
Abstract
Purpose:
The correlation between the graft bending angle (GBA) of the anteromedial bundle and posterolateral bundle after anterior cruciate ligament reconstruction (ACLR) and postoperative tunnel enlargement was evaluated.
Methods:
Two hundred fifty-eight patients (137 males, 121 females; mean age 27.3 years) who had undergone double-bundle ACLR were included. Computed tomographic scans of the operated knee were obtained at 2 weeks and 6 months postoperatively. The area of the tunnel aperture for femoral anteromedial tunnel (FAMT) and femoral posterolateral tunnel (FPLT) was measured; the area at 2 weeks after ACLR was subtracted from the area at 6 months after ACLR and then divided by the area at 2 weeks after ACLR. The femoral tunnel angles were obtained with Cobb angle measurements. The femoral tunnel angle in the coronal plane was measured relative to the tibial plateau (coronal GBA). On the median value, the patients were divided into two groups in each of FAMT and FPLT; those with a coronal GBA of FAMT of ≥27° were classified as group A, while those with a coronal GBA of <27° were classified as group B, those with a coronal GBA of FPLT of ≥23° were classified as group C, while those with a coronal GBA of<23° were classified as group D.
Results:
Group A included 129 knees, while group B included 129 knees. Groups A and B did not significantly differ regarding FAMT enlargement. Group C included 133 knees, while group D included 125 knees. The percentage of FPLT enlargement in group C was significantly smaller than that in group D (p = 0.001).
Conclusions:
A steep coronal GBA of the FPLT after ACLR results in greater FPLT enlargement. The present findings suggest that surgeons should avoid creating a steep GBA of the FPLT in the outside-in technique.
Keywords
Introduction
Recent biomechanical studies have revealed that double-bundle (DB) anterior cruciate ligament (ACL) reconstruction (ACLR), which replicates both the anteromedial (AM) bundle (AMB) and the posterolateral (PL) bundle (PLB) of the native ACL, restores more normal knee biomechanics than traditional single-bundle reconstructions, especially in response to rotatory loading. 1 A steep graft bending angle (GBA) has been recently proposed as a biomechanical factor that could contribute to poor graft healing or graft damage. 2 This may be particularly important in ACLR via the outside-in technique, as the intra-articular aperture is more acute in the outside-in technique compared with the transportal technique. 3
A common complication after ACLR with hamstring autografts is bone tunnel enlargement. 4 –6 The presence of large tunnels often severely complicates revision ACLR surgery and may necessitate staged reconstruction and additional operative procedures that are associated with marked costs. 5 Thus, methods that reduce the risk of tunnel widening after ACLR are needed. 7,8 Tunnel widening likely occurs due to a complex interplay between mechanical and biological factors. The reported mechanical factors include the “bungee effect” due to extracortical femoral fixation 9,10 and bone tunnel positioning, 11 –13 while the biological factors include synovial fluid-derived cytokines and inflammatory mediators, bone quality, graft choice, and cell necrosis from drilling. 4,12,14 –18 Significant postoperative bone tunnel widening occurs at all four bone tunnels, with the greatest amount of widening occurring in the PLB tunnel. 8,19,20
The aim of the present study was to investigate the correlation between the GBA after DB ACLR and postoperative tunnel enlargement. To the best of our knowledge, this is the first study to investigate the correlation between postoperative AMB tunnel and PLB tunnel enlargement after DB ACLR (using the hamstring tendon) and the GBA.
Materials and methods
Two hundred ten consecutive patients with ACL-deficient knees, who underwent DB ACLR between 2013 and 2016, were evaluated. Patients who underwent bilateral ACLR, those with an open physis and those with a concomitant grade 3 injury of the medial or lateral collateral ligament, were excluded from the study; 22 of 280 patients (7.8%) were excluded. The final study population included 137 males and 121 females. The average time period between injury and surgery was 33.7 weeks (range 1–504 weeks). The Institutional Review Board of our institution approved this study (approval no. 2019010903). Informed consent was obtained from all individual participants included in the study.
Surgical procedure for DB ACLR
Anatomic DB ACLR was performed using a hamstring tendon, as previously described. 1 If the diameter of either the AM or PL graft was <5 mm, the gracilis tendons were added. An EndoButton CL device (Smith & Nephew Endoscopy, Andover, Massachusetts, USA) was attached at the looped end, and a Telos artificial ligament (Telos, Marburg, Germany) was attached at the other end.
