
Abstract
Purpose
This study aimed to compare the biomechanical pull-out strength of the three different tension band wiring (TBW) methods employed to fix transverse olecranon fractures on bone models.
Methods
Three different fixation models were created in groups of seven synthetic olecranon fractured bone models. The first technique was fixed the olecranon with the traditional TBW method. The second technique was fixed the olecranon with a large intramedullary screw TBW method. The third technique was fixed the olecranon with the double-screw TBW method. The pull-out force needed for the failure of each specimen under the tensile test device was evaluated, and the results were recorded.
Results
We found that the lowest average pull out strength was 55.10 N (range: 35.87–65.85 ± 10.17) in the traditional TBW method, the highest pull out strength was 84.28 N (range: 63.67–117 ± 18.87) in the double-screw TBW method. The pull out strength was 70.80 N (range: 52.60–80.95 ± 10.18) in the intramedullary screw TBW method. In terms of ultimate failure loads, there was no significant difference between the intramedullary screw TBW and the double-screw TBW (p > .05) while there was a significant difference between the traditional TBW and the other two methods (p < .05).
Conclusion
The use of screw(s) shows higher biomechanical stability than K-wires in the TBW method. Double-screws fixation gives similar results in terms of the biomechanical load to failure compared to a large intramedullary screw fixation. Both screw methods can be used as stable constructs in clinical practice.
Level of Evidence
III, biomechanical trial.
Introduction
Olecranon fractures are observed almost 10% of upper extremity fractures in adults. 1 Simple displaced transverse fractures are common injuries located in the Mayo type 2 classification, including 85% of all the olecranon fractures.2,3 In surgical treatment, open anatomic reduction and internal fixation have been found effective in regaining the triceps extensor force. 4 A variety of fixation techniques are performed in such surgical practices as tension-band wiring, plate fixation, and intramedullary screwing. 5
Weber presented the tension band wiring (TBW) technique in 1963, and Pauwels ascertained the biomechanical principles of TBW in 1935.6,7 TBW is the traditional practice which is the most widely used and recommended by the AO group for olecranon transverse fracture (Arbeitsgemeinschaft fur Osteosynthesefragen and Orthopaedic Trauma Association [AO/OTA] class 21-B1.1).8,9 The TBW converts to tensile forces into compression forces and improves healing during elbow during active extension. 7 In general, the traditional TBW method can be applied in two different ways. Two Kirschner wires (K-wires) can be placed in the proximal ulna, either the intramedullary or trans-cortical ways. 10 Although the traditional TBW method mostly yields promising results, complications can be observed during this process. There is evidence which suggests that the intramedullary placement of K-wires may cause skin irritation due to the migration prominence of pins. At the same time, the risk of damage to the neurovascular structures and impairs forearm rotation may stem from the trans-cortical placement of K-wires.1,8,11 A review of previous literature on comparing the placement of the K-wires has resulted in contradictory findings about the removal of hardware.12,13 Still, hardware removal has been reported as a range from 40% to 92% in the traditional TBW method.14,15
Considering the complications related to the use of K-wires, the use of screw(s) is also another logical option in the TBW method. The screw used in the TBW method is often practiced via a large intramedullary screw. In addition to a large intramedullary screw fixation, authors have performed a different method of using a new double cannulated screws technique in the TBW method. 16 The use of the screw(s) plus the TBW method is associated with a low rate of removal hardware (<10%), and it is considered a safe way for the treatment of transverse olecranon fractures.17,18
Increasing construct stability reduces complications due to the low rate of implant failure. The best our knowledge, existing biomechanical studies have focused on the comparison of traditional TBW and intramedullary screw TBW while none of these studies taking into account the use of double-screws TBW. The comparison among these can provide new insights into the fixation of transverse olecranon fractures. The contribution of this study is to test the effectiveness of three different models and draw some conclusions. In this sense, the core purpose of this study was to compare the mechanical properties of three different techniques employed to fix transverse olecranon fractures (AO/OTA 21-B1.1) in the TBW method: (1) traditional, (2) intramedullary screw, and (3) double-screws. Based on this primary objective, we hypothesized that double-screw TBW would develop the lowest rate of implant failure and increased the stability of the construct as compared to the intramedullary screw TBW and traditional TBW.
