
Abstract
Purpose
We have previously described anterior cruciate ligament reconstruction with a rounded rectangular femoral tunnel created using a rounded rectangular dilator designed to enable a more anatomical and wider tendon-bone junction. However, the influence of remnant tissue preservation on the creation of the rounded rectangular femoral tunnel is not clear. This study aimed to evaluate the influence of remnant tissue preservation on the creation of the rounded rectangular femoral tunnel.
Methods
A total of 198 patients who underwent primary anterior cruciate ligament reconstruction with a rounded rectangular femoral tunnel were evaluated retrospectively. Patients were categorized into a remnant preservation group (group P) and a non-preservation group (group N). Computed tomography images taken 1 week postoperatively were analyzed. The location of the rounded rectangular femoral tunnel evaluated using the quadrant method, its rotation angle, and the graft bending angle were compared between the two groups. The differences and the variance in femoral tunnel assessment were compared using the two-sample t-test and Levene’s test.
Results
Although there was no significant difference in the location of femoral tunnel for the deep/shallow direction along the Blumensaat’s line (difference, p = .326; variances, p = .970), the tunnel was significantly lower in group P than in group N, with no variances (difference, p = .001; variances, p = .326). There were no significant differences and no variances in the tunnel rotation angle and the graft bending angle (difference, p = .727 and 0.514, respectively; variances, p = .827 and .445, respectively). Blow out of the posterior wall of the medial aspect of the femoral lateral condyle was an intraoperative complication that occurred in one case in group N.
Conclusion
The remnant preservation approach creates a lower femoral tunnel compared to the non-preservation technique. However, a rounded rectangular femoral tunnel can be created safely and is reproducible with remnant tissue preservation.
Keywords
Background
Anterior cruciate ligament reconstruction (ACLR) is required to restore joint stability during anterior and internal rotation after an ACL injury. However, a multicenter study on ACL revision reported that technical errors, such as malpositioning of the femoral tunnel, were the main causes of ACLR failure. 1 Trojani et al. 2 reported that technical errors occurred in half of the knees with failed ACLR, and in these cases, malpositioning of the femoral tunnel occurred three times more frequently than that of the tibial tunnel. Therefore, a reproducible and precise method that can be used to create a femoral tunnel within the anatomical footprint of the ACL is important.
ACLR with remnant tissue preservation has been reported to have several advantages.3–7 Crain et al. 3 classified remnant ACL tissues into four types and reported that roof- or wall-adhering remnants (type II or III) contributed to anteroposterior stability. Nakase et al. 6 reported that remnant tissues that were attached to the lateral walls affected not only the anteroposterior laxity but also the rotational stability of the knee. A study on second-look arthroscopy after ACLR with remnant tissue preservation using a hamstring autograft reported that patients with preserved remnant tissue had a thicker graft with better synovial coverage and were resistant to tibial tunnel enlargement.4–7 Recently, Lee et al. 5 found that remnant tissue preservation during ACLR led to better proprioceptive and functional outcomes.
When ACLR is performed, the femoral tunnel is usually made into a round shape using conventional round drills. In contrast, we performed ACLR with a rounded rectangular femoral tunnel using a rounded rectangular dilator that was designed to enable a more anatomical and wider tendon-bone junction.8–10 Some studies have reported that the oval femoral tunnel technique is better at accelerating tendon-bone healing in the early period after ACLR and yields a better knee functionality and laxity than the conventional round femoral tunnel technique.11,12 A few studies have reported that remnant-preserved double-bundle ACLR could be performed with high reproducibility.13,14
The purpose of this study was to evaluate the influence of remnant tissue preservation on the creation of a rounded rectangular femoral tunnel. We hypothesized that a rounded rectangular femoral tunnel could be created precisely and is reproducible even if the proximal end of the remnant tissue was preserved.