Femoral tunnels were made behind the resident’s ridge, just anterior to the cartilage margin. The outside-in technique was used to create the AM and PL tunnels.
The tibial AM tunnel insertion was lateral to the medial intercondylar ridge and posterior to the transverse ligament or Parsons’ knob at 90° of knee flexion. A 2.4-mm guidewire was inserted into the AM tunnel, and a 5.0–7.0 mm tunnel was then drilled over the guidewire. A 2.4-mm guidewire for the PL tunnel was then inserted slightly PL to the AM tunnel. Stapling for graft fixation was performed on the tibial side at 30° of knee flexion. Tibial fixation of the AMB and PLB was carried out with 30 N of traction applied to each bundle.
Postoperative rehabilitation
A continuous passive motion machine was used from postoperative day 2. Partial weight-bearing activity (one-third of the patient’s body weight) was permitted from postoperative week 2. Full-body weight-bearing was permitted from postoperative week 4. Jogging was started from 4 months postoperatively. Full-speed running was allowed at 6 months postoperatively. A complete return to competitive sports was allowed at 8 months postoperatively.
Postoperative evaluation
A clinical examination was performed at 1 year postoperatively (range 11.7–13.8 months postoperatively) in all cases. The side-to-side difference in the anterior translation was investigated using a Telos device, and the Tegner activity score was determined. 21
Computed tomographic evaluation
Area measurement
Computed tomography (CT) scans of the operated knee were obtained at 2 weeks postoperatively (range 2–2.4 weeks postoperatively) and at 6 months postoperatively (range 5.8–7.2 months postoperatively) for all patients using a helical high-speed scanner (SCENARIA, Hitachi Medical Systems, Tokyo, Japan). The settings were as follows: collimation 16 × 0.625 mm, tube parameters 175 mA and 120 kV, acquisition matrix 512 × 512, field-of-view 140 mm, and slice thickness 0.5 mm. The images were evaluated, and the cross-sectional data were obtained using a software package (VOX BASE; J-MAC, Tokyo, Japan). Cross-sectional measurements were calculated, as previously described. 8,20,22 The CT scout view was used (at a level parallel to the outer rim of the lateral femoral condyle and the intercondylar fossa of the tibia). Sagittal reconstruction was performed at a level parallel to the outer rim of the lateral femoral condyle; the femoral bone tunnel area was measured as the cross-sectional area of a 2-mm deep slice made near the opening of the femoral bone tunnel (Figure 1). The tunnel wall was traced within the bony margin, and the area surrounded by trace lines was measured as the cross-sectional area of the tunnel in mm2 to the first decimal place. To calculate the percentage of tunnel area enlargement, the area at 2 weeks after ACLR was subtracted from the area at 6 months after ACLR, and the resultant value was divided by the area at 2 weeks after ACLR.
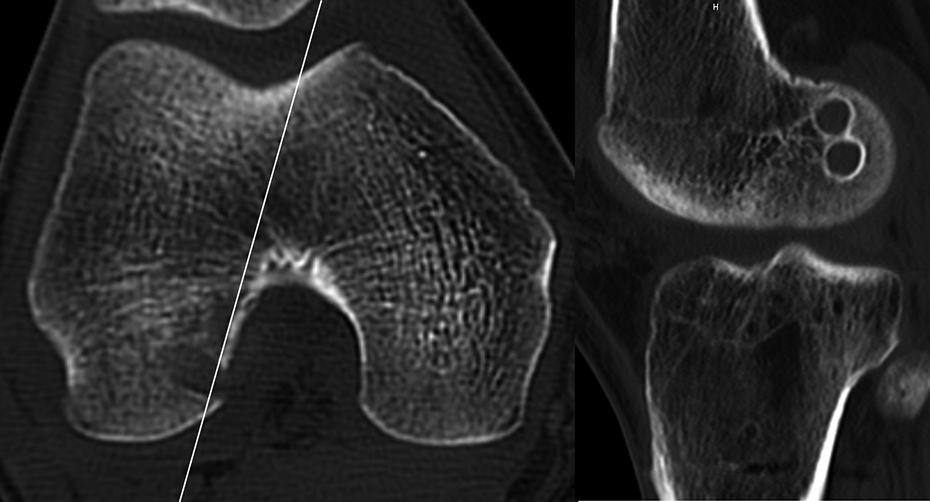
Sagittal reconstruction was performed at a level parallel to the outer rim of the lateral femoral condyle. The cross-sectional bone tunnel area was measured on a 2-mm deep slice made near the opening of the femoral bone tunnel.