Methods
Creating models
Twenty-one left ulna bone models (Synbone®, Malans, Switzerland) with transverse olecranon fractures (AO/OTA class 21-B1.1) were fixed by a single orthopedic surgeon and created three different models in groups of 7. Features of the ulna model were the length of 264 mm, the shaft diameter of 12 mm.
Olecranon fractures fixed to the traditional TBW method classified as group A. Firstly, the olecranon fracture was reduced and maintained by using two towel clamps: one for rotation control of the distal fragment and the other for antigliding and compression of the fracture line. Later, two parallel 1.6 mm K-wires were inserted tangentially just below the joint surface until the pins engaged the anterior cortex of the proximal ulna approximately 40 mm distal of the fracture line and 5 mm from the posterior cortex of ulna drilled a hole. After that, cerclage wire was passed through the drill hole. The cerclage wire was wrapped in the figure of-8 pattern put over the proximal ends of the k-wires and tensioned tightly with standard single knot technique. Finally, the tips of the K-wires were bent 180° using pliers and inserted end of pins into the sawbones (Figure 1). Photograph of a traditional TBW test model (a). Anteroposterior direct (b) and Lateral X-ray (c) views of traditional TBW.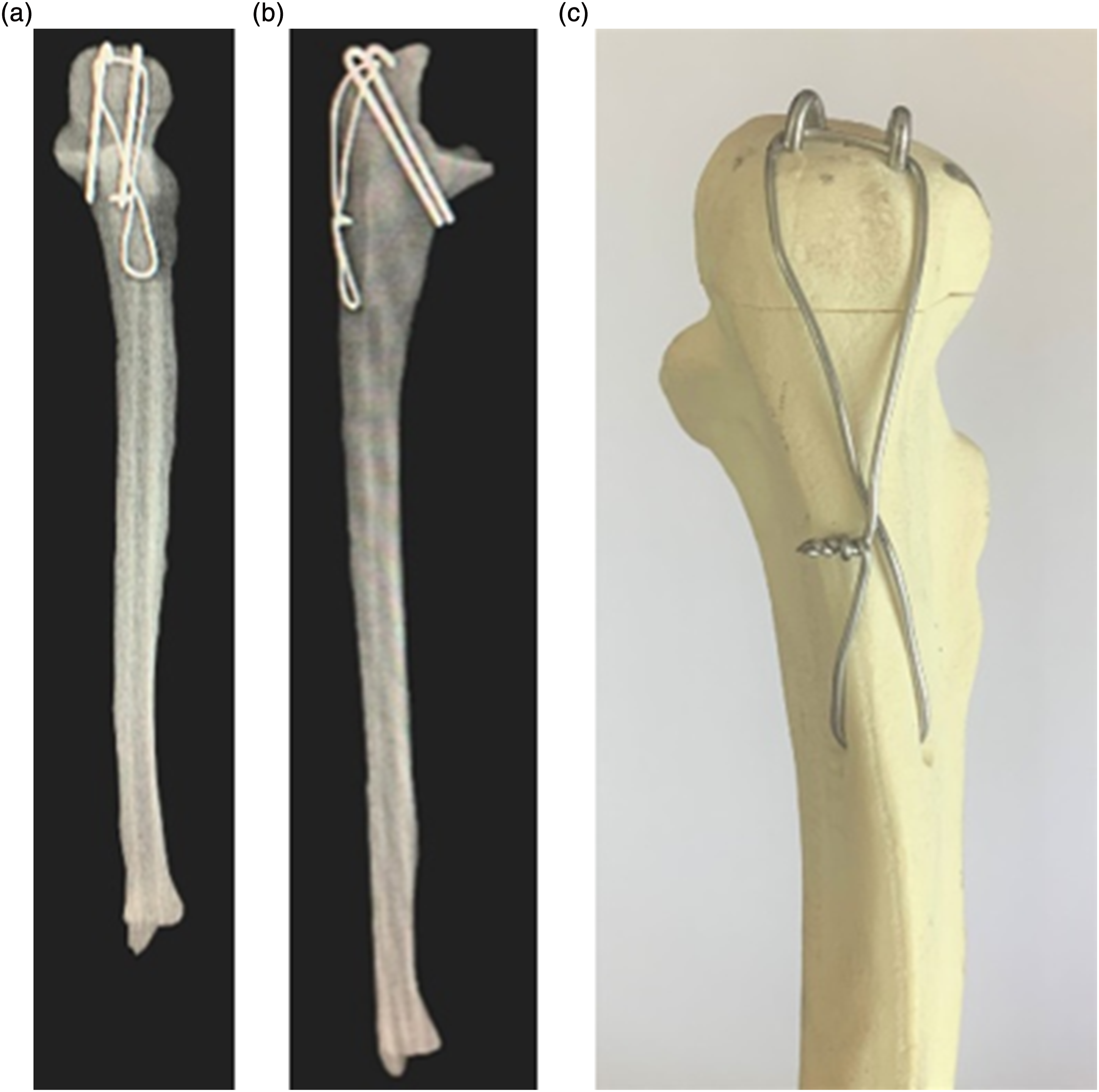
Olecranon fractures fixed to a large intramedullary screw TBW method described as group B. First, the olecranon fracture line was accurately reduced using small pointed reduction clamps. Next, a 2.8 mm K-wire was inserted from the center point of the olecranon tip into the medullary canal to guide the cannulated screw. Then, the top of the olecranon cortex was drilled. A 6.5 mm diameter partially threaded cannulated screw was sent over the K-wire without doing full compression between the screw head and the bone surface. After that, the distal ulnar hole was created as similar to group A. The cerclage wire was passed through the hole just below the screw head. Eventually, the cerclage wire was formed in the figure of-8 pattern and tensioned tightly with a standard 1-knot technique using pliers at the same time the screw was tightened to allow the full compression (Figure 2). Photograph of a 6.5 mm partially intramedullary cannulated screw TBW test model (a). Anteroposterior direct (b) and Lateral X-ray (c) views of intramedullary screw TBW.
Olecranon fractures fixed to the double-screw TBW method named group C.
16