Material and methods
We retrospectively evaluated 257 patients who underwent primary ACLR at our hospital between October 2013 and December 2019. All surgeries were performed using the hamstring tendon. The position of the tunnel was assessed using computed tomography (CT) images taken 1 week after ACLR. The mean follow-up duration was 23.8 ± 8.6 months (12–66 months). The exclusion criteria were ACLR with bone-patellar tendon-bone grafts, multi-ligament injuries that required other ligament surgeries, and a history of surgery or revision surgery. Those cases in which CT images could not be taken 1 week postoperatively were also excluded. Patients who were followed-up for less than 1 year were also excluded. After excluding 59 patients, data from 198 cases were finally analyzed. The cases were categorized into a remnant preservation group (group P) and a non-preservation group (group N). Group P included knees with Crain type II or III remnant tissue 3 that adhered to the roof or the wall of the medial aspect of the lateral femoral condyle, and group N included cases with Crain type I or IV remnant tissues whose proximal ends were not attached anywhere, although their distal ends were attached to the tibia. Cases wherein the proximal ends of the remnant tissues were excised because of very poor continuity were also included in group N. Furthermore, those cases with Crain type II or III remnant ACL tissues after surgery, in which 50% or more of the remnant tissue attached to the femoral condyle was resected intraoperatively, were changed to group N. Operation records were used to retrospectively confirm the procedure for remnant tissue. This study was approved by the Kanazawa University Medical Ethics Review Committee (1842-1), and verbal informed consent was obtained from each patient before they participated in the study.
Patient demographics
A total of 85 knees and 113 knees were assigned to group P and group N, respectively. Femoral tunnel size was defined as the size of the femoral rounded rectangular dilator used during the surgery. A total of 14 cases with Crain type II or III remnant tissues were converted into group N as 50% or more of the remnant tissue was resected during the surgical procedure because of the level of damage.
Surgical technique
Surgery was performed, and the classification of the remnant tissue was determined by a senior orthopedic surgeon (J.N.). Anatomical single-bundle ACLR was performed using a rounded rectangular femoral dilator, as previously reported.
8
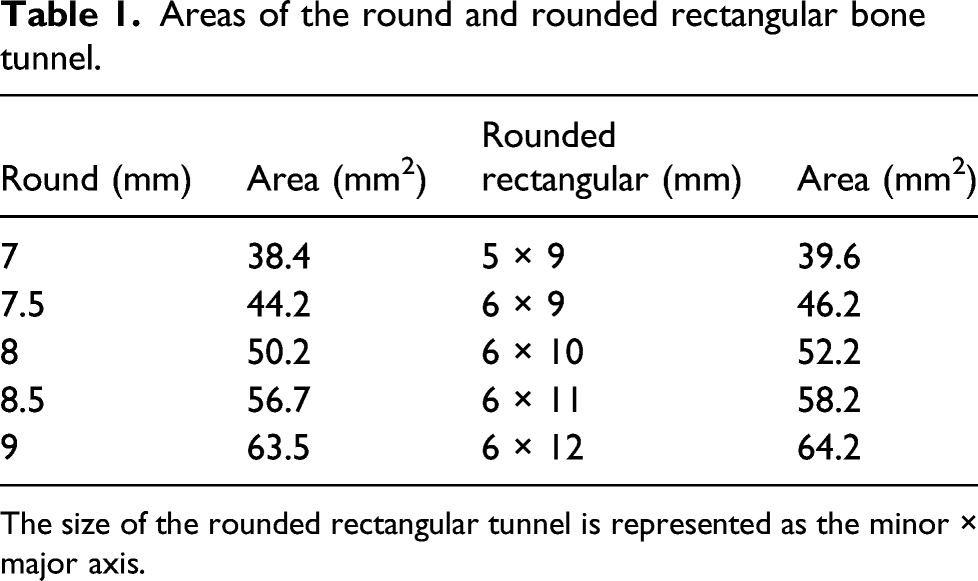
The minor axis of the dilators was 6 mm long, while its long axis varied in length to match the size of the graft (Figures 1(a) and (b)). The areas of the round and rounded rectangular bone tunnels are shown in Table 1. Because the hamstring tendon graft is soft and can transform its shape to match the shape of the tunnel, the graft could be passed through the rounded rectangular tunnel measuring 6 mm in the minor axis in all cases, even when the grafts were large. A femoral tunnel was created with a rounded rectangular shape at the center of the ACL’s anatomical femoral footprint using a rounded rectangular dilator with an inside-out technique. We preserved the remnant tissue on the femoral side for all patients in group P using a method that was similar to the method described by Tensho et al.