Reliability calculations were made based on the cross-sectional area measurements. Two orthopedic surgeons (SY and KH) jointly developed and agreed to the measurement methods; however, they were blinded to each other’s measurements and their own previous measurements. Analyses of the intraclass correlation coefficients revealed an intraobserver reliability of 0.938 (95% CI 0.772–0.984) and an interobserver reliability of 0.907 (95% CI 0.671–0.976). Tunnel locations
At 2 weeks postoperatively, the femoral tunnel position was measured by the femoral quadrant method using three-dimensional (3-D) CT. The location of the centre of the femoral tunnel was defined as the percentage of the distance from the most posterior contour with respect to the total length of the lateral condyle parallel to Blumensaat’s line and the percentage of the distance from the intercondylar roof with respect to the total depth of the intercondylar notch perpendicular to Blumensaat’s line (Figure 2). 23 The tibial tunnel position was measured by the tibial quadrant method using 3-D CT. The location of the centre of the tibial tunnel was defined as the percentage of the distance from the most medial contour with respect to the mediolateral width of the tibial plateau and the percentage of the distance from the most anterior contour with respect to the anteroposterior length of the tibial plateau (Figure 3). 23

The location of the center of the femoral tunnel was defined as the percentage of the distance from the most posterior contour with respect to the total length of the lateral condyle parallel to Blumensaat’s line and the percentage of the distance from the intercondylar roof with respect to the total depth of the intercondylar notch perpendicular to Blumensaat’s line.

The location of the centre of the tibial tunnel was defined as the percentage of the distance from the most medial contour with respect to the mediolateral (ML) width of the tibial plateau and the percentage of the distance from the most anterior contour with respect to the anteroposterior (AP) length of the tibial plateau.
GBA measurement
The femoral tunnel angles were obtained with Cobb angle measurements. The femoral tunnel angle in the coronal plane was measured relative to the tibial plateau (coronal GBA). The measurement was performed with the knee in extension (Figure 4). 2

The femoral tunnel angle in the coronal plane was measured relative to the tibial plateau (coronal graft bending angle).
Based on the median coronal GBA value, the patients were divided into two groups in each of femoral AM tunnel (FAMT) and femoral PL tunnel (FPLT); those with a coronal GBA of FAMT of ≥27° were classified as group A, while those with a coronal GBA of <27° were classified as group B, those with a coronal GBA of FPLT of ≥23° were classified as group C, while those with a coronal GBA of <23° were classified as group D.
Statistical analyses
Spearman’s correlation coefficients were calculated. The differences between groups A and B were evaluated using χ 2 test for categorical variables and the parametric two-sample t-test and the nonparametric Mann–Whitney U-test for continuous variables. A power analysis was performed based on a previous study 20 using G*Power 3.1. 24 The mean FPLT enlargement and standard deviation were calculated for patients aged <40 and ≥40 years. With an effect size of 0.39, an α of 0.05, and a minimum of 218 subjects, the power of the current study is 0.8.
Results
The percentage of FAMT enlargement was not correlated with the coronal GBA of the FAMT (r = −0.04; p = 0.52), while the percentage of FPLT enlargement was correlated with the coronal GBA of the FPLT (r = −0.28; p = 0.03).
Group A included 129 knees, while group B included 129 knees. Groups A and B did not significantly differ regarding sex, age, body mass index (BMI), time between injury and surgery, pre- and postoperative Tegner activity score (TAS), Lysholm score, pivot shift test, and percentages of tunnel enlargement (Table 1).
Clinical findings in groups A and B.a

BMI: body mass index; SSD: side-to-side difference; FAMT: femoral anteromedial tunnel; FPLT: femoral posterolateral tunnel; TAMT: tibial anteromedial tunnel; TPLT: tibial posterolateral tunnel; CT: computed tomography; n.s.: not significant.
a Data are presented as the mean ± standard deviation or median [minimum, maximum].
Group C included 133 knees, while group D included 125 knees. Sex, age, BMI, time between injury and surgery, preoperative and postoperative TAS, Lysholm score, and pivot shift test were not significantly different. Compared with group D, group C had significantly smaller percentages of FPLT enlargement (p = 0.001; Table 2).
Clinical findings in groups C and D.a

BMI: body mass index; SSD: side-to-side difference; FAMT: femoral anteromedial tunnel; FPLT: femoral posterolateral tunnel; TAMT: tibial anteromedial tunnel; TPLT: tibial posterolateral tunnel; CT: computed tomography; n.s.: not significant.
a Data are presented as the mean ± standard deviation or median [minimum, maximum].