Initially, the olecranon fracture line was reduced like the other two methods. Two parallel 1.6 mm double-guide K-wire was inserted tangentially at a 20° angle with the longitudinal axis of ulna from the tip of the olecranon into the posterior ulna cortex. The guide pins of suitable length engaged the posterior ulna, and drilling was performed over the pins. Following that, a spaced of approximately 10 mm between two 4.5 mm diameter partially threaded cannulated screws were inserted of penetrating the posterior ulnar cortex over the guide pins. The cerclage wire was passed through double-cannulated screws to cross over. Ultimately, it was tensioned by pulling on a side like the traditional TBW method (Figure 3). Photograph of a double 4.5 mm partially threaded cannulated screws TBW test model (a). Anteroposterior direct (b) and Lateral X-ray (c) views of double-cannulated screws TBW.
Biomechanical testing
Each model underwent tensile tests with the MakroXtens II extensometer using a universal electronic material testing device (Z330, Zwick/Roell, Germany) with a 5 kN ± 0.2 tension/compression load cell, randomly. To simulate the impact failure in biomechanical tests, the normal stretching speed to which the bone is exposed can be selected as 0.01–10 mm/s. All specimens were loaded under displacement control at a rate of 0.2 mm/second until catastrophic failure.
To simulate the triceps muscle insertion, a 2 mm wide tunnel was opened to the olecranon tip, and the steel wire was passed through the hole. The distal ulna was placed into the iron tube using the 3-component epoxy resin-based grout to adhere to the models. Models were placed on the test device vertically, as in a previous study.
19
The proximal aspect of the models was fixed to the upper jaw via steel wire, and the iron tube was placed in the hydraulic jaw (Figure 4). The pull-out force was simulated by pulling the connection point of the steel wire. The test was canceled when the implant system failed either bone model or hardware. Test setup with the TBW of the proximal ulna under the uniaxial tension testing system (Zwick/Roell ®).
Statistical analyses
The maximum force data were analyzed with the failure test of the surgical methods used in olecranon fractures (ver. 21.0; SPSS Inc., Chicago, IL, ABD). In the analysis, p < .05 was accepted as statistically significant. Kolmogorov-Smirnov test was used to evaluate the normality of the distribution. While group A and group C showed normal distribution, group B not normally distributed. Therefore, comparisons between groups were performed using the Mann-Whitney-U Test.