15
(Figure 2). In group P, using a thermal device with the knee flexed at 90°, the posterior part of the proximal end of the remnant tissue was peeled as little as possible but just enough to create a space through which the rounded rectangular dilator could be inserted. The remnant tissue that was attached to the proximal-posterior portion of the footprint of the ACL on the femoral side was then carefully peeled, and the rounded rectangular dilator was rotated to make it parallel to the intercondylar ridge (Figure 1(c)). In many cases, Crain type II or III remnant tissues were not attached to the anatomical area but were adhered to the roof or wall of the medial aspect of the lateral femoral condyle, which was anterior to the actual anatomical footprint. Consequently, the anatomical attachment could be confirmed after a small amount of peeling (Figure 1(d)). Once the remnant was peeled to some extent, the anatomical footprint of the ACL on the femoral side was checked from the anteromedial portal. The guide pin was then inserted from the far anteromedial portal while the knee was in deep flexion. We made a conventional round tunnel along the guide pin with a depth of 15 mm using a round drill that was 6 mm in diameter via the far anteromedial portal with the knee in the deep flexion position. The rounded rectangular tunnel was then dilated to a depth of 15 mm using a rounded rectangular dilator (Figure 1(e)). The long axis of the rectangular dilator was along the intercondylar ridge, and the angle of the dilator was confirmed using radiographic images (Figures 1(f) and (g)). The tibial tunnel was made using conventional round drills. The site of attachment of the ACL on the tibia was confirmed by probing. We usually identified the Parson’s knob to the anterior side and the medial intercondylar ridge to the medial side. The drill guide aimer for the tibia was set at an angle of 55°. We made a slit in the remnant tissue, and the tip of the aimer was positioned on the anteromedial part of the distal end of the remnant tissue. Drilling was carefully performed, in order to ensure that the remnant tissue was not damaged. The size of the tibial tunnel was determined based on the diameter of the graft using a conventional rounded sizing block. The hamstring tendon graft was fixed using a loop device, with an adjustable length, at the femoral site and a double spike plate and screw (Smith and Nephew, Andover, USA) at the tibial site. The initial graft tension was set to 40 N with the knee flexed at 20° (Figure 1(h)). Surgical methods for creating a rounded rectangular femoral tunnel with remnant tissue preservation. (a) We use rounded rectangular dilator depending on graft size. (b) Sizing block of the graft for the femoral side. (c) Using a thermal device, the posterior side of the proximal end of the remnant tissue, especially the remnant tissue that is attached to the proximal-posterior portion of ACL footprint (white arrowhead), is peeled to create space to insert a rounded rectangular dilator. (d) After only the posterior side of remnant tissue is peeled, the target point is confirmed (white arrow). (e) The tunnel is dilated up to a depth of 15 mm using a rounded rectangular dilator, and (f) the rotation of the dilator is confirmed by radiographic images. (g) The rounded rectangular femoral tunnel is created behind the ACL remnant. (h) The graft was transplanted with remnant preservation. Areas of the round and rounded rectangular bone tunnel. The size of the rounded rectangular tunnel is represented as the minor × major axis. Illustration of remnant-preserving ACL reconstruction with a rounded rectangular femoral tunnel of the left knee. From the sagittal view, ACL remnant on the femoral side covered the graft.

Rehabilitation was performed as previously reported. 8 Full range of motion and weight bearing were allowed depending on the patient’s pain on the day after the surgery, except for patients with complicated meniscal lesions. Jogging were allowed 3 months postoperatively if the quadriceps muscle strength was more than 70% of that of the contralateral leg when measured with a Biodex System 4 (Biodex Medical Systems, Shirley, NY, USA). Patients were generally allowed to play pivot motion 6 months postoperatively if the strength of the quadriceps muscle was more than 90% of that of the contralateral leg, and if the physical assessment results of the half-squat test and the single-leg hop test were good. Patients were allowed to return to sports 8–10 months postoperatively.
