstrain or the formation of microdefects in root dentin. 37 Another factor that may have an influence on the outcome of these studies is the age of the teeth used. Indeed, the results of previous studies have reported a reduction of crack growth and an increase in fracture resistance of about 30% for older teeth 12 due to the reduction of the lumen area and deposition of mineralized structure. 11 Another study confirmed that the average fatigue resistance was significantly lower in young hydrated dentin than in old dentin. 38
One of the limitations of the sectioning method used in the present study may be the impossibility of visualize pre-operative dentin status because chemical attack by storage solution, the extraction forces, trauma of dysfunctional occlusal forces prior extraction, and sectioning procedures can introduce analysis errors in sample groups.16,35 In particular, the microcracks found can be eventually realized by the sectioning procedures, instead of the mechanical and filling procedures. MCT undestructive 3D studies may overcome this bias. 14
Conclusions
Results of the present study reported that there is no statistically significant relationship between microcracks presence and Mtwo instrumentation sequence and MicroSeal filling technique.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to thank Department of Oral Science, Nano and Biotechnology, University of “G. d’Annunzio” Chieti–Pescara, for funding this research (5537/27-11-2017) for the scholarship provided to the first author (Carlesi T.).