Results
Descriptive values of the bone models.

Statistical analysis of the maximum strength between the fixation methods.

*p < .05.
Discussion
The present study aimed to investigate the biomechanical pull-out strength of the three different TBW methods to answer whether a double-cannulated screws TBW fixation is more stable or not.
The use of a large intramedullary screw or double-cannulated screws in TBW significantly increased the stability of construct compared with the use of two trans-cortical placement of K-wires fixation (p < .05). Although the double-screw provided a higher ultimate load to failure compared to the intramedullary screw, no significant difference between these two methods (p > .05) was observed. The outcomes of this study were not as satisfactory as expected.
The main target in the surgery of olecranon fractures is to restore the anatomical construction and maintain sufficient absolute stability. 20 The tension band wiring method is the gold standard for treating non-comminuted olecranon fractures. The traditional tension band technique involves the use of two intramedullary K-wires plus wiring. The main challenge of the intramedullary placement of K-wires is the instability of the construct. 21 This instability might result in complications such as proximal migration of the pins, fracture line displacement, and unstable construct, which can cause osteoarthritis in the long-term follow-up. 22 Therefore, the traditional method has been modified by using the trans-cortical placement of K-wires instead of the intramedullary. Even though this modification was promising, comparative studies shown controversial results. For instance, Van et al. 22 demonstrated that fewer complications and removal of metal rate in the trans-cortical placement of K-wires. In contrast, Chan et al. 13 did not report any significant difference in fixation metalwork removal rates. Another study found that the proximal bent end of pins inserted in the cortex of the olecranon creates extra stability. 19 In their study, the biomechanical pull-out strength of the bi and tricortical K-wire fixation with tension band wiring method was compared. The results represented that the tricortical K-wire fixation was biomechanically superior. 19 Despite all these modification methods, in tension band wiring method performed with K-wires has a high reported removal rate independently the position of the pins.23,24
The screw(s) with or without the tension band is employed instead of the pins to increase the construct stability in the transverse olecranon fractures. Also, the use of screws provides more compression and resistance in the fracture line. 25 Hahn et al. 26 illustrated that a higher implant failure in the conventional method compared with the intramedullary screw in a cadaveric study. Raju et al. 27 evaluated the clinical outcomes of 25 patients of olecranon fractures treated with AO cancellous screws plus TBW, and there were no poor clinical results. Metal prominence was noticed in only one patient. In a biomechanical study, Murphy et al. 25 compared four different tension band wiring methods; the figure of eight cerclage wire, a 6.5 cancellous screw, a 6.5 cancellous screw plus wire, and AO tension band. They concluded that cancellous screw plus wire provided the greatest strength of fixation compared to other techniques. In addition to a large intramedullary screw fixation, the double-cannulated screws plus tension band, which is a novel technique defined by Lu et al., 28 has been investigated in the lately published study. They reported that symptomatic prominence of the metalwork at nine cases (45%) of the traditional method and two patients (4%) of the double-cannulated screws method. The study was concluded that double-cannulated screws could significantly decrease complications and lower re-operation rate compared with the conventional method. 28
The fundamental limitation of the study was related that implants do not reflect real conditions in biomechanical research with saw bone. Secondly, the study was addressed to a simple fracture type. Thirdly, the compression and displacement values of the fracture line were disregarded. Moreover, incorrect anatomic traction direction was ignored since the effect of the comparative results in terms of biomechanical constructional stability were insignificant. Future studies may be required to focuse on a comparative clinical study to reflect the actual situations about this subject.
Conclusion
In general, a stable construct minimizes complications such as removable hardware, gap appearance, and symptomatic prominence of the metalwork. Screw(s) with tension band provides superior construct stability as compared to the AO tension band technique on bone models. Double-screw fixation gives similar results in terms of the biomechanical load to failure compared to a large intramedullary screw fixation. Both screw methods can be used as stable constructs in clinical practice.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Amasya Üniversitesi (FMB-BAP 19-0400).