CT measurement for the femoral tunnel
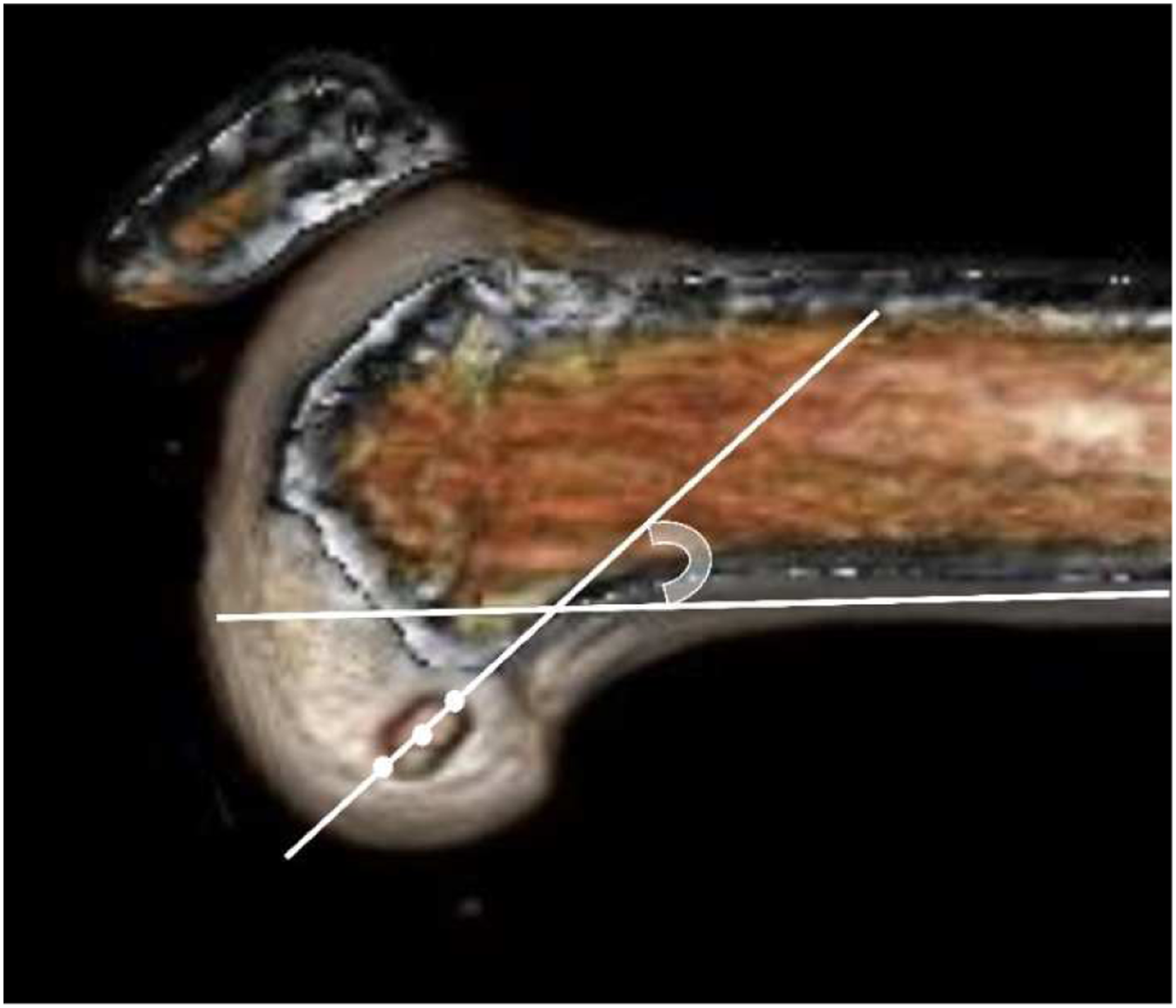
We used CT (LightSpeed VCT; GE Healthcare, Tokyo, Japan) to evaluate the effect of remnant tissue preservation on the creation of a rounded rectangular femoral tunnel. We obtained 0.6 mm thick cross-sectional images that were used to reconstruct the femur (without any soft tissue) using the AquarisNET (TeraRecon Inc. Foster City, CA, USA) program. Using the three-dimensional CT image, the center of the femoral tunnel was identified. We then compared the location of the tunnel, the rotation angle of the rounded rectangular femoral tunnel, and the graft bending angle (GBA). To locate the femoral tunnel, the 3D reconstruction was performed in a true lateral position and viewed from the medial side of the knee. A true medial view of the femur was established by superimposing the posterior aspects of the femoral condyles. The center of the femoral tunnel aperture was calculated using the quadrant method.16,17 In this method, four distances, namely, the distance of the lateral condyle on the sagittal plane along the Blumensaat’s line (t), the maximum intercondylar notch height perpendicular to the Blumensaat’s line (h), the distance from the center of the rounded rectangular femoral tunnel to the proximal border along line t (x), and the distance from the center of the femoral tunnel to the Blumensaat’s line (y) were measured (Figure 3). The ratios of “x:t” (deep/shallow) and “y:h” (high/low) were expressed as percentages to describe the position of the femoral tunnel. To evaluate whether the rotation of the rounded rectangular tunnel was reproducible, the rotation angle of the tunnel, defined as the angle between the long axis of the tunnel aperture and the line along the femoral posterior cortex on the 3DCT image, was assessed (Figure 4). The GBA was defined as the angle between the intra-articular graft and the femoral tunnel on the reconstructed coronal image (Figure 5).