Discussion
The most important finding of the present study was that if the coronal GBA of the FPLT was steep, the percentage of FPLT enlargement was large. Previous studies have reported that the GBA is significantly correlated with the femoral intraosseous graft maturation after ACLR using the outside-in technique 2 and that a steep GBA may negatively affect proximal graft healing after ACLR. 25
Bone tunnel enlargement after ACLR is a recognized complication; however, the mechanism of bone tunnel enlargement is not fully understood. Tunnel enlargement occurs due to a complex interplay of biological and mechanical factors. Mechanical factors considered to affect tunnel enlargement include nonanatomic tunnel placement, 11 –13 micromotion at the tunnel aperture when soft tissue grafts are used with suspensory fixation, 5 increased stress at the tunnel–graft interface, 25 and aggressive rehabilitation. 26 Furthermore, Tomihara et al. reported that the creation of a femoral aperture with a sharp edge due to a steep GBA of the PLB results in abrasive force and repetitive bending, which causes excessive mechanical stress on the bone–graft interface and may result in tunnel enlargement of the femoral PLB. 27
Shin et al. reported that the tunnel length in patients with a mild GBA is increased compared with the tunnel length in those with a steep GBA. 28 The creation of a fixation point that is a long distance from the joint line leads to tunnel enlargement due to the “bungee cord effect.” 10 Thus, an excessively mild GBA should be avoided; although our study did not investigate the acceptable range of mild GBA, the present results suggest that a GBA of less than 23° should be avoided.
Previous studies evaluating DB ACLR using the outside-in technique have reported mean widenings of the FPLT of 30.8% 29 and 46.4%. 19 In the present study, the amount of tunnel widening was larger than that reported in the abovementioned studies. This may be because we assessed the widening using serial CT scans, whereas the abovementioned studies evaluated the difference between the area measured on the last follow-up image and the diameter of the intraoperative reamer. Although previous studies have reported the percentage tunnel enlargement using the outside-in technique, 19,29 an acceptable limit for percentage tunnel enlargement has not been reported in the literature.
The morphological change at the tunnel aperture is reportedly not limited to any specific direction, and the tunnel enlargement occurs in all directions. 30 Furthermore, femoral tunnel enlargement after ACLR occurs at the aperture, but not in the middle, of the femoral tunnel. 23 Hence, we evaluated bone tunnel enlargement at the tunnel aperture.
Bone tunnel enlargement also depends on the positioning of the bone tunnel, 11,13 with a more anterior and higher femoral tunnel position associated with greater widening of the femoral tunnel. 11 In the present study, there were no significant differences in the tunnel positions of the two groups.
Weber et al. 31 reported that the apertures of both the tibial and femoral tunnels generally increase until postoperative week 24. Thus, we examined CT scans of the operated knee that were obtained at 2 weeks and 6 months postoperatively. In addition, this timing for the follow-up CT scans was chosen considering the influence of each patient’s physical size.
The present study had several limitations. First, the patients’ bone mineral density, which might have affected tunnel enlargement, was not assessed. Second, the follow-up period was relatively short at only 6 months; however, tunnel enlargement is reportedly generally maximally increased by postoperative week 24. 31 Third, the lack of significant differences between groups for some parameters may have been due to the low statistical power of the present study. Fourth, tunnel enlargement was evaluated on two-dimensional CT rather than on 3-D CT. Recent studies have shown that 3-D CT might be beneficial for evaluating the size of bone tunnels after ACLR. 32,33 Fifth, no comparisons were made with other groups of patients, such as those undergoing anatomic single-bundle ACLR or patients in whom interference screw fixation techniques were applied. Sixth, differences in postoperative activity levels may have affected the development of tunnel enlargement.
To the best of our knowledge, this is the first study to investigate the correlation between PLB tunnel enlargement after DB ACLR (using the hamstring tendon) and the GBA. When the coronal GBA of the FPLT was steep, the percentage of FPLT enlargement was large. The strength of the present study was the comparability of the two groups in terms of sex, type of graft, surgical technique, and rehabilitation program. The present findings suggest the need for surgeons to avoid creating a steep GBA of the FPLT in ACLR using the outside-in technique.
Conclusion
The percentage of enlargement of the FPLT was associated with the GBA in DB ACLR using hamstring tendon autografts.
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.