18
Determining the center of the femoral tunnel. The quadrant method was used to determine the center of the femoral tunnel on three-dimensional computed tomography images. t: total length of the lateral condyle; h: maximum intercondylar notch height; x: distance from the center of the femoral tunnel to the proximal border along line t; and y: distance from the center of the femoral tunnel to the Blumensaat’s line. The rotation angle of the rounded rectangular femoral tunnel. The rotation angle of the rounded rectangular femoral tunnel is the angle between the long axis of the tunnel aperture and the line along the femoral posterior cortex on the 3DCT image. 3DCT, three-dimensional computed tomography The graft bending angle. The graft bending angle is the angle between the intra-articular graft and the femoral tunnel on the reconstructed coronal image.

Clinical assessment
We compared the postoperative outcomes, including the incidence of revision, postoperative residual instability, and subjective knee score, of the two groups. Anterior and rotational instability was evaluated using a KT-1000 arthrometer (MEDmetric, San Diego, CA) and the pivot shift test at the latest follow-up. The patients were assessed subjectively using the International Knee Documentation Committee (IKDC) knee score 19 and the Knee Injury and Osteoarthritis Outcome Score (KOOS) 20 1 year postoperatively.
Statistical analysis
Data are presented as mean and standard deviation. All measurements were analyzed using IBM SPSS Statistics, version 24.0 (IBM Corp., Armonk, NY, USA). According to the results of the Shapiro–Wilk test that was used to test the normality of the distribution, the age, height, body weight, body mass index, tunnel rotational angle, KT, IKDC score, KOOS were compared using the Mann–Whitney U. The chi-square test was used to compare sex, revision rate, and residual rotational instability, which was assessed with the pivot shift test. Tunnel location and the GBA were compared using the two-sample t test. We included 95% confidence interval (CI) to assess the magnitude of the differences in tunnel location and angle. The reproducibility of the rounded rectangular tunnel was assessed using Levene’s test, which compared the variance of the femoral tunnel position and angle between the two groups. The intra- (K.A.) and inter-(K.A and R.Y.) observer reliability of the measurements of the femoral tunnel location (deep/shallow and high/low), the tunnel rotation angle, and the GBA was determined using the intraclass correlation coefficient. A priori power analysis with a power of 0.80 and an alpha error of 0.05 revealed that 164 cases were needed to detect the difference in femoral tunnel assessment. A p-value of <.05 was considered significant.
Results
Patient characteristics.

Femoral tunnel location and angle
CT measurement of the rounded rectangular femoral tunnel.

Clinical assessment
Clinical assessment.
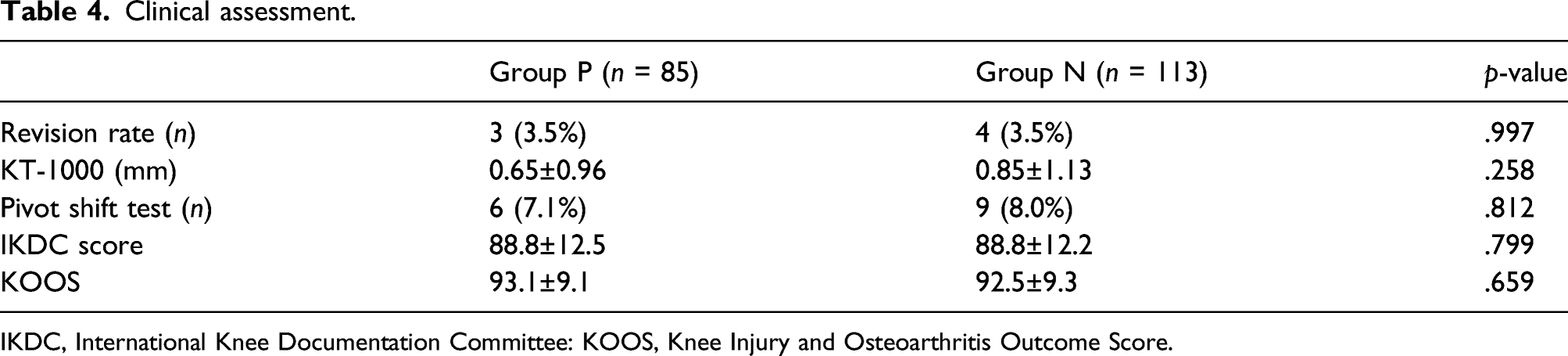
IKDC, International Knee Documentation Committee: KOOS, Knee Injury and Osteoarthritis Outcome Score.
Discussion
This study identified that there was a significant difference in the location of the femoral tunnel in the high/low direction between patients in whom the ACL remnant was preserved and those in whom it was not preserved. However, there were no significant differences in variations in the tunnel location and angle. Moreover, no case of blow out of the posterior wall of the medial aspect of the femoral lateral condyle was seen in the group in which the remnant was preserved. Therefore, a rounded rectangular femoral tunnel can be safely made and is highly reproducible if the remnant of the ACL is preserved.
Nakase et al. 8 reported the rounded rectangular femoral tunnel technique using a rounded rectangular dilator that can reproduce the native tendon-bone junction of the ACL, and performed an ACLR with a thicker graft. Oshima et al. 9 showed that the cross-sectional shape of the four-fold semitendinosus tendon was oval, not round. These findings suggested that the graft fitted better in a rounded rectangular femoral tunnel than in the conventional rounded tunnel. In this study, we used this technique even for small Asian women who had a narrow intercondylar space, even though this makes it difficult to locate the anatomical position of the femoral tunnel if a thick graft is used, because the optimal anatomical position and area directly posterior to the lateral intercondylar ridge are limited. There have been many cadaveric reports on the footprint of the ACL on the femur.21–23 Śmigielski et al.22,23 reported that the direct insertion of the ACL fibers had a ribbon-like appearance, which was continuous with the posterior femoral cortex. Nawabi et al. 21 reported that the ACL fibers located shallow within the femoral footprint bore more force during stability tests than the deep fibers. Creating a “shallower” femoral tunnel, just behind the lateral intercondylar ridge, during ACLR is advantageous. Theoretically, a rounded rectangular tunnel could be created along the intercondylar ridge. Graft tunnels placed outside the native ACL femoral footprint may result in loss of stability, abnormal graft tension patterns, and graft impingement at the roof of the intercondylar notch.24,25 A systematic review by Hu et al. 26 revealed that the theoretical centers of the ACL femoral tunnels were located at 28.4 ± 5.1% (x) and 35.7 ± 6.9% (y) as evaluated using the quadrant method. Following a recent questionnaire-based survey of 221 surgeons from 23 countries, the intended center of the ACL footprint was located at 27.0% (range, 18–39%; SD, 3.5%) in the deep/shallow direction and 31.4% (range, 18%–49%; SD, 5.5%) in the high/low direction. 27 This finding was in line with our current results. Therefore, the rounded rectangular femoral tunnel can be made within the native ACL footprint with the remnant tissue.
In this study, the femoral tunnel was located at a lower level in group P than in group N. This result was similar to that of a previous study that investigated remnant tissue behind double bundle ACLR. 13 We think that this was because the space between the remnant tissue and the proximal articular surface became smaller due to preservation of the remnant tissue. Koga et al. 13 showed that remnant tissue behind the femoral tunnel of the anteromedial bundle was made lower and deeper than the remnant non-preserved tunnel. In this study, there was no significant difference between the deep/shallow directions of the location of the femoral tunnel. This is because the femoral tunnel in this study was placed a little deeper in non-remnant preserved group, than what was previously reported (27.0–28.4%).26–28 The deeply placed femoral tunnel had a higher tension at full extension and became loose when the knee was flexed.13,29 However, this difference was very small. Furthermore, it is reasonable to create the rounded rectangular femoral tunnels a bit posterior to the native direct insertion site when using hamstring grafts, in view of tunnel enlargement and graft deviation. 10,30
In this study, the GBA was not influenced by the preservation of the remnant tissue during surgery. Many studies have reported a positive correlation between the GBA and higher stress at the proximal graft-bone interface on the femoral tunnel aperture, and this influences graft healing.18,31–33 Previous studies have reported a GBA of 56°–77° after a single-bundle ACLR which is consistent with our results (68.3 ± 8.5 in group P and 69.1 ± 8.3 in group N).18,31,33,34 Tashiro et al. 32 found that the GBA was affected by the surgical drilling technique. The GBA in the transportal technique was lower than that in the outside-in technique but higher than that in the transtibial technique. Previous studies on remnant-preserved ACLR reported the use of the outside-in or transtibial technique.13–15 To the best of our knowledge, this was the first report about remnant preserved ACLR using rounded rectangular femoral tunnel using the trans-portal technique.
Our hypothesis was validated, as creation of a rounded rectangular femoral tunnel was possible and reproducible even if the proximal end of the remnant tissue was preserved. Although this technique could be used for ACL injury with Crain type II and III remnant tissue, it is more suitable for cases with Crain type II remnant tissue. We considered some possible reasons for the high reproducibility of the femoral tunnel using our technique. Koga et al. 13 showed that the posterior border of the direct insertion, as well as the posterior articular surface, served as landmarks that enabled surgeons to create highly reproducible femoral tunnels when remnant preserved ACLR was performed. The other reason may be that the location of the femoral tunnel and rotation of the rounded rectangular femoral dilator were confirmed on intraoperative radiographic images. Of course, the rigid loop device also could be used for this technique.
The effect of preserving the remnant tissue on clinical outcomes remains controversial. Many studies have reported improved knee laxity and proprioception, revascularization, and synovial coverage of the reconstructed ACL.4–7 However, other surgeons have found no benefits of preserving the remnant tissue on clinical outcomes.35,36 There were also no significant differences in the clinical outcomes of the two groups in this study. More recent meta-analyses have shown slightly better postoperative knee stability and clinical scores following ACLR wherein the remnant tissue was preserved.28,37 The biological effects of preserving the remnant tissue have been attracting attention. Some studies have reported that the remnant tissue expressed various types of collagen, CD34+ cells, and other genes.38,39 However, it is still unclear whether these biological effects influence clinical outcomes.
Our study has some limitations. First, group N included cases wherein the proximal end of the remnant tissue was excised because of poor continuity as it was likely to be damaged because of intraoperative procedures, such as graft insertion, even if it was not excised. This could have introduced a potential selection bias. Second, the tunnel might slightly enlarge postoperatively, and this could influence all measurements. To minimize the effects of femoral tunnel enlargement on all measurements, 3DCT images taken 1 week postoperatively were used in this study. Third, the correlation between the intercondylar ridge and the rounded rectangular femoral tunnel was not evaluated. Since no preoperative CT imaging was performed in this study, it was difficult to compare and detect the intercondylar ridge on the CT image taken 1 week postoperatively. Finally, the morphology of the Blumensaat’s line has been reported to vary, and this variation can influence the results of the quadrant method. 40 As mentioned above, the intra- and inter-observer reliability for the tunnel location was all high agreement.
The results of this study showed that a surgeon can reproducibly create a rounded rectangular femoral tunnel even if remnant tissue was preserved. However, it should be noted that the tunnel should be created in a slightly lower position.
Conclusions
The remnant preservation approach creates a lower femoral tunnel compared to non-preservation technique. However, a rounded rectangular femoral tunnel can be created reproducibly and safely with remnant tissue preservation.
Footnotes
Authors’ contributions
Study design: J.N., K.A., H.T. Recruitment and data collection: J.N., K.A., R.Y., M.K. Data analysis and interpretation: J.N., K.A. First draft of paper: K.A. Revision of paper: All authors. All the author(s) have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.